I am interested in personalized care and translational research in women’s cancer. lab & clinical research knowledge apply in my “bench-to-bedside" approach.
If you have breast cancer you must watch this episode of @breastfriendspd featuring my incredible oncologist and friend Dr @hoperugo. She understands where we came from and where we are going, values supportive care as much as treatment, and I’m lucky to have her in my corner.
In 1998, the approval of trastuzumab began to change the poor prognosis of HER2-positive breast cancer for the better.
Over the following nearly 30 years, anti-HER2 therapy evolved step by step: trastuzumab, pertuzumab, T-DM1, and now T-DXd.
With the latest anti-HER2 ADC data, T-DXd has now been approved in two new indications for early-stage HER2-positive breast cancer.
First, we changed the prognosis for the better.
Now, the goal is cure...
T-DM1 or T-DXd after neoadjuvant therapy?
Residual HER2+ disease after NAC does not automatically mean adjuvant T-DXd.
🔹 KATHERINE → any residual invasive disease qualified for T-DM1
🔹 DESTINY-Breast05 → T-DXd studied in higher-risk residual disease
Key high-risk features in DESTINY-Breast05: • Initial cT4/cN2–3 disease
OR
• Residual nodal disease (ypN1–3)
An important eligibility distinction while interpreting adjuvant escalation strategies.
#BreastCancer #HER2positive #Oncology #MedEd #MVOnco
Major FDA news today for early-stage HER2+ breast cancer. T-DXd approved for two separate indications: neoadjuvant Stage II/III disease (T-DXd x4 followed by THP x4), and adjuvant treatment for residual invasive disease after neoadjuvant HER2-targeted therapy.
The data are striking. DESTINY-Breast11: pCR 67.3% vs 56.3% with ddAC-THP (p=0.003). DESTINY-Breast05: 3-year IDFS 92.4% vs 83.7% with T-DM1, HR 0.47 (95% CI 0.34-0.66, p<0.0001).
But the real work is just beginning. Not every high-risk patient needs T-DXd upfront. Our challenge as oncologists is figuring out who needs what. Biomarker-driven selection, ctDNA, pCR response – these questions have to follow. Escalation and de-escalation strategies needed. #bcsm
#BCSM #BreastCancer
Wow- big month for breast approvals so far...and it's only May 15th!
#TDXd approved for neoadjuvant and adjuvant HER-2+ #bcsm
Our @US_FDA breast colleagues have been very busy, thank you!
In this video, Fengting Yan, MD, PhD, (@FengtingYan) discusses how her clinical practice is informed by data and guidelines available on testing in breast cancer. #bcsm
https://t.co/9nQ0DtTq0q
I will be speaking at the Best of Hematology and Breast Cancer 2025 on January 3-4, 2025 in Seattle. My talk will be on 'No' for the Hrt Debate
You can register here: https://t.co/z7lINDqsWo
2
A new moonshot to fight cervical cancer is missing something: only one of the sponsors is within reach of the WHO’s recommendation for protecting women. We can and must to better LINK HERE:
https://t.co/jxgVdajnou
@btfoundation@binayshah@ProvSwedish @swedish @sid
Our opinion piece in @statnews highlighting the need for stronger implementation and broader access to HPV vaccination programs to end cervical cancer in the US and across the globe. Thank you @binayshah and @FengtingYan for co-authoring this.
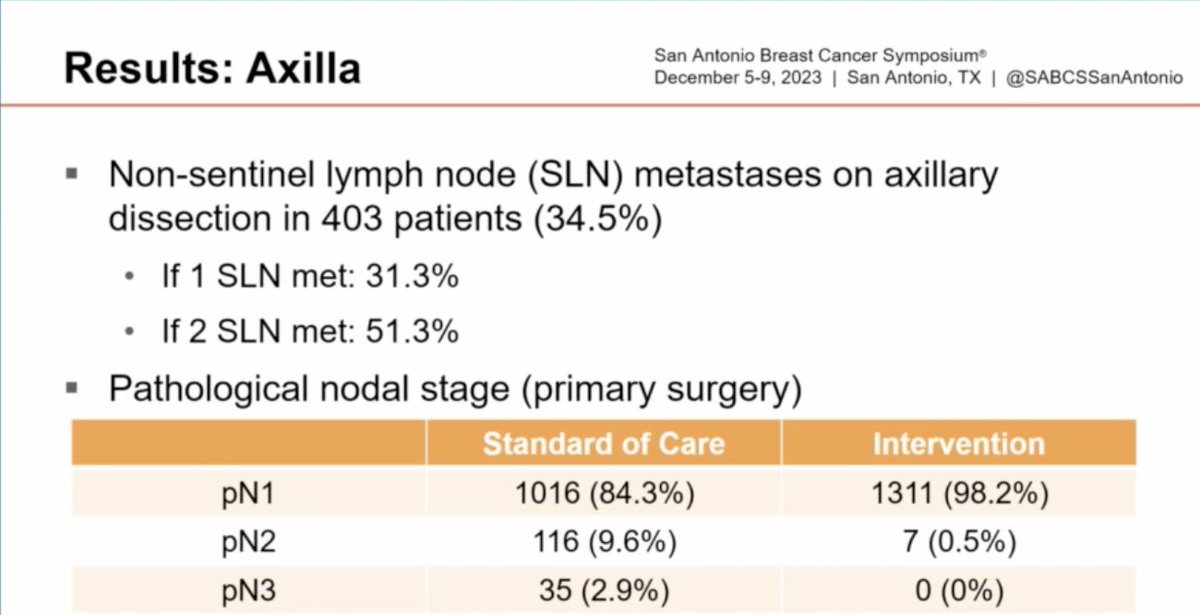
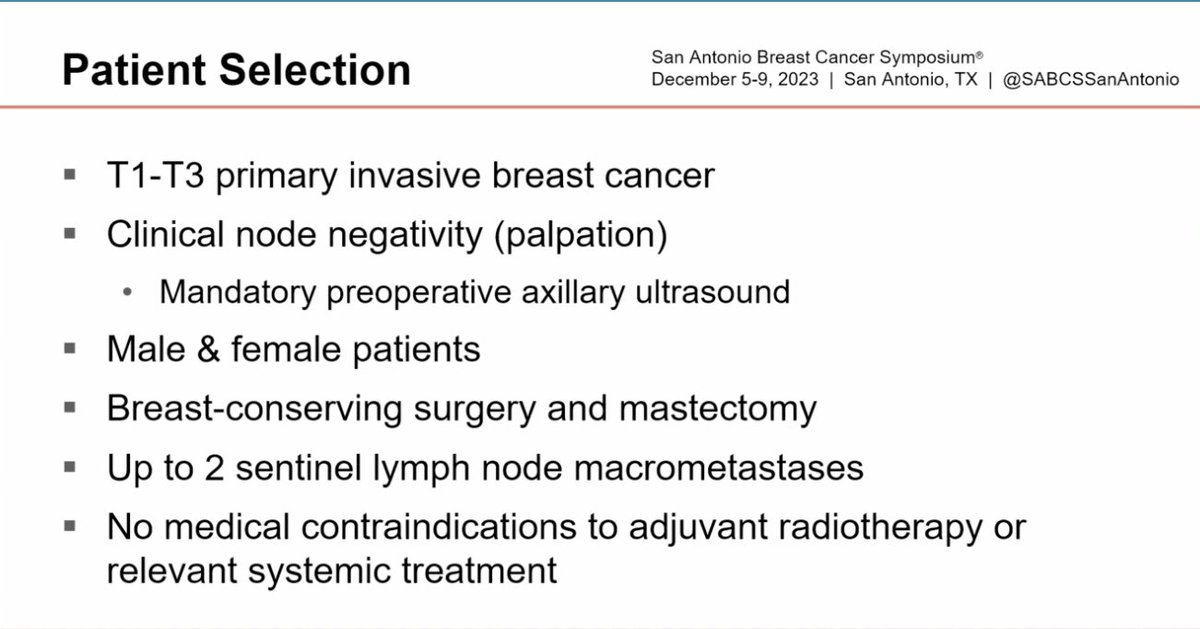
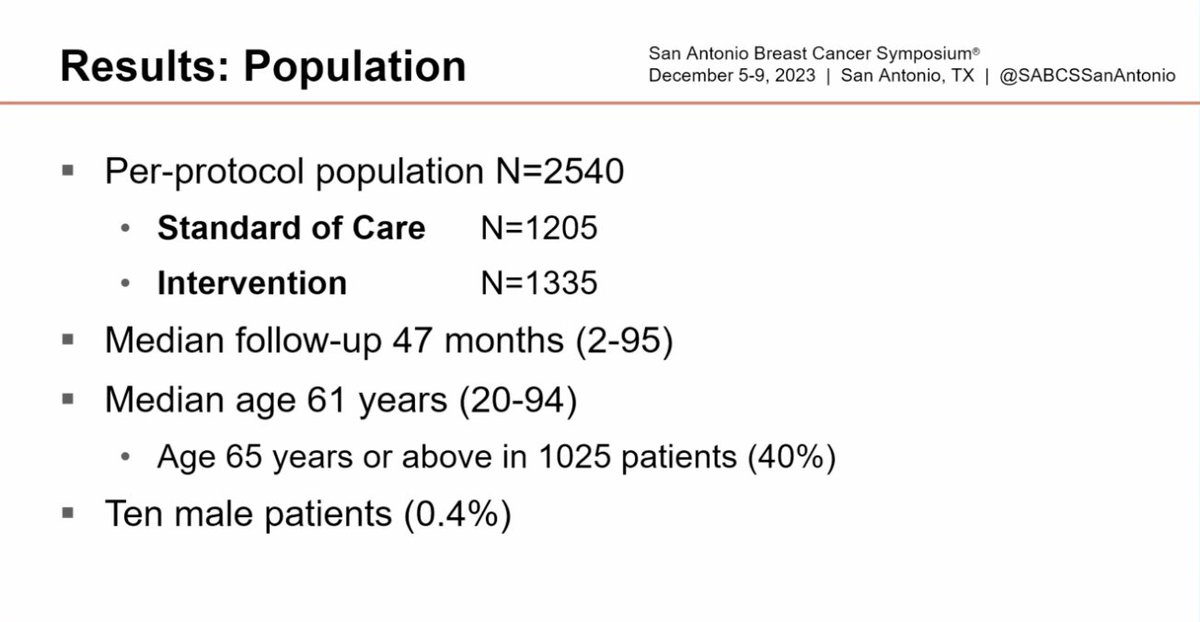
SENOMAC: SNB +/- ALND in pts with up to 2 macromets
n=2450
Median f/u 47 mo
Median tumor size 20mm (6% T3)
85% had 1 macromet
34.3% with ENE
34.5% had additional LNs on ALND (if 1 SLN 31.3%, if 2 SLN 51.3%)
No difference in 5 yr RFS 88.7% vs 89.7%
#SABCS23@OncoAlert
At #SABCS23, check out our poster presentation exploring the safety profiles of Chinese breast cancer patients who received a CDK 4 & 6 inhibitor in the MONARCH plus and monarchE trials.
See the data here: https://t.co/tHZRe745Dj
#bcsm#BreastCancer#CancerResearch
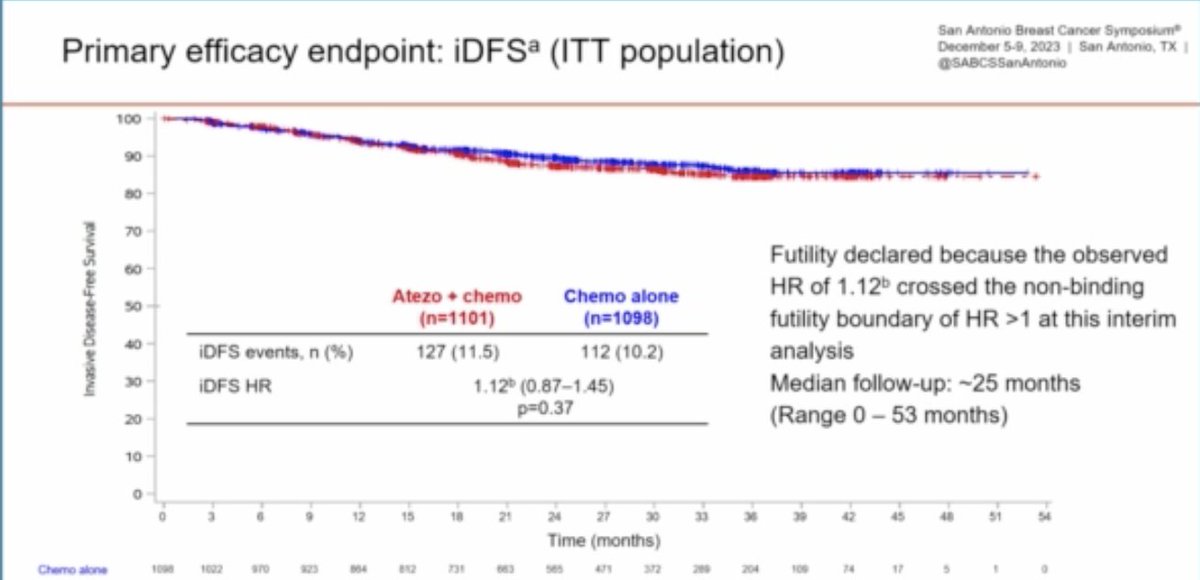
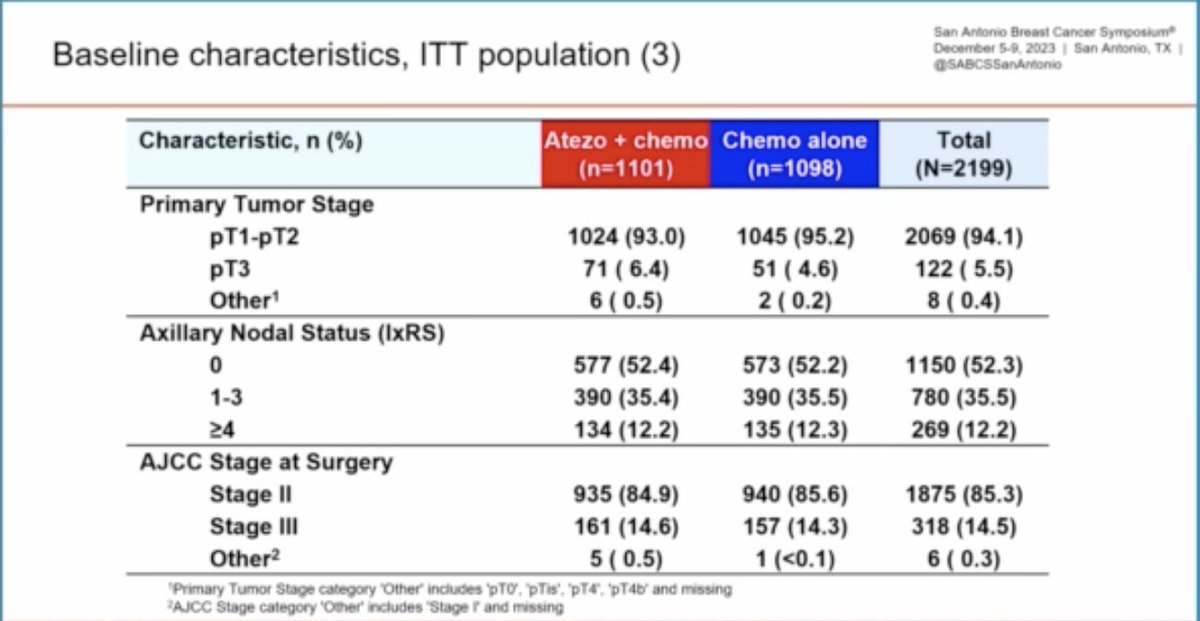
IMP030: Adj chemo+/- atezo in stage 2/3 TNBC
Median f/u 25 mo
iDFS: HR 1.12, p=0.37
iDFS in PDL1+ HR 1.03
Why is there no benefit in the adjuvant setting? Is it PDL1 vs PD1 (unlikely given benefit in IMP031 preop)? Is it that there is no tumor in place?
@OncoAlert#SABCS23
HER2CLIMB-02: The addition of tucatinib to T-DM1 significantly improved PFS (9.5 vs 7.4 months, HR 0.76, p=0.016) in patients with HER2+ MBC. OS curves look reverted (HR 1.23), though immature. Significant increase in the rate of severe liver toxicities and diarrhea. Poll below👇
monarchE: ctDNA at baseline + 24 mo in a subset of pts
Detection of ctDNA at baseline soon after completion of neo/adjuvant tx: 10/178 (5.6%)
3 of 10 cleared ctDNA + none recurred
7 of 10 had persistence + all recurred
#SABCS23@OncoAlert#bcsm
MONARCH3: AI +/- abemaciclib
Final OS analysis
Median follow-up 8.1 years
66.8 vs 53.7 mo
Absolute Difference 13.1 mo
Not statistically significant
23.3% progression free at 6 yrs on the abemaciclib arm
@oncolaert #SABCS23