Ahead of the launch of the DSM-5-TR it seems we're gonna be getting much more ignorance and much less bliss for quite some time...
https://t.co/5dZFKsX9CO
It boggles my mind how anyone doing psychotherapy can float off into guru land or feel consistently amazing about their work. Maybe some are legit supershrinks. But as long as one is in supervision or consultation, exposing your work to criticism, this work is so humbling.
@TweetATherapist There is a very telling part of the article, in which a “mainstream” psychologist says “Part of the process of recovering from an eating disorder is to separate yourself from the disorder, but not like that” - There is no substance to the “not like that”… it’s all “like that”
PARTS LANGUAGE ISN’T EXCLUSIVE TO IFS. PARTS LANGUAGE ISN’T EXCLUSIVE TO IFS. PARTS LANGUAGE ISN’T EXCLUSIVE TO IFS. PARTS LANGUAGE ISN’T EXCLUSIVE TO IFS. PARTS LANGUAGE ISN’T EXCLUSIVE TO IFS. PARTS LANGUAGE ISN’T EXCLUSIVE TO IFS. PARTS LANGUAGE ISN’T EXCLUSIVE TO IFS. PARTS!!
@Dooobeedoozy@therealRYC@AdamUrato1 These are certainly as confounded as the schizophrenia study. Plenty of face validity though to the notion that an SSRI has an effect on foetal development, and if that is considered alongside a lack of demonstrable benefit for SSRIs then hard to argue for them.
Maria A Oquendo, the new Chair of DSM-6 (yes it's coming) has received unrestricted educational grants and/or lecture fees form AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, Otsuka, Pfizer, Sanofi-Aventis, and Shire. She receives royalties from the commercial use of....
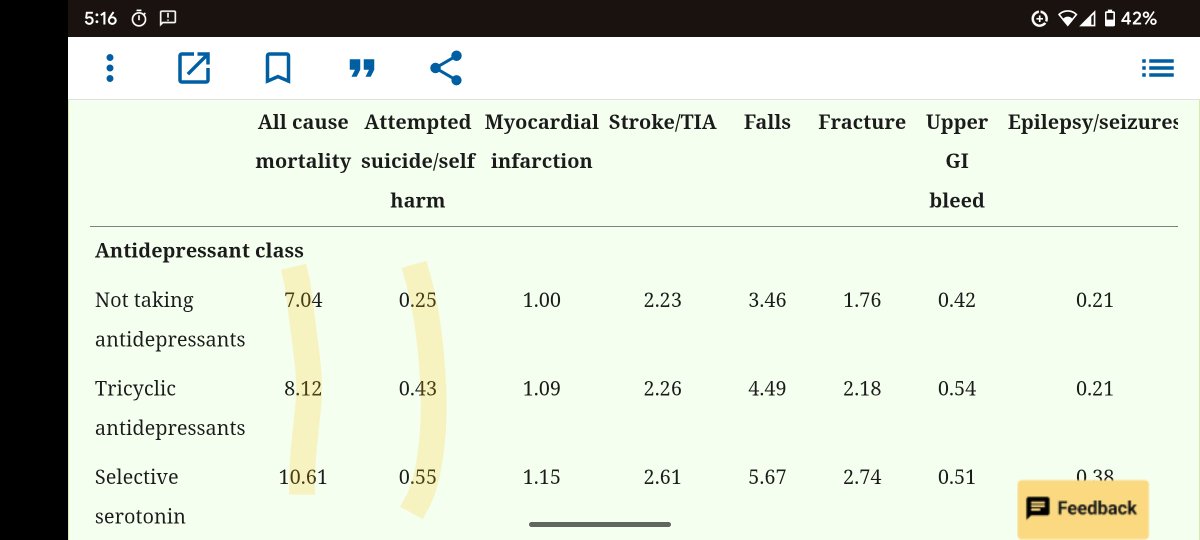
This is totally incorrect. Among the many false claims here, the Coupland study from 2011 found both an increase in all cause mortality and suicidality in adults aged 65+, not a decrease as claimed.
https://t.co/IDWydAVTjW
Stark fact from new paper:
“Countries permitting assisted dying for mental disorder as the sole underlying condition find that" Borderline Personality Disorder is a common reason to request end of life.
https://t.co/vP5PQhZR9N
Canada is about to adopt that permissive policy.
When I was in my very early 20s and in analysis the first time, long before I had decided to become a therapist, long before I knew anything about psychotherapy (let alone psychoanalysis), I fell, for a time, into a common pattern and phase of many patients and analysands. 🧵
RADAR trial data showed people recover to their baseline levels of function and symptoms after a relapse, suggesting the hypothesis that relapse is toxic to the brain is incorrect 1/2 https://t.co/pb1yLMjffQ
Researchers, if you’re comfortable with abuse, post that X issue “has never been studied before”. The online community will do your literature review for you
There were so many examples of psychiatrists post-hoc rationalising their knowledge of AD inefficacy with pen to pad when I was in training it got to be very silly. This was before I started research in nosology but all that silliness was pointing in a certain direction already.
Good to be reminded of this from time to time and to share widely with non-psychiatric colleagues. Rob Howard is hardly alone in this practice: when I was in training I would say the majority of my supervisors said something like this 🧵
Psychiatry professor Robert Howard says at Royal College of Psychiatrists International Congress that depression drugs are no better than placebo in people with dementia but he uses the drugs as placebos because “people get better.” He ignores the drugs have serious harms!