Director of Medical Affairs @Labcorp Oncology. Breast Medical Oncologist. Former Hem/Onc Fellow @MontefioreNYC. Former resident @UTHimres. Alum @UNC. #BCSM
Congrats to Elsa- so well-deserved!
In recognition of all her great ctDNA work we should rename tissue-agnostic MRD approaches to tissue-Anagnostic ones!😉
@PGrivasMDPhD
When I moved to the US in 2021, breast oncology was very different. With 2025 coming to an end, I decided to look back and review 10 major milestones in BC medical oncology care we saw over the past 5 years. With hope and expectation to see so much more unfolding over the next 5!
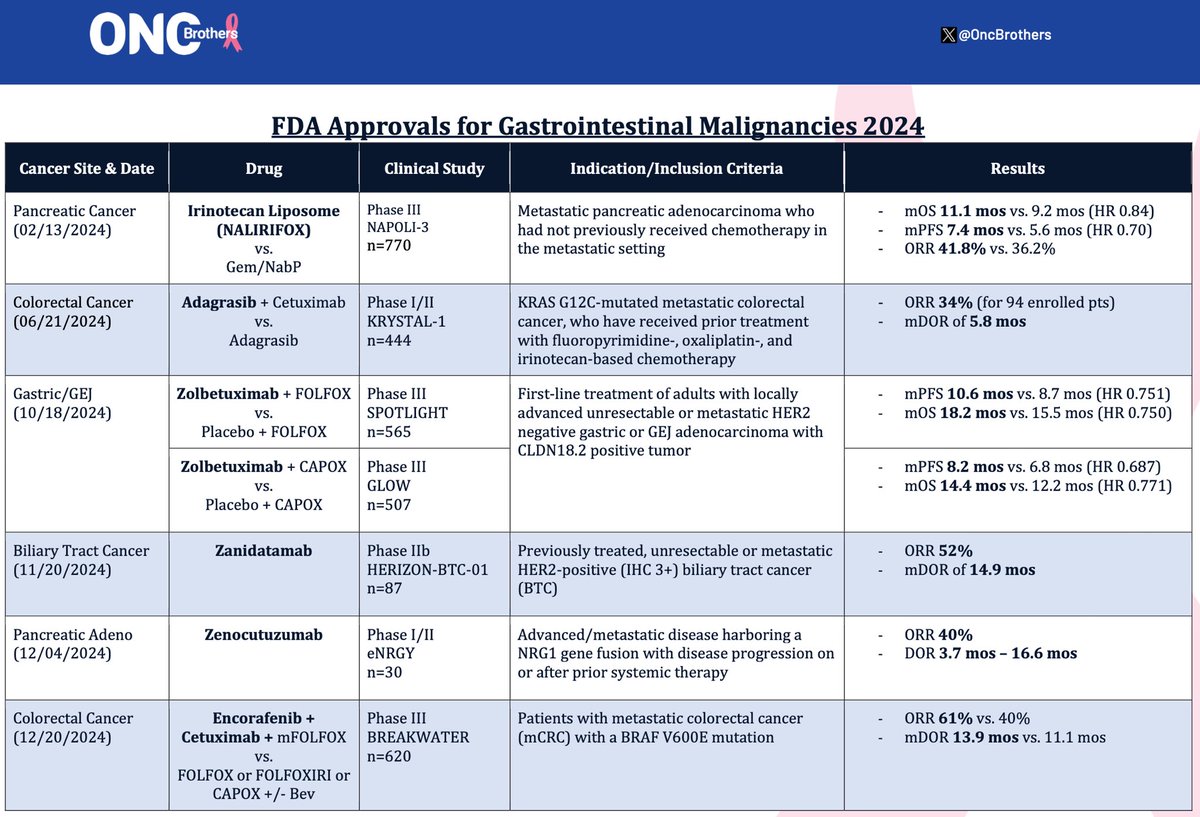
ASCO GI is upon us.
The data leakage has begun 👀🔥
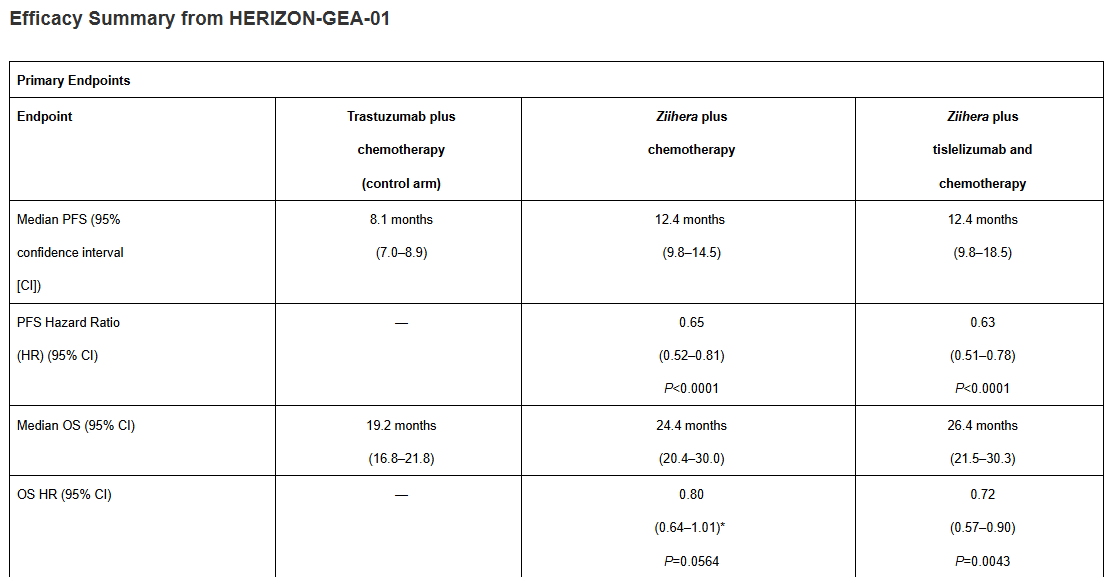
Late-breaking press release ahead of ASCO GI for HERIZON-GEA-01, testing zanidatamab + chemo, with or without tislelizumab, vs trastuzumab + chemo in first-line HER2+ locally advanced or metastatic GEA.
Important caveat up front: this is a press release, not a paper. But the signal is hard to ignore.
🧬 PFS improved in both zanidatamab arms
Median PFS 12.4 months for both doublet and triplet vs 8.1 months with trastuzumab
Roughly a 35% reduction in risk of progression
🧠 The real interest lies in OS
Triplet median OS 26.4 months vs 19.2 months with trastuzumab
That’s more than two years median OS in metastatic GEA
The doublet also crossed 24 months with a strong trend (is tisle necessary?)
🧐 Key nuance:
PFS is essentially identical between doublet and triplet
OS clearly separates
This looks like depth and durability rather than early disease control
📊 ORR is similar across arms, but duration of response is dramatically longer
DoR 20.7 months with the triplet vs 8.3 months with trastuzumab
💧 Toxicity note
Diarrhea is the standout issue and will need proactive management
Grade 3 or higher diarrhea occurred in roughly 20 to 25 percent, with overall diarrhea rates around 40 percent
Open question
I would love to see this compared head-to-head against current SoC chemo + trastuzumab + pembrolizumab. That said, it’s hard to argue with a two-year median OS and a clear survival tail.
Takeaway:
If confirmed on full presentation, zanidatamab looks poised to replace trastuzumab in first-line HER2+ GEA. The next step may not be whether it works, but how much intensity each patient really needs.
#GI26 @OncoAlert@TheGutOncLab
https://t.co/m4aJv6h5nv
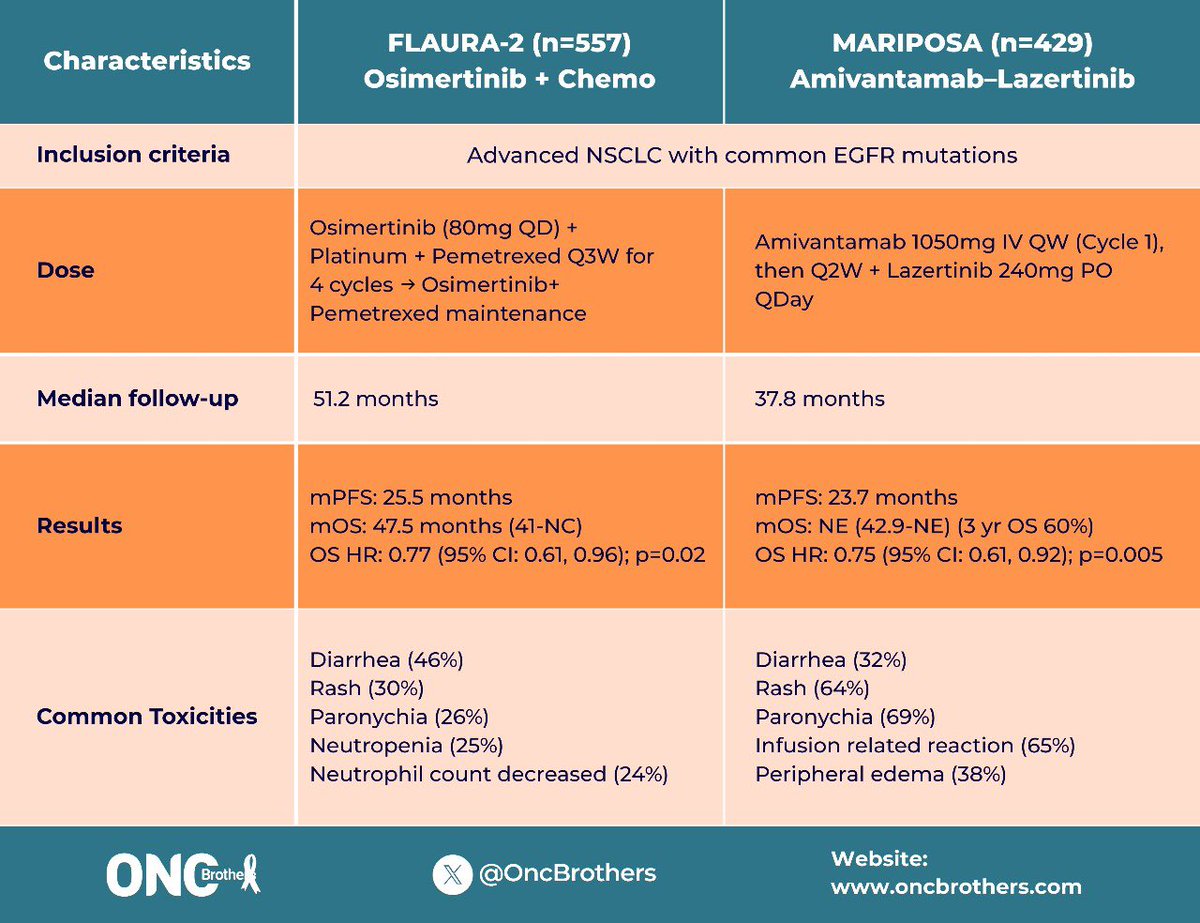
We all will be having this conversation and cross trial comparison for every EGFR mNSCLC pt we see in the clinic. Take a minute to get a real pt perspective by @jillfeldman4 👇👇 #FLAURA2 & #MARIPOSA data!
#WCLC25#OncTwitter#lcsm
There’s no Level 1 evidence that our current frequency of post-treatment surveillance imaging & labs reduces the risk of death.
(From NEJM piece on pros/cons of routine surveillance protocols, especially relevant in current ctDNA era) – worth a read!
https://t.co/usCJsBIgHI
Online now for the #AACR25 session on Advances in #KRAS Biology in PDAC by session speaker @andrewaguirremd: Response and Resistance to RAS inhibition in Cancer https://t.co/y2lwO3oXdz
Evolution of HER2 testing over 40 yrs.
IHC lacks the dynamic range to predict outcomes with T-DXd, yet novel quantitative assays are emerging.
We presented data with HS-HER2 to predict T-DXd activity at #ESMO24. More data coming at #ASCO25.
Stay tuned.
https://t.co/ZcH1fAjpJd
PSA to cancer patients out there. Putting the word integrative in front of their name does not make a non-oncologist an oncologist. Cancer biology is incredibly complicated and takes decades to learn. If someone did not do medical oncology fellowship they are not med onc. #bcsm
HER2 is no longer just a breast/Upper GI cancer story. ADCs are changing the landscape, making HER2 a tissue-agnostic target across multiple tumor types. Our mini-review article in @FrontOncology on the subject. @OncoAlert
https://t.co/PQC2TPWQTn
ctDNA in CRC is prognostic, but there is no data showing that treatment initiated earlier based upon ctDNA positivity confers improved survival (or QOL).
Earlier detection alone does not equal benefit.
Great job @KristenCiombor 👏👏 #GI25
I’m so honored to present this important study on patient awareness of HER2-low breast cancer, led by amazing @BeccaPrevisMD@Labcorp@outcomes4me at #SABCS24 🌟
➡️ Patient awareness gaps exist and education increases biomarker awareness and empowers pt-doc discussion
As I try to figure out INAVO120, I would like to point out that patients with PIK3CA mutations do very well on first line Abema/Fulv or Ribo/Fulv with median PFS beyond 16 months in registrational trials.
Palbo/Fulv as a control arm is questionable
Thanks @Larvol for dataset.
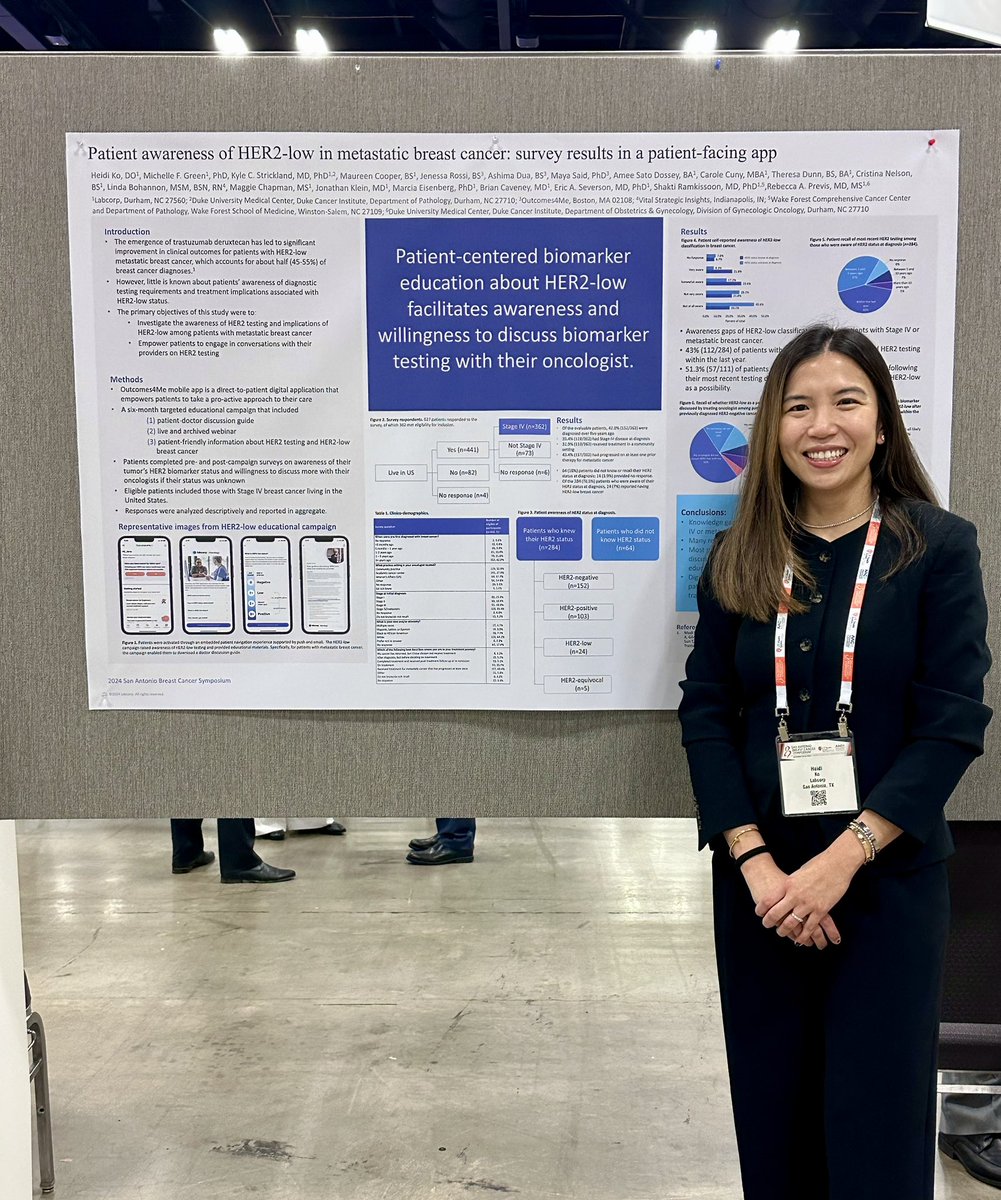
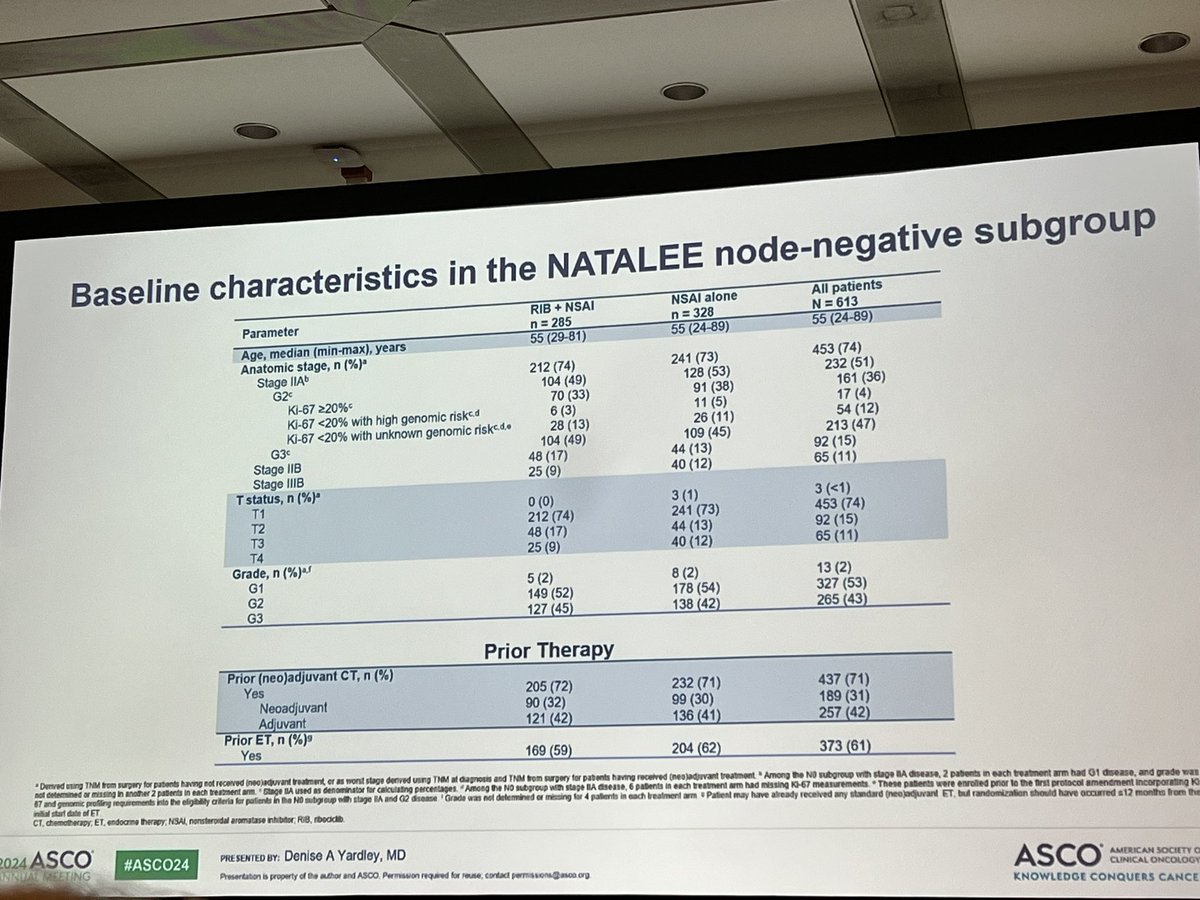
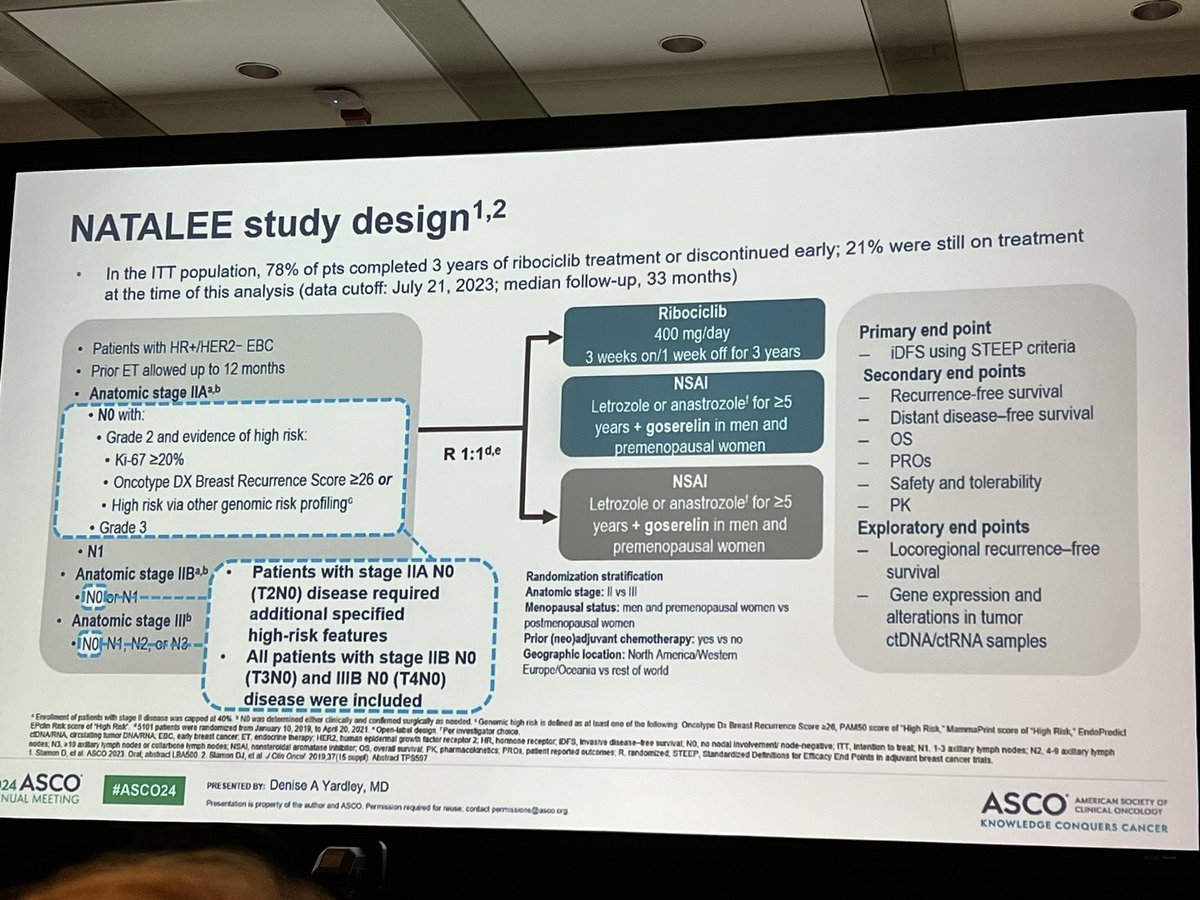
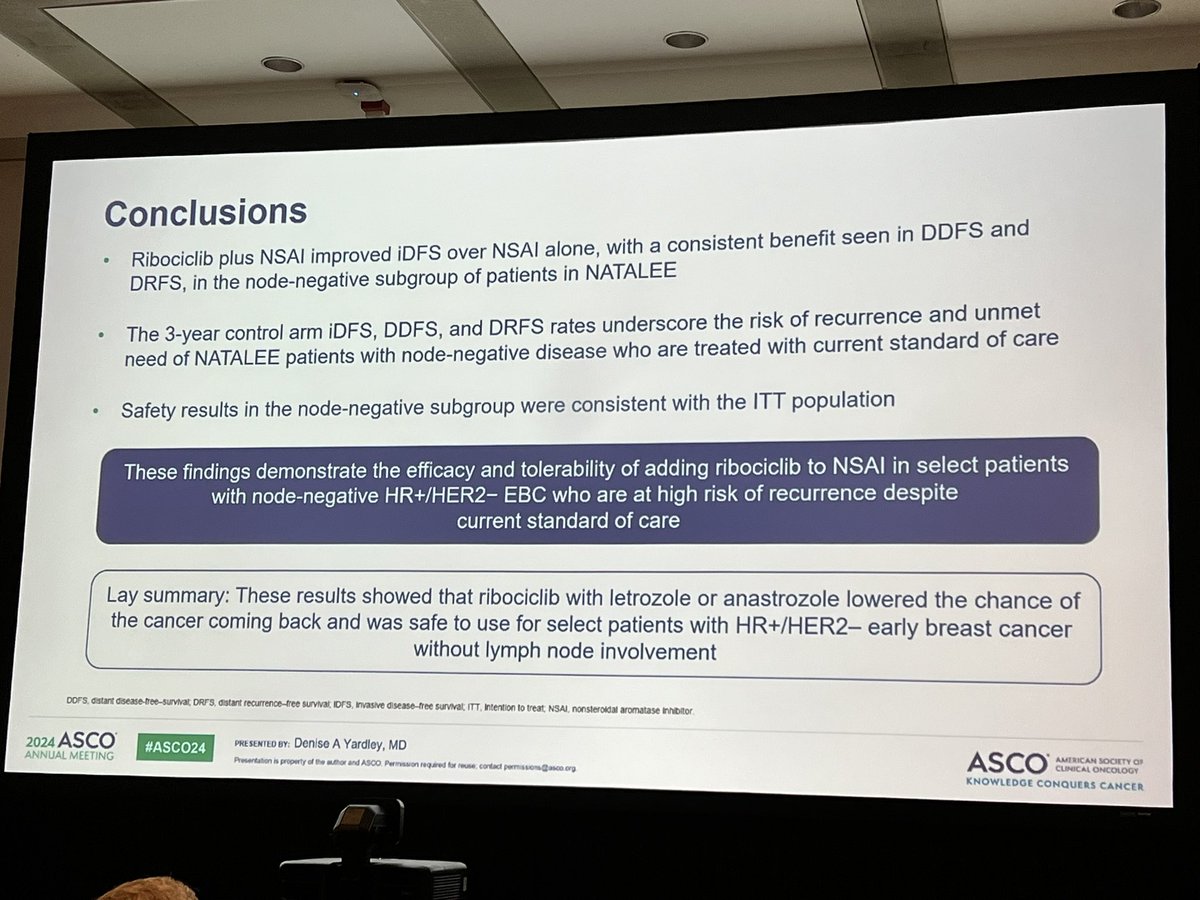
Node-negative subanalysis of NATALEE (n=613). Mostly includes patients with T2 disease (75%), virtually all with G2-3 disease. Consistent benefit in iDFS (93.2% vs 90.6%, HR 0.72), DDFS and DRFS with adjuvant ribociclib. Safety also consistent with ITT. #ASCO24#bcsm