@joostholslag That would be great. To start, any modeling approach that produces executable clinical guidelines would be great.
This is a challenge even without constraints on the used modeling approach.
With experience of executable clinical pathways the standard would eventually emerge 🤞
@ppazos openEHR schemas could be generated. Similar to how they are for OpenAPI by @pieterbos82@sebast_iancu and you.
You are lucky to have your own CDR to test this with.
@ppazos The schema in my case is provided by Camunda. It is the way to communicate with their engine.
#openEHR part is using RM inside BPMN.
I might use openEHR proto messages for frontend (for tasks list app and an app for adapting care plans).
For CDR I'll have to use REST API.
@ppazos @BHaarbrandt @joostholslag@docpaulmiller@ResusCouncilUK I would rather pay somebody who took time to learn #openEHR basics doing my frontend apps then pay 3 others who expect me to hand-hold them through writing vanilla web apps they are comfortable with.
Some apps are focused on CDR. Why not spend some time reading about #openEHR?
@ppazos @BHaarbrandt @joostholslag@docpaulmiller@ResusCouncilUK Since I'm handling both backend and frontend, I appreciate frontend components that are “aware” of the #openEHR DV_ structures that map directly to the openEHR DV_ classes.
I use such components even if the form is completely generated and I could care less about their code 😊
@joostholslag@ppazos@Nedaphealthcare@pieterbos82 Maybe some frontend apps use only your CDR API which simplifies it for the developers. If CDR API and Ruby API are used at the same time, I would rather use only Ruby API (which talks with CDR). 3/3
@joostholslag@ppazos@Nedaphealthcare@pieterbos82 Talking to a CDR directly from a frontend app feels like directly inserting into a database. However since you put an API in front of the CDR it is just a 2nd backend (like the one in Ruby). 1/3
@joostholslag@ppazos@Nedaphealthcare@pieterbos82 I would still rather have a single backend per frontend app which talks to other APIs/backends. User authentication/authorization is simpler that way. 2/3
@ppazos Thank you for these thoughts. I'm starting to work on such an architecture and made the same notes just a few hours ago 😊
It feels good you think the same about the architecture and use of #CDR, #frontend, #backend, #workflow.
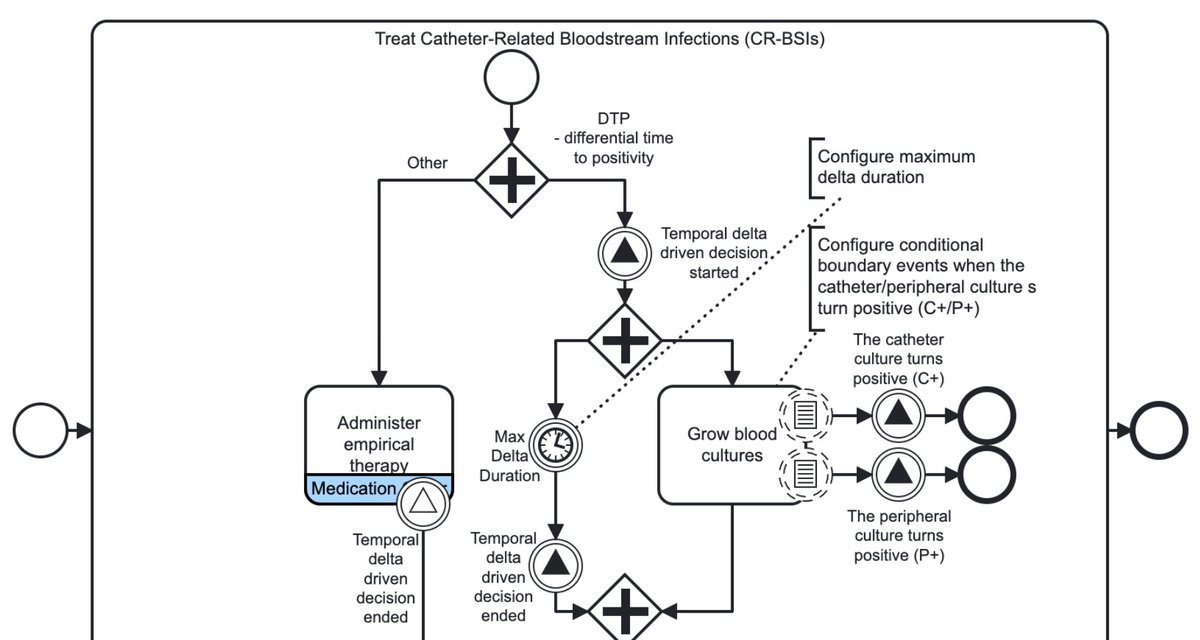
Research papers propose #BPMN extension to limit temporal distance between any non-consecutive process elements.
That is visually appealing but the engine doesn’t execute it.
So I created an inter-activity duration constraint that #Camunda can execute:
https://t.co/7MwWFPAU4d
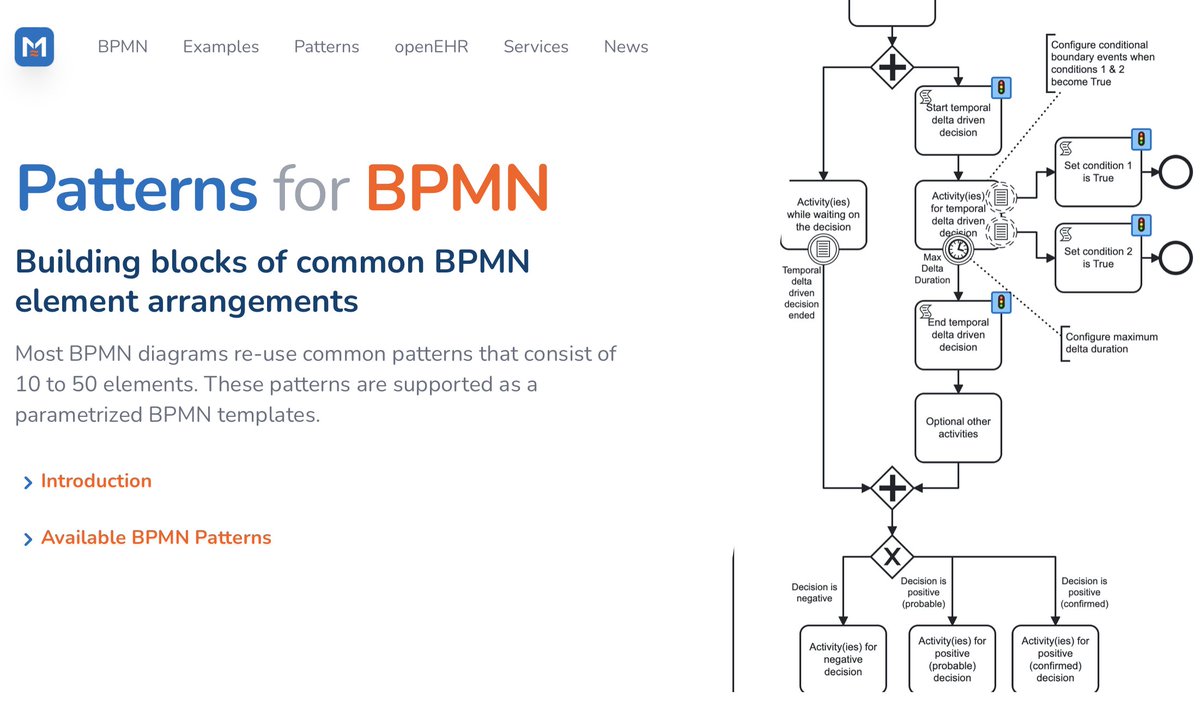
@Camunda Lets use patterns instead of extending the standard 😊
I implemented 4 groups of patterns in Camunda #Modeler:
✅ Temporal
✅ Repeat
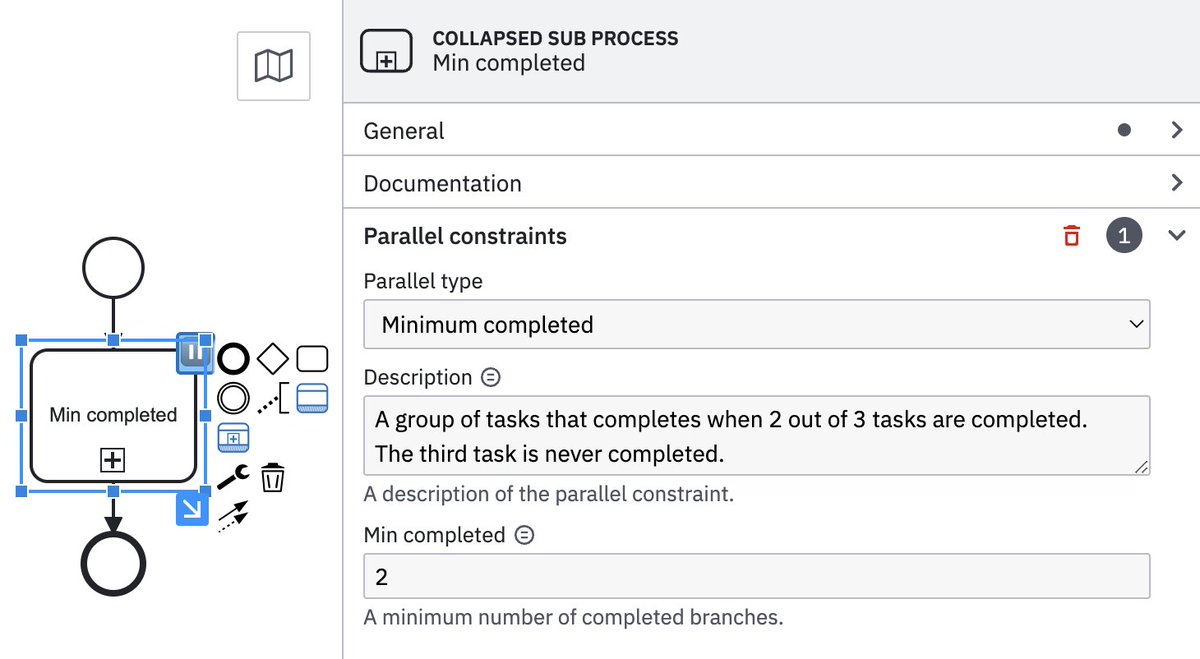
✅ Parallel
✅ Exclusive resource lock
They are all executable on a standard #Camunda engine.
https://t.co/pi7YYsJRV8
@ErikSundvall@bjornna @DIPSASA Nice UI!
My first attempt was Node-RED: https://t.co/Iu5mHCwleX - similar but open-source.
I switched to #BPMN and #Camunda (also open-source): https://t.co/xWTbBW3rfa
If we manage to convert clinical guidelines into executable form, we should use non-proprietary tools.
@GeoffCardwell@Trisotech@BPMPlusHealth The BPMN Quick Guide is meant as a simple introduction for those without any BPMN experience.
I couldn’t find a PDF version of it but it doesn’t take a long time to read its online version (maybe on a tablet).
Here is a short introduction from #ChatGPT:
@BHaarbrandt Since everybody has been chatting with ChatGPT (instead of working), I decided to ask it to do some work for me. It wrote the introduction for #BPMN patterns:
https://t.co/TSDijBdlMR
I only changed "business processes" to "processes" since they are for clinical processes.
@atthatmatt@wolands_cat@rikrenard To do all that, it would need to know what “the correct” pathway should be.
ChatGPT can't do it:
https://t.co/dCkqd6S9nW
The LLMs at this stage need somebody to teach them how the correct clinical pathway(s) looks like. They need examples first.