@Rainmaker1973 Look into Dendritic Cell vaccines for cancer. More specifically #DCVAX. Thats the real deal. PH3 complete with promising results for Glioblastoma. The Dendritic cell platform can be used for all solid tumors. Its being commercialized currently by $NWBO.
$nwbo @alphavestcap
"So the company may submit the IND package to the FDA by the end of this month!", which makes the 6/3/26 Parker timing propitious.
https://t.co/kRkh9s9Kjo
https://t.co/Y7j5yoERZ8
https://t.co/kgS6arxf9S
https://t.co/Y7j5yoERZ8 https://t.co/e6lCpCZxrR https://t.co/e6lCpCZxrR https://t.co/ZJZOb4STAI https://t.co/tURKZodAgq https://t.co/gdfCyrbsWF https://t.co/IukQ16JoAI https://t.co/1lr9YNW6VB https://t.co/gdfCyrbsWF https://t.co/Z6QG9OiuKN https://t.co/haLAtddirO
https://t.co/ZJZOb4STAI https://t.co/5spbps8BE2 https://t.co/qf3LKRmBks https://t.co/tURKZodAgq https://t.co/5eoiv4mcfx
@ATLnsider I doubt $NWBO would help long-term Glioblastoma survivors appear before Congress if they thought their product lacked efficacy and could not be approved.
When will @adamfeuerstein and @John_Hempton appear before Congress to argue DCVax is Grapefruit Juice?
This is the validation event for $NWBO #DCVax-L's Phase 3 design.
INSIGhT showed matched external controls correctly return the null for three failed drugs (HRs 0.88 to 1.00). DCVax-L used a more rigorous version of the same method (roughly 20x the patients, RCT-only comparators, 14 prespecified criteria) and produced 0.58 at first recurrence, far outside that bias band.
And the bias runs the wrong way for skeptics. Rahman's own 2025 Neuro-Oncology paper found trial-enrolled #GBM patients have worse survival than non-trial patients (HR 1.30). DCVax-L drew its controls from RCT arms, so the comparison is tilted against the therapy. The 0.58 is most likely an underestimate, not an artifact.
The irony: this method was criticized in JAMA Oncology in 2023 by a founding INSIGhT co-author. His own former collaborators just published the paper validating it.
INSIGhT, FDA, and MHRA all converge on one conclusion:
https://t.co/RLaMmSi65t
#dcvax $nwbo #gbm
Research Spotlight: External Controls Show Promise for Use in Glioblastoma Clinical Trials
May 27, 2026
Rifaquat Rahman, MD, a radiation oncologist with Mass General Brigham Cancer Institute, is the senior author of a paper published in the Journal of Clinical Oncology, “Treatment Effect Reanalysis of the Randomized Individual Screening Trial of Innovative Glioblastoma Therapy Trial in Newly Diagnosed Glioblastoma With External Control Data.”
Rifaquat Rahman, MD📷
Q: What challenges or unmet needs make this study important?
Glioblastoma (GBM) is a highly aggressive primary brain tumor that has a poor prognosis despite standard of care surgery, radiation therapy and chemotherapy. Many ongoing research efforts aim to develop more effective therapies for GBM, but there have been very few advances over recent decades. Because inefficient clinical trial designs have been identified as one of the challenges for the field, the idea of “external control data” could offer a solution.
External control data means comparing outcomes for people enrolled in a clinical trial to people external to the study. Patients have expressed support for these approaches, as many patients enroll in GBM clinical trials in hopes of receiving a promising experimental therapy and do not want to receive standard of care therapy on the control arm of a trial.
Q: What methods or approach did you use?
We conducted a validation study that re-analyzed a completed randomized controlled trial with external control data. We did this to see if external control data could work for future clinical trials and early-phase testing of promising therapeutics for patients newly diagnosed with GBM.
To serve as possible external control arms for GBM trials, we derived patient-level data from multiple real-world and clinical trial datasets, including data from our institution and others. We did this over several years, as it’s very challenging to assemble this type of data.
We then re-analyzed the experimental arms from the INSIGhT randomized trial (NCT02977780), swapping out the internal control arm from the trial with our external control dataset. We applied statistical techniques to adjust for differences between the external control patients and INSIGhT trial participants. This included estimating treatment effects with the external controls.
As part of our study, we evaluated several novel clinical trial designs—specifically, a single arm trial with external controls, and hybrid trials with randomization and external controls. We also simulated scenarios to evaluate trial designs that integrate external controls.
Q: What did you find?
When we re-analyzed the data from the INSIGhT trial, we obtained the same result when using our external control datasets as the original randomized trial. This supports the use of external control datasets for future clinical trials.
Q: What are the real-world implications, particularly for patients?
For GBM, where the current standard of care control therapies lead to poor outcomes, patients often have a strong preference to receive promising experimental therapies. Our study provides a pathway to novel clinical trials where more patients receive the experimental therapy and fewer patients are assigned to the control arm. Not only would these trials be more patient-friendly, but they would also help accelerate the discovery of new promising therapies for GBM.
Read the paper(opens external link in new tab)
Authorship: In addition to Rahman, Mass General Brigham authors include Isabel Arrillaga-Romany, Tracy T. Batchelor, Wenya L. Bi, Omar Arnaout, Pier Paolo Peruzzi, Daphne Haas-Kogan, Shyam Tanguturi, Ayal Aizer, Sandro Santagata, David M. Meredith, E. Antonio Chiocca, Keith L. Ligon, and Patrick Y. Wen.
Paper cited: Rudra Gupta, T., et al. “Treatment effect re-analysis of the randomized INSIGhT trial in newly diagnosed glioblastoma with external control data.” Journal of Clinical Oncology. DOI: 10.1200/JCO-25-01586
Funding: This work was supported by the National Institutes of Health (R01LM013352). Rahman is supported by Joint Center Radiation Therapy Foundation Grant and Kayes Technology Grant.
Disclosures: Rahman reports consulting or advisor board participation for Servier, Telix, and NH TherAguix. Additional author disclosures can be found in the paper.
Gemini AI Analysis on potential relevance for DCVax platform technology
he May 27, 2026 announcement from Mass General Brigham regarding the Journal of Clinical Oncology paper ("Treatment Effect Reanalysis of the Randomized INSIGhT Trial in Newly Diagnosed Glioblastoma With External Control Data") is not a threat to Northwest Biotherapeutics (NW Bio) or DCVax-L.
Instead, this announcement represents a massive scientific validation, a structural tailwind, and a profound regulatory synergy for NW Bio's clinical trial methodology.
The relationship between this announcement and DCVax-L reveals why this acts as a validation rather than a threat.
1. The Core Synergy: Academic Validation of NW Bio’s Blueprint
The biggest battle NW Bio fought over its Phase III trial for DCVax-L was its pivot to a contemporaneous external control arm to measure overall survival (OS). Skeptics and traditionalists argued that external/historic controls were inherently flawed due to selection bias and could not accurately mirror a randomized internal control.
Northwest Biotherapeutics
The Mass General Brigham study completely dismantles that skepticism.
What the Study Did
Led by Dr. Rifaquat Rahman and a team of top neuro-oncologists (including prominent names like Dr. Patrick Wen), researchers took a completed, gold-standard randomized trial (the INSIGhT trial) and deliberately ripped out the internal control arm. They replaced it with a meticulously curated, propensity score-matched external control dataset.
Mass General Brigham
The Ultimate Finding
When they re-analyzed the trial using external controls, they got the exact same results as the original randomized trial.
Mass General Brigham
The Synergy: This is an independent, peer-reviewed proof-of-concept proving that external controls, when properly adjusted using statistical techniques like propensity scoring, are highly precise and reliable in Glioblastoma (GBM). It gives regulatory bodies like the FDA, MHRA, and EMA an independent, academic green light to trust external control data in neuro-oncology.Mass General Brigham
2. Why This Is NOT a Threat
To be a threat, an announcement usually needs to introduce a competing therapeutic breakthrough, a superior manufacturing platform, or a regulatory roadblock. This announcement does none of those things.
It’s a Validation of Methodology, Not a Drug: The paper does not present a new molecule or vaccine that competes with DCVax-L's dendritic cell platform. It re-evaluated abemaciclib, neratinib, and CC-115—therapies that had already failed to show survival benefits. The study simply proved that an external control could identify those failures just as accurately as an expensive, internally randomized trial
The Shared Network Effect:
Look at the co-authors on the paper. Institutions like Mass General Brigham and Dana-Farber (where Dr. Patrick Wen operates) are the absolute epicenters of neuro-oncology. Having these specific elite clinicians publish a paper championing external controls creates a more receptive environment for approvals of drugs that relied on that exact design—chief among them being DCVax-L.
3. The Long-Term Commercial and Trial Potential
The broader implications of this study align perfectly with the arguments NW Bio has made for years regarding trial ethics and speed.
Patient Recruitment & Ethics
As Dr. Rahman noted in the announcement, GBM patients strongly resist enrolling in trials where they risk being randomized into a standard-of-care (SOC) placebo arm, because SOC outcomes are notoriously poor. By validating single-arm or hybrid trials using external controls, the medical community can promise patients: "If you join this trial, you will receive the experimental therapy." This will radically accelerate trial recruitment.
Mass General Brigham
The GBM-X Platform Accentuation
The study mentions the development of the Glioblastoma External (GBM-X) Data Platform, designed to help investigators leverage external data to contextualize single-arm trials early in drug development.
ResearchGate
This infrastructure benefits advanced platforms like DCVax. As combination therapies (e.g., combining DCVax-L with checkpoint inhibitors or localized therapies) become the next frontier in neuro-oncology, companies will no longer need to waste years and hundreds of millions of dollars building massive placebo arms. They can run agile, highly targeted trials against verified external baselines.
https://t.co/uR3hmg6E9I
✅️Algorithms Discoverable?
The federal magistrate judge in $NWBO's spoofing lawsuit against six of the largest market makers in the world, including Citadel and Vitru, believes that the Defendant market makers' trading algorithms are discoverable
The Magistrate Judge stated, in relevant part:
"I'm not sure how that gets limited, frankly." [1]
See attached Image.
[1] Docket #286, https://t.co/2vLwDOXAki
Google is raising $80 billion of equity a week before SpaceX is trying to raise $75 billion a few months before Anthropic and OpenAI are trying to raise $100 billion from investors and you’re laughing???
This is a cataclysmic exit liquidity avalanche
$NWBO
@zubirahmed@Siobhain_Mc@Keir_Starmer@wesstreeting@METhompson72@biggercapital
After more than 2.5 years in the MHRA process, the question is no longer whether a decision should be made on DCVax-L — the question is why a decision still has not been made.
At this point, I cannot help but wonder whether powerful interests are benefiting from continued delay. Every month that passes forces Northwest Biotherapeutics to raise additional capital, diluting shareholders and weakening the company financially. Whether intentional or not, the effect is the same.
It is also impossible to ignore the broader context. Northwest Biotherapeutics is currently pursuing litigation in the United States against several major market makers, alleging manipulative trading practices, including spoofing. These are some of the most powerful participants in the global financial system.
While I have no evidence that any regulatory body has been improperly influenced, it is fair to ask difficult questions when a company involved in such litigation experiences extraordinary delays. Large financial institutions often possess extensive networks of influence throughout the financial ecosystem. It is therefore reasonable for investors to question whether forces that benefit from delay may also be working, directly or indirectly, to prolong uncertainty surrounding this application.
The UK has repeatedly stated its ambition to become a global leader in cell and gene therapies. If that is truly the goal, this case sends exactly the wrong message to investors around the world.
Capital is the lifeblood of medical innovation. Investors fund the research, the clinical trials, the manufacturing infrastructure, and ultimately the therapies that patients desperately need. When a promising therapy remains in regulatory limbo for years, confidence in the system is damaged.
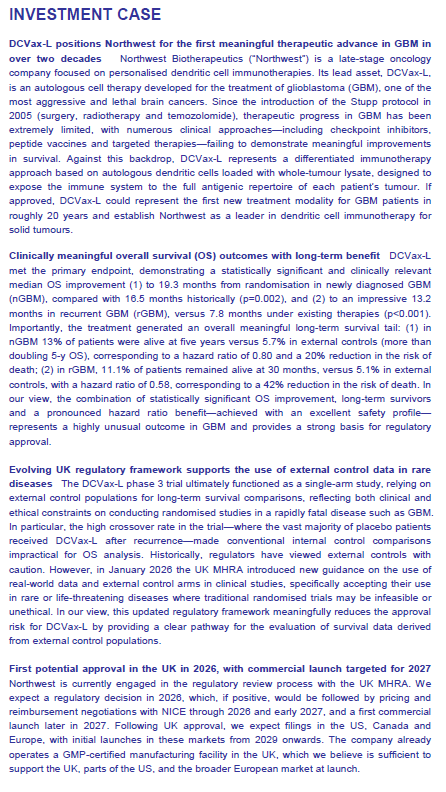
DCVax-L has demonstrated long-term survival benefits in glioblastoma, one of the deadliest forms of cancer. Approximately 13.5% of patients were alive at five years versus roughly 5% under standard care, with a long-tail survival benefit and minimal toxicity.
Meanwhile, patients continue to wait.
Investors continue to wait.
Doctors continue to wait.
The scientific community continues to wait.
Regardless of the final outcome, the MHRA owes patients, physicians, researchers, investors, and the public a clear and timely decision.
If the UK wishes to remain a destination for biotechnology investment and a leader in advanced therapies, transparency, predictability, and timely regulatory action are essential.
Two and a half years is enough.
https://t.co/Tg3T4Mvkuf
@kshaughnessy2@LisainNJUSA Looking forward to seeing @adamfeuerstein convicted next. His knowingly false statements intended to impact the share price of $NWBO were even more blatant when compared to Andrew Left’s actions.
💜 DCVax Long-Term Survivor Series — Part 7 💜
Tonight I want to share the story of Kat Charles from the UK.
After undergoing surgery, radiation, chemotherapy, and even participating in a clinical trial, Kat was told there was nothing more doctors could do. She and her husband Jason were told she had approximately three months to live.
Instead of accepting that prognosis, they kept searching for options.
The family ultimately raised funds to access DCVax.
Years later, Kat told the BBC that scans showed no visible tumor. Her husband Jason said:
“DCVax has done what everyone said was impossible.”
Even more remarkably, Kat later shared that she was still receiving ongoing DCVax injections every six months and was alive 11 years after her glioblastoma diagnosis.
When I was told that long-term glioblastoma survivors don’t exist, stories like Kat’s are exactly why I refused to stop looking.
Every survivor has a story.
Every family deserves hope.
And every patient deserves the chance to fight for their future.
💜 #DCVaxForBraelyn #BrainCancerAwarenessMonth
https://t.co/79rHKEgNR8
GoodGuyBill
$nwbo
@alphavestcap
Thursday, May 28, 2026 10:39:27 AM
A Message to Weary Longs: Why I Still Believe NWBO Has Likely Received Positive MHRA Signals
Let me be blunt: a lot of people on this board are exhausted, and I don’t blame them. The wait has been long, the silence is maddening, and the skeptics love to fill that vacuum with doom. But at some point, you must stop staring at the silence and start looking at the actions. Because NWBO’s actions are not subtle. They’re not ambiguous. They’re not “maybe someday” gestures. They are the actions of a company that already knows where this is heading. NWBO is engaging in concrete, capital-intensive, operationally irreversible decisions that a severely cash-strapped microcap simply cannot justify unless they’ve received strong, positive, non-public signals from the MHRA.
Let’s start with the obvious: NWBO does not have the financial cushion to gamble. With ~$1–2M in cash, heavy liabilities, and a going-concern warning, they don’t have the luxury of throwing money at speculative infrastructure. Every move they make has to be tied to something real. Yet look at what they’ve done anyway.
They committed to a dedicated leukapheresis clinic at London Welbeck Hospital — not a temporary trial setup, but a permanent, commercial-grade facility designed to handle patient volume and even external clients. That is not a “hope” move. That is a “we’re going to need this” move.
Then there’s the Grade C expansion at Sawston, which more than doubles capacity and is explicitly commercial. Grade C is not for R&D. It’s for throughput. It’s for scale. It’s for product that’s going to market. And NWBO is building it out while sitting on barely enough cash to run payroll. That alone should tell you something.
But the biggest tell — the one skeptics never want to address — is the U.S. tech transfer. Tech transfer is expensive, complicated, and irreversible. You don’t do it unless you expect to be producing commercial product. A company in NWBO’s financial condition does not take on that burden unless they believe approval is coming.
And it doesn’t stop there. They’re integrating Flaskworks/Eden automation, which is only needed when you’re planning for thousands of patients, not dozens. They’re negotiating a second UK manufacturing site, which only makes sense if they expect volume beyond what Sawston can handle. Advent is training new facilities, both in the UK and the U.S., and training is the last step before commercial production. You don’t train multiple sites unless you’re preparing for a real launch.
And then, most recently, they brought in Dr. Annalisa Jenkins — someone with global R&D leadership at Merck Serono, senior roles at BMS (both companies’ products were trialed with DCVax-L… coincidence?), a biotech CEO background, and even service on the FDA Science Board. This is not a symbolic hire. This is someone you bring in when you’re preparing for the final regulatory stretch and the transition into commercialization. A company with NWBO’s balance sheet does not bring in someone of her caliber unless they believe they’re going to need her expertise (and Dr. Jenkins would not have accepted the position without believing likewise).
When you put all of this together, the idea that NWBO is just “hoping” for approval becomes laughable. These are post-approval actions happening before the approval announcement. And that only happens when a company has received strong, positive, non-public signals from the regulator — the kind of signals that say, “Make sure you’re ready.” Regulators never say “you’re approved” ahead of time. But they absolutely give late-stage cues about manufacturing readiness, supply-chain planning, post-approval obligations, and commercial-scale validation. NWBO’s actions match those cues point for point.
So yes, the wait is long. Yes, the silence is frustrating. But the company’s behavior is telling a very different story than the skeptics are. NWBO is not acting like a company guessing. They’re acting like a company preparing for the inevitable.
If you’re tired, I get it. But don’t ignore what’s right in front of us. The signals are there. And they’re louder than the wait, the silence, or the skeptics.
“People who shut their eyes to reality simply invite their own destruction.”
—James A. Baldwin (quote from Baldwin's 1953 essay "Stranger in the Village,")
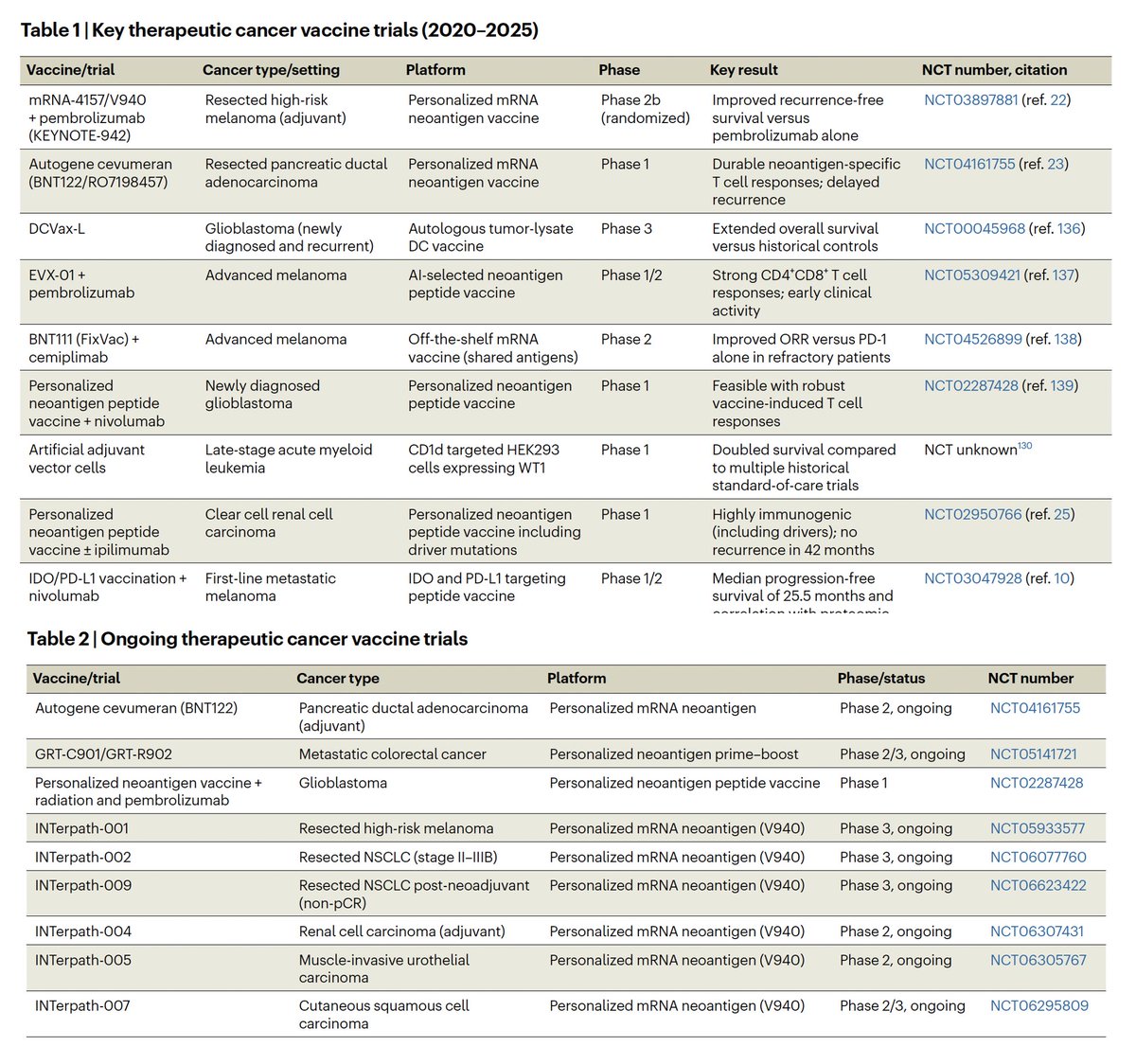
Here's a Table summarizing the personalized vaccines that rev up the immune system vs refractory cancers. Another one vs metastatic melanoma (with ~50% cure rate at 5 years) will be out soon.
$NWBO The Northwest Biotherapeutics Empire Forecast 2030: Why Northwest Biotherapeutics Is the Most Underestimated Cancer Immunotherapy Company in the World https://t.co/HwvgNKXCgP
Commodities vs S&P500
Commodities have been in a major (A-B-C pattern) correction for over 40 years
Now, we are witnessing the start of another massive bull market (imho), due to a perfect mix of shortages, a geopolitical conflict and monetary debasement (flight to hard assets)
Northwest Biotherapeutics: $NWBO
"first potential approval in the UK in 2026"
- First Berlin Equity Research
To me this looks like the greatest advance in treating brain cancer in 100 years. First Berlin think their therapy, DCVax-Direct, could treat all solid cancers.
NWBO '26 Q1 10Q
https://t.co/6CnSZhYu73
At this point I’m skimming the filings for information regarding $NWBO's commercialization of their lead product and steps $NWBO might take to address their cash crunch. The information on additional trials and US manufacturing is great, but those trials and US manufacturing are many many years away from positively impacting the finances. Here is what stood out to me in $NWBO's recent '26 Q1 10Q.
➡️Significant Reduction in Net Loss
The net loss for the 3 months ended March 31st from 2025 was $19.343m and for 2026 it was reduced to $3.069m. I’d imagine we are starting to feel the Advent merger synergies.
➡️Another Approval Timeline Hint
First, lets look my at the prior speculation on timelines.
Speculation #1: Per data posted by Tunnelvisionplenty, there is a big batch of approvals coming 6 months post the 2nd CHM meeting. $NWBO had their 2nd CHM meeting on November 27/28 of 2025. Six months past this date is late May 2026.
Speculation #2: For the first time in the ’25 10k we saw that Advent started DCVax-L specific training which typically takes about six months. I assume they wanted this training to be complete prior to approval. This statement wasn’t in the ’25 Q3 10Q. So, this training likely started October-December ’25 timeframe. That means the training would be complete in the April-June ’26 timeframe.
Speculation #3 (contained in recent 10Q): In this ’26 Q1 10Q we see that $NWBO started a leukapheresis buildout in the UK. I assume this is being timed to be done for the approval decision. The 10Q states that $NWBO expects the buildout “…to be completed by June…”
So, we have three separate signals pointing to approval in May, April-June and finally June. There is an ongoing CHM meeting for May 21/22. Hopefully $NWBO is on the agenda at this CHM and we have an approval decision in mid ’26 as a few speculative timelines are starting to align.
➡️Potential UK Property Sale
"The Company owns a 17-acre parcel of land on the edge of Sawston, UK...If zoned for residential development, the Company has been advised that its property would be extremely valuable."
This is a positive step to possibly address $NWBO’s cash crunch and something to keep an eye on. I would also like to know what the company means by "extremely valuable".
➡️Spoofing Lawsuit Settlement Language
“The funds are being held in escrow while the Company pursues discussions with other lesser defendants about resolution of the case against them. The Company anticipates that the funds will be released from escrow when the discussions with the lesser defendants have been completed.”
That’s a positive sign that some of the smaller players are possibly talking settlement. I’m surprised $NWBO put this language in a public filing. Regarding the statement that the funds will remain in escrow until discussions with lesser defendants have been completed is puzzling. I’m not sure why those funds would be required to stay in escrow until discussions with other parties are complete. The only thing I can think of with my limited knowledge of the situation is that $NWBO sold interest in the lawsuit to certain investors and maybe their agreement stated that the first [insert dollar value] of the settlement goes to paying off the investors. Maybe $NWBO is required to hold the funds in escrow until the settlement has reached a certain amount to pay off the initial investment of the investors. Who knows. It's an unusual statement so I figure it has something to do with the possible unusual arrangement of selling lawsuit interests to investors.
That's all that stood out to me on the commercialization/cash front. Fingers crossed for mid '26 approval decision!
$NWBO
Last November, I had a discussion with a representative of $NWBO who told me, word for word:
“The MHRA has all the information in hand to make a decision…”
Six months later — and now 29 months after the MAA submission — we are still in complete limbo.
Considering the compelling survival data, the strong statistical evidence, and the virtually nonexistent toxicity profile, #DCVAX should have already received a decision.
Meanwhile, the manufacturing facility (Advent/Sawston) has now obtained the necessary approvals to commercially produce the personalized vaccine.
The patients are ready. The company is ready. Shareholders are ready.
Today and tomorrow, the CHM committee meets to determine whether medical products should be approved or not. Hopefully #DCVAX is on the agenda and a positive decision will finally be communicated very soon.
The next step after authorization will be to expand and confirm the vaccine’s effectiveness across additional cancer types.
Time matters. Patients cannot wait forever.
$NWBO Today I transferred $ from my bank to my Fidelity account which I do often and the $ is available immediately to trade. Today I got the error message about having to wait for $ to clear to purchase stocks under $3. I have never received this error message and when I pressed and spoke to supervisor then manager I was told "usually your $ is available right away but this time it was not" (No S Sherlock) When I pressed why he said news is expected. I told him that I believed it was because they need to cover their short positions and are making it harder for retail to buy shares. All of a sudden he was silent after some ohms and ahhhhs and couldn't get off the phone fast enough.
Overall Survival
2.1 months, median benefit for 71 FDA approved solid tumor drugs, from 2002-2014 (only 42% of these met ASCO criteria for "clinically meaningful improvement")
5.4 months, DCVax-L benefit in rGBM (13.2 v 7.8, a 69% gain)
2.8 months, DCVax-L benefit in nGBM (19.3 v 16.5, a 17% gain)
DCVax-L aka Murcidencel is a new Cancer Vaccine
$NWBO $XBI
https://t.co/ZcV6Q9ZUeR
























![hoffmann6383's tweet photo. ✅️Algorithms Discoverable?
The federal magistrate judge in $NWBO's spoofing lawsuit against six of the largest market makers in the world, including Citadel and Vitru, believes that the Defendant market makers' trading algorithms are discoverable
The Magistrate Judge stated, in relevant part:
"I'm not sure how that gets limited, frankly." [1]
See attached Image.
[1] Docket #286, https://t.co/2vLwDOXAki](https://pbs.twimg.com/media/HJ77xJCWcAE5jwb.jpg)