@Chronotrope Should we not be using remifentanil to blunt the spinal reflexes? If hypnosis is appropriate (as seen on the DSA/pEEG), then the issue is nocicpetive input for which we have remi. Why paralyze the patient? Increase the remi to treat the problem ?
@Chronotrope@gas_liverpool@Rollo002@BluntingStress@TIVAuk@SIVAnaesthesia Are you suggesting that remi made the alpha disappear? Is it not more likely the reduced cardiac output from more remi caused a plasma increase of propofol, deepening the patient as if they had received a propofol bolus. How, If possible, would remi even cause alpha loss?
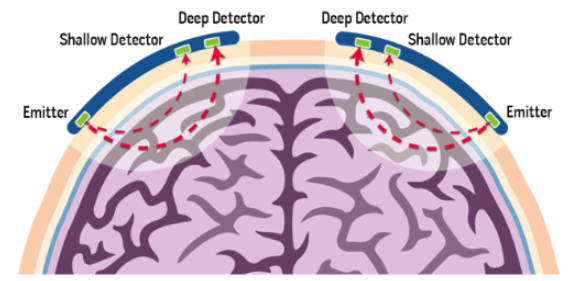
🆕 Last tutorial of the year - ATOTW 538: Cerebral Oximetry—An Introduction https://t.co/brMo7ctVOP
This tutorial provides a concise overview of cerebral oximetry, focusing on the basic science of near-infrared spectrometry, its limitations, primary applications, and its use in various surgical procedures. #anaesthesia #anesthesiology #cerebraloximetry
@DrShmuk@francisco_alobo You are cherry picking. The Irwin article is very good,but you can't use it as absolute proof to mix any drugs-It speaks more about mixing for TIVA, and not about fixed doses and fixed rate infusion-it also says you need to have proof of stability of your mixes,which Daniel does
@Chronotrope@hdavidrosen@DrShmuk Please correct me, but i was under the impression that B-unaware and BagRecall (both M. Avidan) showed that with EtAA monitoring, awareness (with recall) was equivocal with or without DoA monitoring. Is that not accurate?
Did 2 awake VL oral intubations today, using airway blocks. Worked an absolute treat. Really satisfying to have a completely awake pt with tube down their throat and completely comfortable.
@bobfunn There are occasions where mixing is ok. And have been tested as safe. Lido+Mgs (for obs), KLM for OFA or sparing, soda bic and lido for epidurals, ketamine+propofol. Willy-nilly bad, tested... Not so bad. https://t.co/GcXEAg4UMW https://t.co/Qn6kPH67fz
@MoosaFarhaan@jeffgadsden@amit_pawa@RegionalAnaesUK@DrMGorecha But then again, plastics and ortho do this routinely for various blocks and for them is almost second nature to do. That doesn't mean they are correct though. Best advice :High conc+ultrasound =minimal wait and maximum effect
@MoosaFarhaan@jeffgadsden@amit_pawa@RegionalAnaesUK@DrMGorecha "Mixing local anesthetics does not produce a faster onset and reduces the duration. It’s not the best of both worlds - it’s the worst of both." https://t.co/80bjPvVagq.
This article (IMO) - Compelling argument to NOT mix...
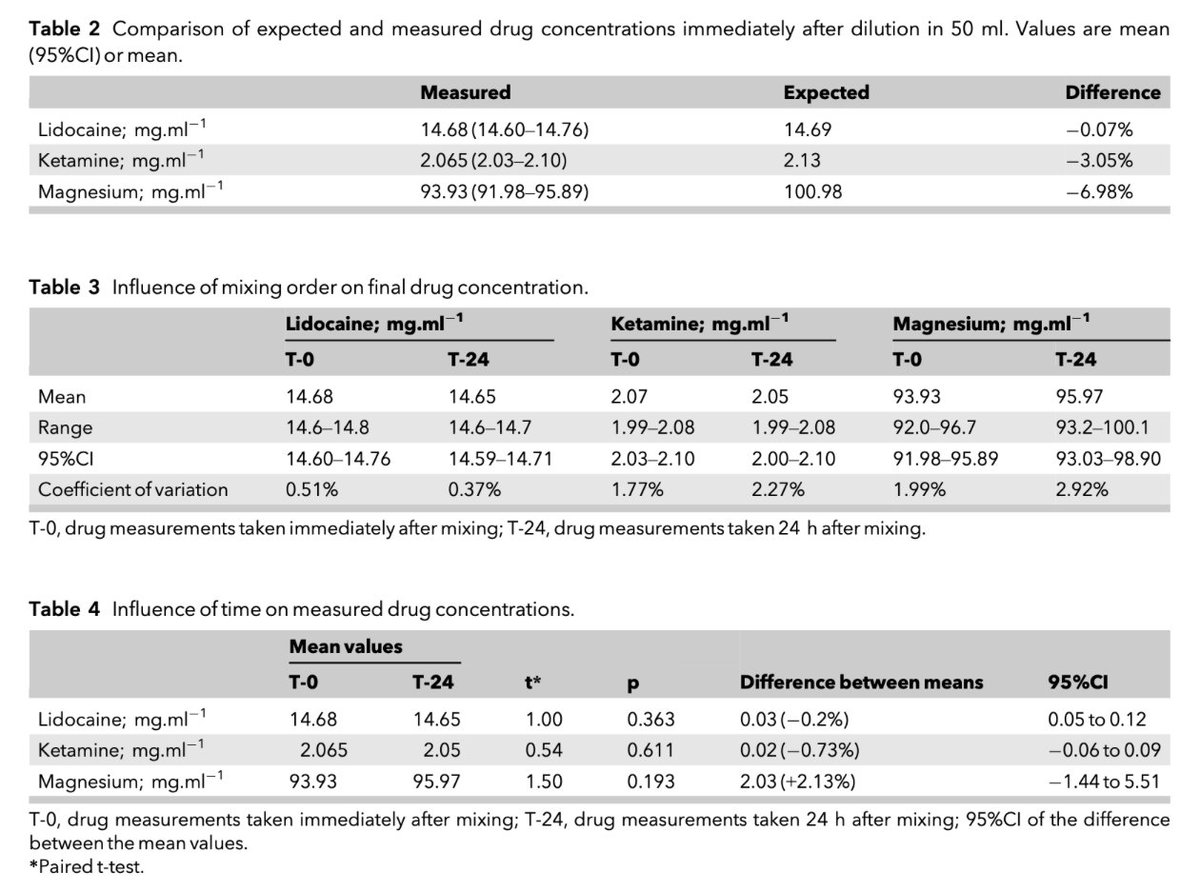
@critconcepts I once tried to show that this mix is safe and stable using HPLC. The preliminary results were good. A mix similar to this is used for opioid free Anaesthesia and is well described. It is a really nice combination though... get mixing
@francisco_alobo@FriedbergBarry@Anaes_Journal@kwymansa The ability to combine the drugs, even though we don't know which is the most effective, was the key point. In out setting with only one syringe driver, we can now do a form of OFA. I think that is more important than which drug is best
🔐A mixture of ketamine, magnesium and lidocaine in one syringe were chosen for testing as they are commonly available, but with an aim to make this admixture relevant for low- and middle-income countries such as South Africa.
@kwymansa
🔗https://t.co/xSwR0TR1p1
🔐Compatibility and stability of an admixture of multiple anaesthetic drugs for opioid-free anaesthesia.
This great new paper from @kwymansa is now #FreeForAWeek!
🔗https://t.co/xSwR0TR1p1
@sillyoldjen So you use no medication at all? You are very lucky, many people in the world aren't so lucky. In terms of on label off label use, fair point, but I think you will find we use MANY drugs off label to help people. It is about balancing risk and benefit
@sillyoldjen We are well aware that mixing drugs can cause unknown reactions.. That is precisely why we do research like this, to make sure that it is safe and that there are no untoward reactions. All drugs can have side effects, but I assume you use paracetamol.
@sillyoldjen You aren't a doctor. And more importantly, you are not an Anaesthetist. You seem to be angry and hurt about something, sorry about that. But that paper, my paper, is pretty good. And will help in LMIC countries. Mixing drugs is fine- if done correctly and in a safe manner.