Dyslipidemia in Older Adults: Balancing Prevention and Individualized Care: @JACCJournals#CVAging
🥸 Our new manuscript published in JACC as commentary on the new dyslipidemia guidelines as it relates the older adult populations - work led by @MichaelGNanna
😱 In simple language, what would you do if you see an 85 year old patients with dyslipidemia: here is the summary below:
👇👇👇
Subacute coronary artery occlusion: complexities of the grey zone: @ESC_Journals
🥸 Nice focused issues on interventional cardiology in the European Heart Journal
👇👇👇
Work started with the @US_FDA many years ago accumulating all of the PCI trials submitted for approval by FDA to the US market - led by our mentor Dr Batchelor.
I will summarize!
I had great time at Inova!
👇🏻
#HeartFailure (HF) affects more than 64 million individuals worldwide, and acute HF is associated with 1-year mortality rates of 23.6% in North America and Europe.
Cardiac resynchronization therapy restores synchronous ventricular activation in patients with HF, reduced LVEF, and left bundle-branch block, or in those requiring chronic ventricular pacing, and may improve LV function, decrease HF hospitalizations, and reduce mortality. 🧵
🔗 Learn more in this JAMA Review: https://t.co/HYZqQg8rzi
The cardiology community has lost a giant. We honor the extraordinary legacy of Eugene Braunwald, MD, MACC, a visionary leader and pioneer whose outstanding contributions shaped the foundation of cardiovascular medicine as we know it today.
Read more: https://t.co/uaC2n4m5gD
The American Heart Association mourns the passing of the legendary cardiologist Eugene Braunwald, M.D., widely recognized as one of the most influential figures in the history of cardiovascular medicine. Over seven decades, his work reshaped the understanding and treatment of heart disease, leading many to call him the father of modern cardiology.
Braunwald was a lifelong contributor to the American Heart Association, helping advance its research and scientific mission, and was honored with some of the Association’s highest honors for his lasting influence on cardiovascular care and research. His influence extended well beyond his own discoveries, as generations of Association‑supported investigators, clinicians and academic leaders were trained by Braunwald or guided by the clinical trial standards and mentorship models he helped establish.
https://t.co/ieZuHYMyOP
HF with mildly reduced EF (HFmrEF) sits between HFrEF & HFpEF; where does it truly belong?
A new HFSA Scientific Statement examines its epidemiology & pathophysiology & provides a comprehensive management framework for this understudied HF phenotype🫀
🔗 https://t.co/pP2WihJQxc
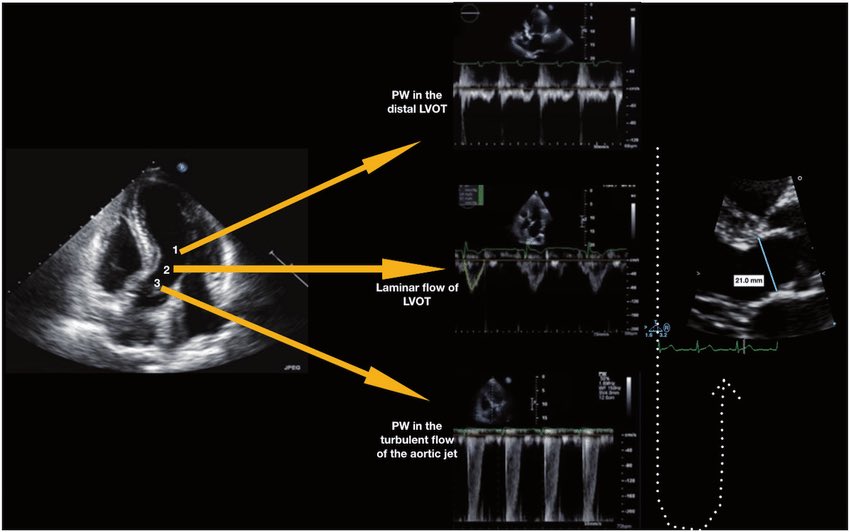
🫀 Did you know where the recommendation to place the pulsed wave Doppler sample volume 0.5–1 cm from the aortic valve to measure LVOT VTI comes from?
The answer is more interesting than it seems. It doesn’t come from a single study or an experiment designed for that purpose. It comes from a historical chain spanning nearly 40 years:
🔬 1982–1984 — The physical foundation
Pasipoularides and Murgo demonstrated using invasive catheters and mathematical models that in aortic stenosis there is a real zone of flow acceleration in the LVOT, just proximal to the valve, without any second anatomic obstruction. Pure hemodynamics — no Doppler yet.
👉 Bird et al. Circulation 1982 → https://t.co/oCXGNgWsPF
👉 Pasipoularides et al. Am J Physiol 1984 → https://t.co/cfvNMpEgzG
📐 1984 — The apical 5-chamber view
Lewis, Kuo and Quinones were the first to validate cardiac output measurement using pulsed wave Doppler from the cardiac apex. They described placing the sample volume “immediately proximal to the aortic valve leaflets” — but without specifying any distance in centimeters.
👉 Lewis et al. Circulation 1984 → https://t.co/lRVjLuYMEs
📏 1985 — The first numerical distance
Skjaerpe, Hegrenaes and Hatle (the Norwegian group) were the first to quantify this in Doppler: they empirically observed that flow acceleration began 0.5 to 1.5 cm proximal to the valve, and placed the sample volume just proximal to that zone. They directly cited Pasipoularides as supporting evidence. This was the first time a numerical distance appeared in the technique.
👉 Skjaerpe et al. Circulation 1985 → https://t.co/rf7l2FQUs4
📊 1986–1988 — Practical consolidation
Otto et al. used ~1.0 cm. Oh, Tajik and the Mayo Clinic group explicitly established the range of 0.5 to 1.0 cm in 100 patients, justifying it as necessary to avoid the subvalvular acceleration zone. This is the figure we all recognize today.
👉 Otto et al. JACC 1986 → https://t.co/avke1qOy4x
👉 Zoghbi et al. Circulation 1986 → https://t.co/KFiChfBNuc
👉 Oh et al. JACC 1988 → https://t.co/1C8sHRSMPq
📋 2002 — It becomes “official”
Quinones, Otto, Zoghbi and colleagues codified it in the ASE guidelines as “~5 mm proximal to the aortic valve”… but without citing any specific study to support it. It had already become expert consensus.
👉 Quiñones et al. JASE 2002 → https://t.co/U3hXFns4jx
⚔️ 2017 — The debate reopens
Baumgartner et al. (EACVI/ASE) maintained the 0.5–1 cm recommendation. However, Hahn and Pibarot responded with a critical letter pointing out that the original articles from the 1980s measured at the aortic annulus, not 0.5–1 cm below it, and that moving away from the annulus introduces errors due to the elliptical and irregular shape of the subannular LVOT.
👉 Baumgartner et al. Eur Heart J Cardiovasc Imaging 2017 → https://t.co/iu07xBTwQS
👉 Hahn & Pibarot. JASE 2017 → https://t.co/uqgcv8kzO7
💡 Bottom line:
The 0.5–1 cm figure was never experimentally validated as the optimal distance. It emerged from empirical observations in the 1980s aimed at avoiding a flow acceleration zone that had been demonstrated with invasive catheters. It was adopted through accumulated clinical practice and later elevated to a formal recommendation by consensus. The debate over whether to measure at the annulus or 0.5–1 cm below it remains open to this day.
One of those recommendations we all follow but few know where it actually came from 🙂
Dr Benigno Valderrábano Salas
@MDBeni@JaeKOh2@ottoecho@WilliamZoghbi@ASE360@EACVIPresident@NephroP@iamritu@PPibarot@hahn_rt@MAecocardio@SISIACOficial@SONECOM_AC@VazyurVasquez@Cardiotweets83@HEARTof_echo@echobasics
🧲CMR findings in mitochondrial disease: a guide for clinicians🧵 Tweet 1/5
🫀⚡ Not all LVH is sarcomeric HCM
Up to 30% of patients with mitochondrial disease have cardiac involvement.
The heart is often the first clue 👀
#CardioTwitter#WhyCMR#Cardiology#FOAMed
🫀🔥 LDL is controlled. Statins are optimized. And yet… patients still have events.
This study addresses one of the most important unanswered questions in cardiology:
👉 What really drives residual cardiovascular risk?
📊 In >9,400 statin-treated patients with LDL <70 mg/dL undergoing PCI:
Patients were stratified by:
Triglycerides (TG ≥150 mg/dL)
Inflammation (hs-CRP ≥2 mg/L)
💡 The result is striking:
👉 Inflammation—not triglycerides—drives risk
Residual inflammatory risk → ~1.8x higher MACE
Combined TG + inflammation → ~1.9x higher MACE
Residual TG risk alone → NO significant increase
⚠️ And what’s driving this?
👉 Mostly all-cause mortality
Not subtle. Not marginal.
👉 Clinically meaningful.
🧠 Let’s be clear:
We’ve spent decades optimizing:
✔ LDL
✔ Lipid profiles
✔ Cholesterol targets
But this study shows:
👉 You can win the lipid battle… and still lose the war
🔥 Because atherosclerosis is not just lipid-driven.
👉 It’s an inflammatory disease
🎯 Clinical implication
Risk stratification cannot stop at LDL.
We need to integrate:
hs-CRP
Inflammatory burden
Systemic biology
🚀 Paradigm shift
From:
❌ “How low is LDL?”
➡️ to
✅ “How active is the disease?”
🧠 Bottom line
Lowering LDL is necessary.
👉 But it is NOT sufficient.
If inflammation persists:
👉 Risk persists.
⚡ The future of prevention?
Not just lipid control.
👉 Inflammation-guided precision cardiology.
🫀 Sepsis-induced cardiomyopathy is not rare. It is under-recognized.
And more importantly:
👉 It is dynamic, reversible… and frequently misinterpreted
⚠️ The clinical trap
You see a septic patient with:
✔️ Hypotension
✔️ Vasoplegia
✔️ “Normal” or even high LVEF
👉 And you assume the heart is fine
❌ Wrong
🧠 What septic cardiomyopathy really is
Sepsis-induced cardiomyopathy (SICM):
▪️ Acute, reversible myocardial dysfunction
▪️ Can affect LV, RV, systolic and/or diastolic function
▪️ Not related to coronary disease
▪️ Often unmasked after resuscitation
👉 It may appear hours to days after ICU admission
🔥 Phenotype matters!
SICM is NOT one disease.
It is a spectrum of hemodynamic phenotypes:
🟠 LV systolic dysfunction
🔵 Hyperdynamic vasoplegic state
🟣 RV failure
🟡 Persistent hypovolemia
⚪ Apparently “normal” profile
👉 Each requires a completely different treatment strategy
🚨 Why LVEF misleads you
In sepsis:
➡️ LVEF depends on afterload
➡️ Vasoplegia can artificially increase LVEF
➡️ “Normal EF” ≠ normal contractility
👉 Ventriculo-arterial coupling is the real issue
🫀 Pathophysiology
Sepsis affects the heart at every level:
▪️ Cytokine storm → myocardial depression
▪️ β-adrenergic downregulation → poor response to catecholamines
▪️ Calcium handling dysfunction → ↓ contractility
▪️ Mitochondrial failure → ↓ ATP
▪️ Microcirculatory dysfunction → impaired perfusion
👉 Yet: minimal cell death → reversibility is possible
⚡ Clinical reality
SICM can:
✔️ Develop early OR late (up to 72h)
✔️ Mask or mimic other shock states
✔️ Coexist with AMI
✔️ Flip phenotype during resuscitation
👉 This is why single measurements are dangerous
🧩 Management principle
There is no universal treatment
Instead, Treat the phenotype, not the label
Examples:
🟠 LV failure → consider inotropes (carefully)
🔵 Hyperkinetic vasoplegia → vasopressors, avoid overload
🟣 RV failure → ventilatory strategy + afterload reduction
🟡 Hypovolemia → guided fluids
👉 Echocardiography is the cornerstone
🚀 Where the field is going
Future management will rely on:
▪️ Hemodynamic phenotyping
▪️ Biomarker + immune profiling
▪️ AI-guided decision making
▪️ Personalized therapy
👉 Not “one-size-fits-all sepsis bundles” anymore
🎯 Take-home
Septic shock is not only a vascular disease, It is a cardiovascular syndrome with multiple phenotypes
And if you miss the cardiac component You miss the patient ⚠️
📚 Aissaoui N et al. (2025)
European Heart Journal
DOI: 10.1093/eurheartj/ehaf340
Left Ventricular Unloading in Anterior STEMI without Shock: The STEMI Door to Unload (DTU) Randomized Controlled Trial: @JACCJournals
🥸 Here is a synthesis to Door to Unload and key market implications from this trial.
😱 Happy Saturday.
👇👇👇
Asundexian for Secondary Stroke Prevention: @NEJM
🥸Asundexian at a daily dose of 50 mg on the risks of ischemic stroke and major cardiovascular events?
👇👇👇
Bleeding Risk with Apixaban vs. Rivaroxaban in Acute Venous Thromboembolism: @NEJM
🥸Apixaban vs Rivaroxaban: Results from the COBRRA Trial
😱 Important for older patients
👇👇👇
Left Atrial Appendage Closure or Medical Therapy in Atrial Fibrillation: @NEJM
🥸 The controversy in LAA closure
😱 I summarized it before when it was presented at @AHAScience but here you go...
👇👇👇
Risk-Guided Antihypertensive Treatment Eligibility in Older Adults Under Updated Hypertension Guidelines: @AnnalsofIM
🥸 Our new publication in the Annals of Internal Medicine led by @MichaelGNanna
😱 Question is: the new guidelines introduced the PREVENT risk equations, with a recommended threshold of 7.5% or higher to guide treatment decisions -
🥸To evaluate the effect of these new recommendations by exploring how risk-guided therapy would affect pharmacotherapy recommendations in people aged 65 years or older.
😱Here is a summary of the paper: bravo to the Heartwise Lab members.
👇👇👇