The Respiratory Care Foundation of Texas provides respiratory care students with scholarships to aid their educational journey. Please support our 48hr Tis the Season Flash Fundraiser.
Donate here: https://t.co/QiE8zHKqHB
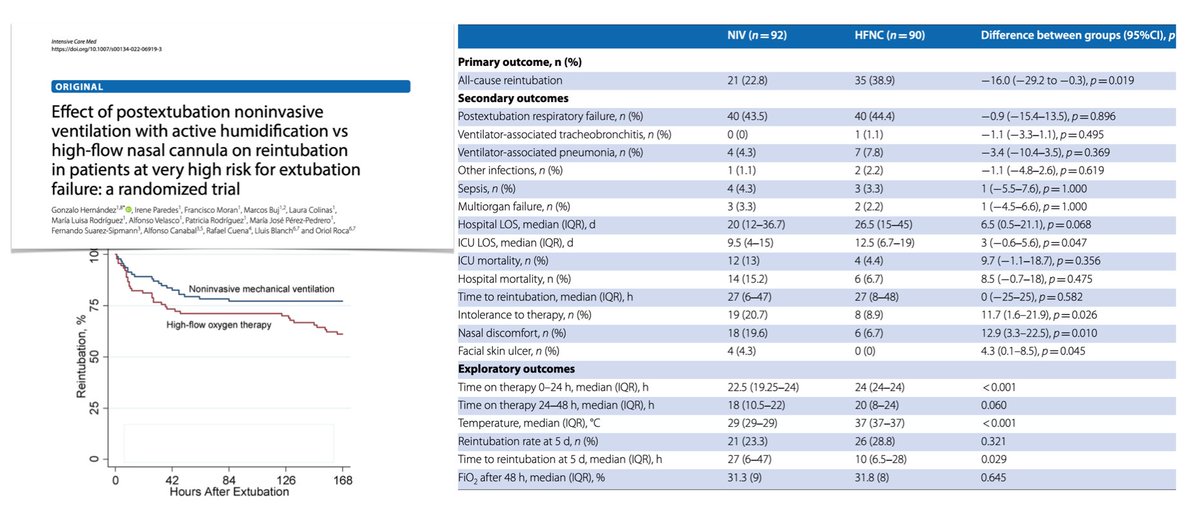
NIV + active humidification vs HFNC in adult critically ill pts at very high-risk for extubation failure, RCT in 🇪🇸 ICUs: noninvasive ventilation superior to high-flow nasal cannula O2
➡️ reintubation required in 23.3% pts receiving NIV vs 38.8% if HFNC
📎 https://t.co/2mNTf3PYEF
@BrownHospMed Great visual of the pendeluft effect. You see the protrusion of the right chest wall occurs during the patient's expiratory efforts. Thanks for sharing!
@ArielG_RRT@ventilacionmeca@DocMusician@DrMiguelIbarra1@emireles_c@RyanHughes_RRT@GkuhnRRT I would assess P100 and observe the patient in a spontaneous mode to assess their desired volume, flow and pattern, and attempt to mimic that if spontaneous isn't sufficient. And reassess P100 for neural drive satisfaction post changes. Thanks for posting this. Good exercise.
@ArielG_RRT@ventilacionmeca@DocMusician@DrMiguelIbarra1@emireles_c@RyanHughes_RRT@GkuhnRRT Clearly for every mandatory breath delivered there's at least one missed patient effort. First thought was CMV mode, but then recognized that the vent does respond to the subsequent effort which appears greater than the missed effort, so perhaps sensitivity setting or PEEPi?
Mechanical ventilation and end of life. Clear and concise communication can mean the difference between prolonged suffering or liberating the tube and vent for peace and comfort. We should all hope for peace and comfort in our final moments. #respiratorytherapy