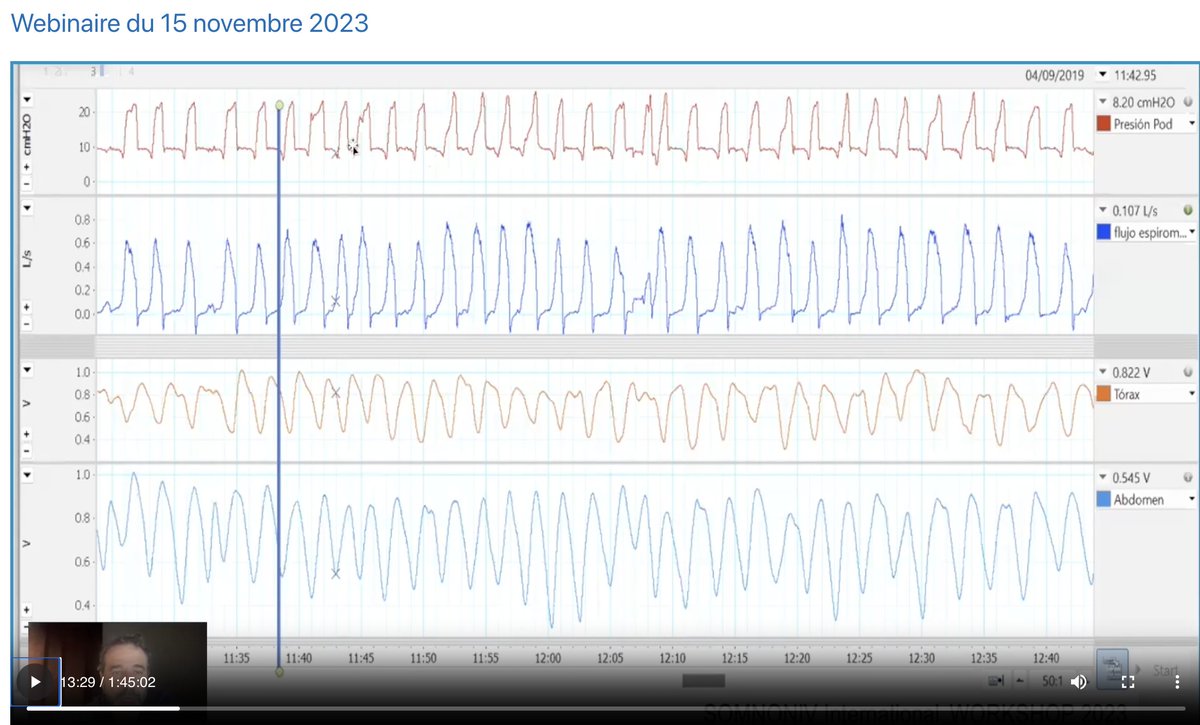
Nice first webinar for difficult traces with the SOMNONIV group, congratulations to the experts who found all the causes! not so obvious...do no be depressed...it was expert level...https://t.co/pGsrccTTE1
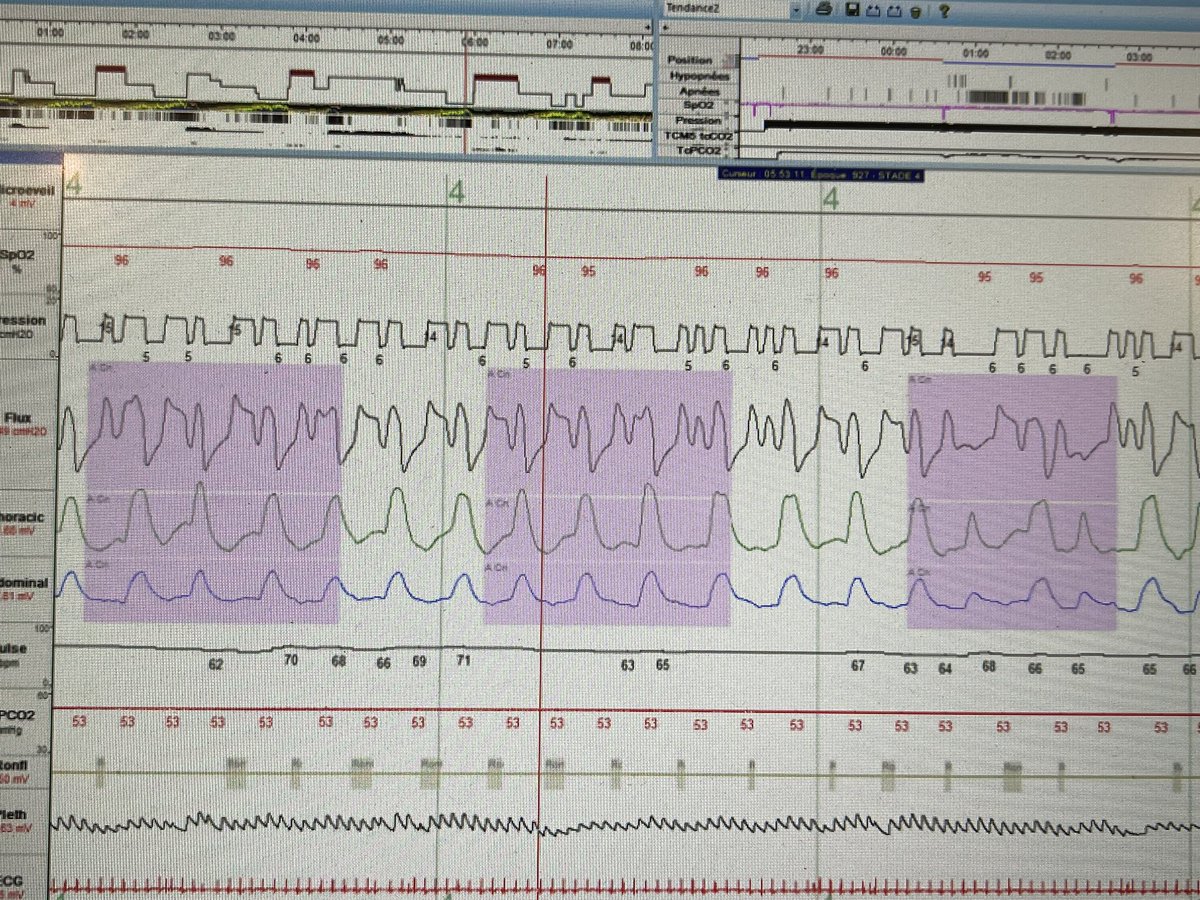
Always the same question with Cheyne Stokes ventilation…are upperairway opened or closed during the « central » event. Here a CS in post stroke. Your opinion?
Le questionnaire sur le monitoring est toujours en cours, nous avons 75 réponses, merci de rajouter les vôtres pour monter à 100!!
https://t.co/XV3JAwHUwk
What are these big abdominal movements? spontaneous ventilation and the traces are (spo2/nasal flow/thermistance/ thorax and abdominal belts) ….our hypothesis leg movements…what do you think?
Copd patient with Paco2 at 50mm d’hg during the day….would you ventilate this patient? A polysomnography would ve very usefull but as the delay is 3 months….we are going to ventilate him…that’s real life…and that’s probably why copd is the first pathology ventilated at home
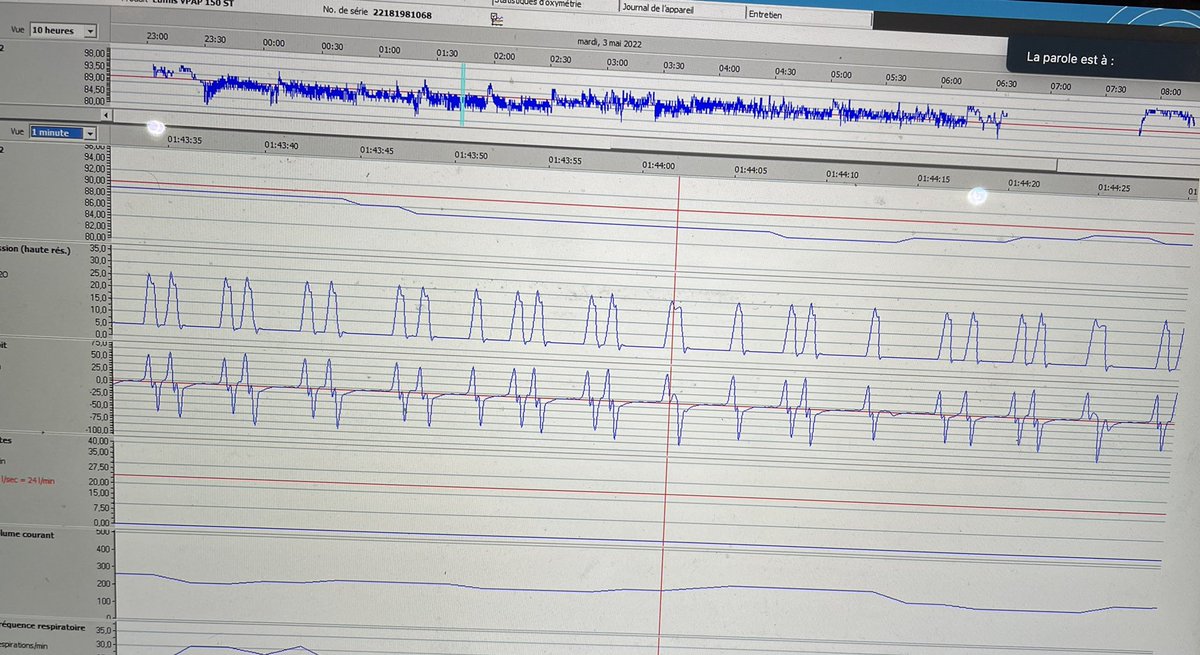
Severe COPD patient, Paco2 48mmhg under niv…the zero line is badly calculated by the software or massive autoEpap? The inefective efforts confirm that it is autoPep…what to do? That’s another question😨
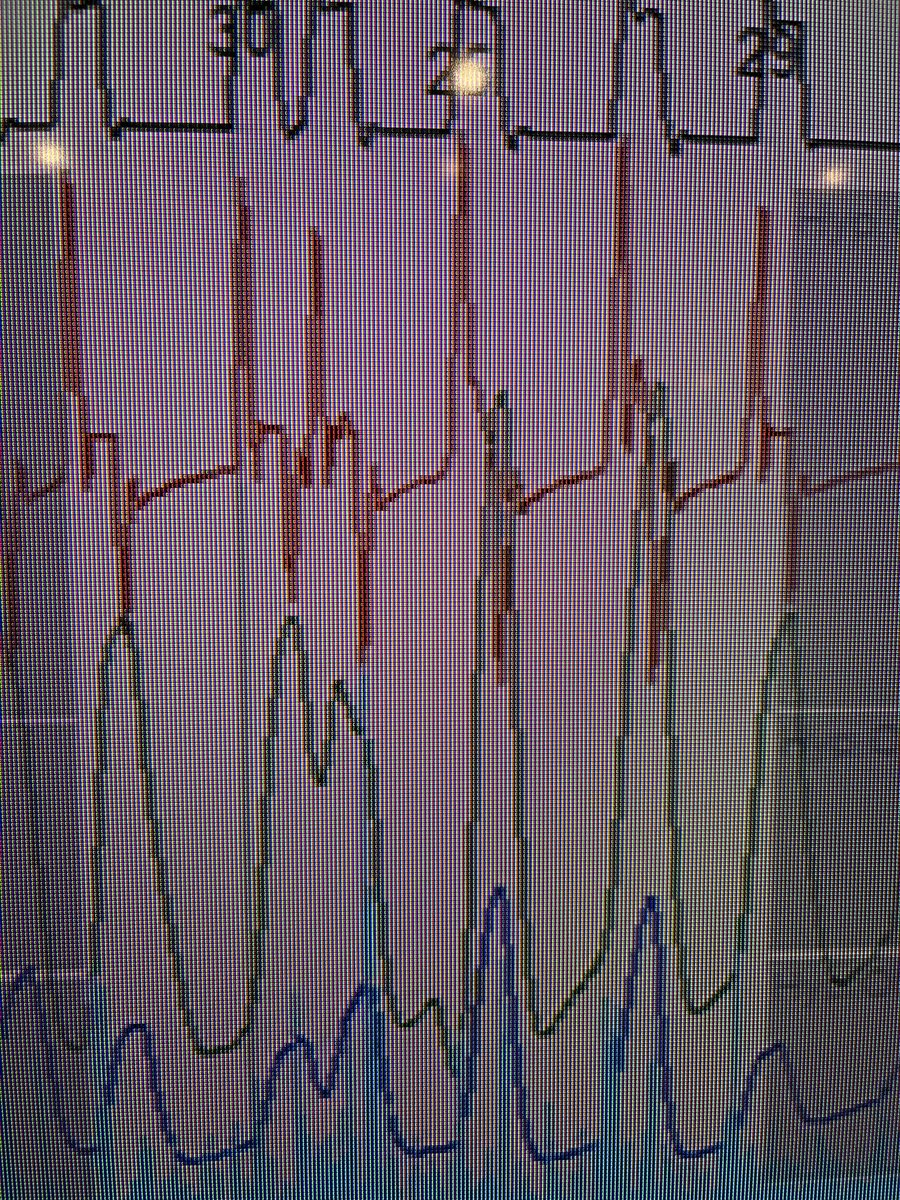
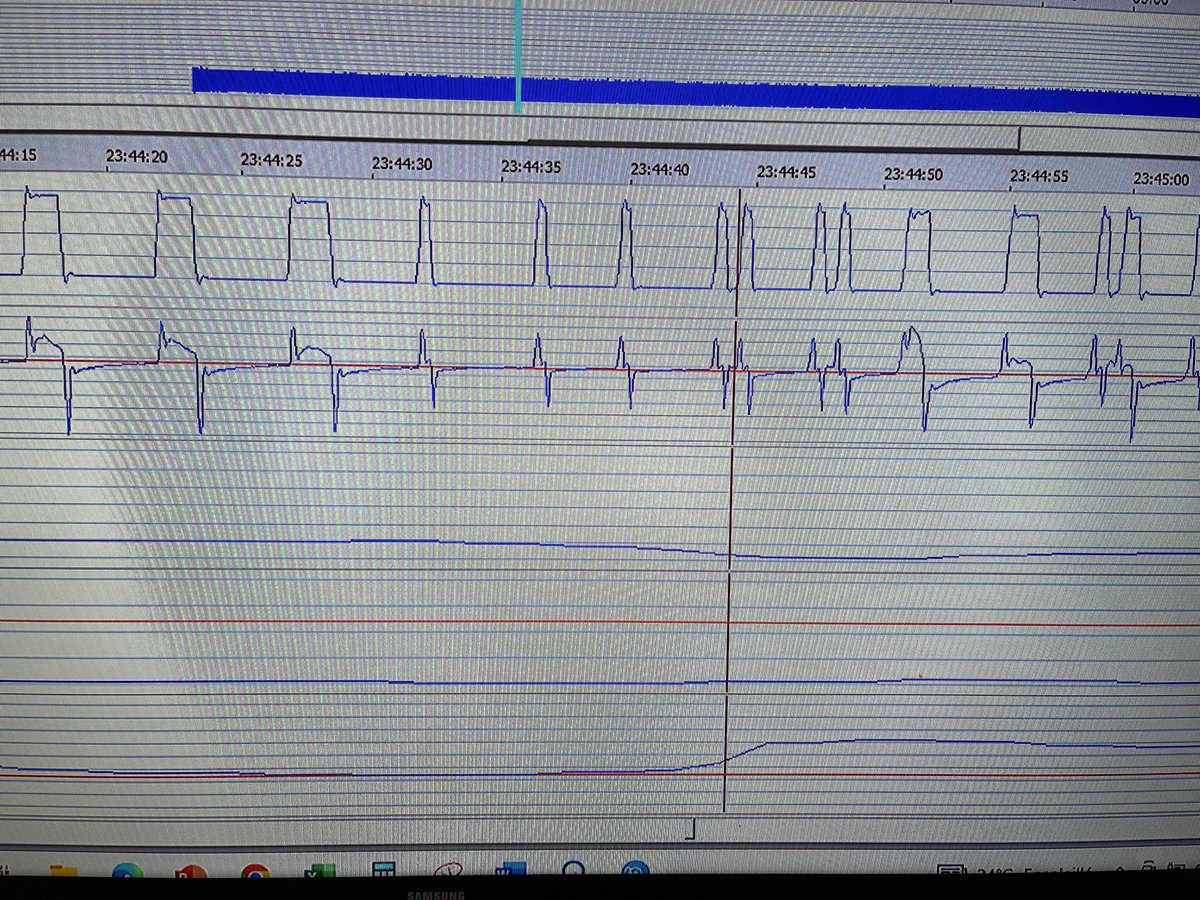
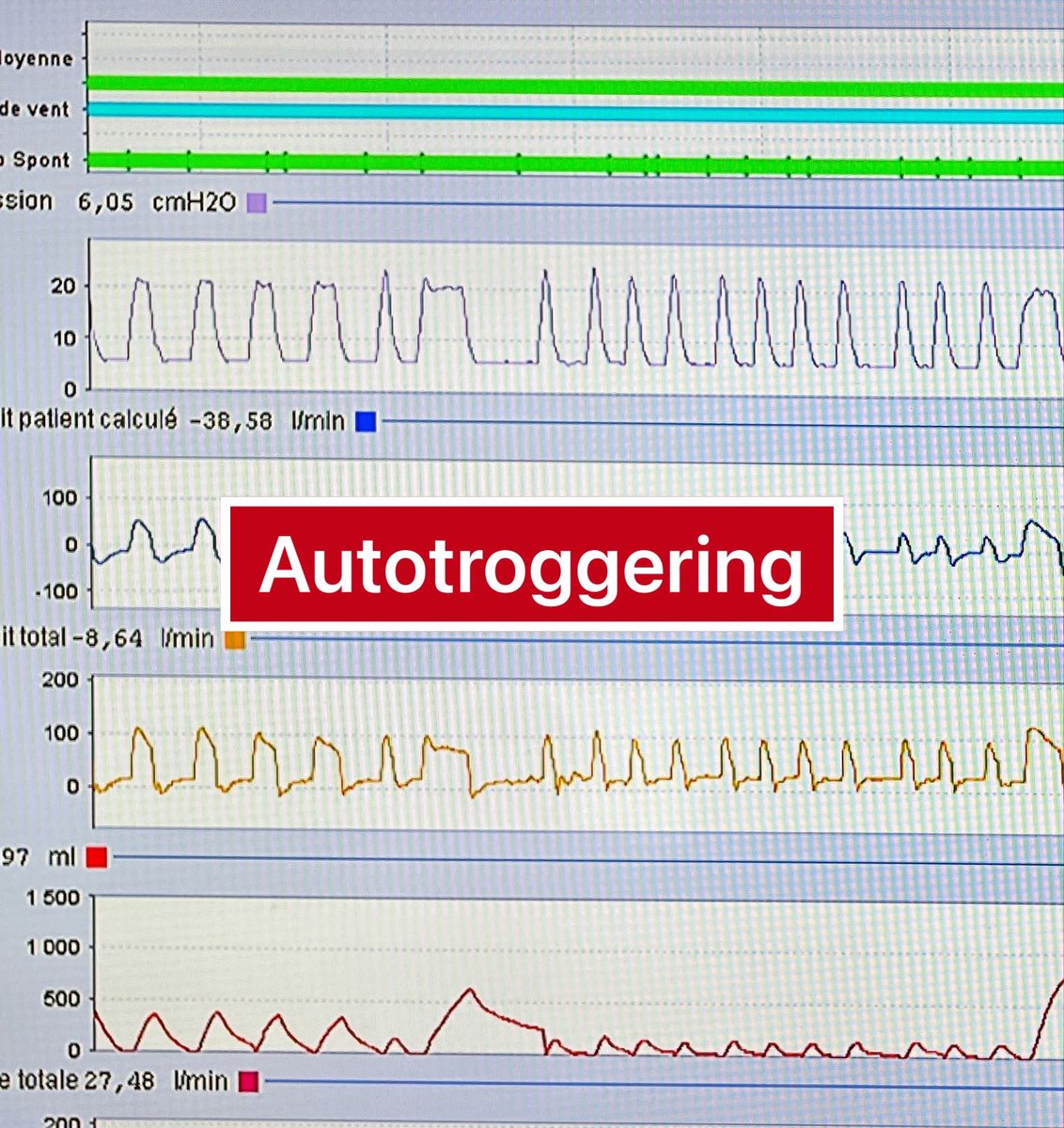
Autotriggering yes! but due to obstructions… (decrease of the flow). Here we just change the trigger that was very sensitive…few obstructions that we respect
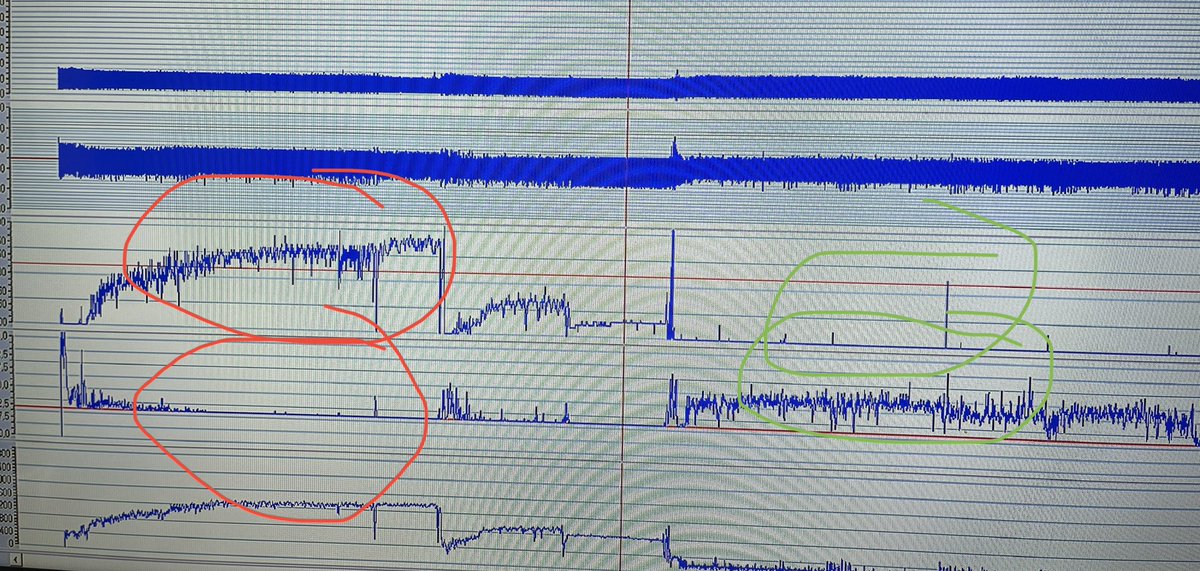
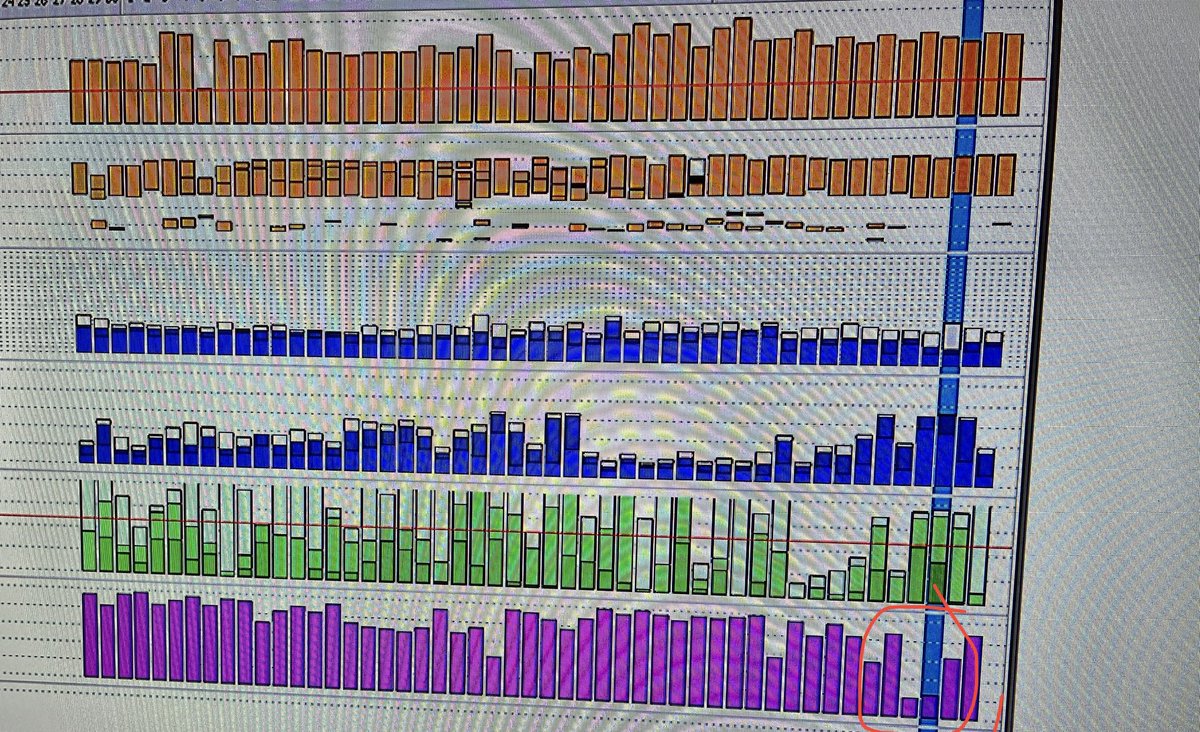
A good indirect sign for leaks : when the triggered cycles decrease and the control cycles (wrongly due to leaks (red circles) increase…decrease the triggered cycles is not always a good point!
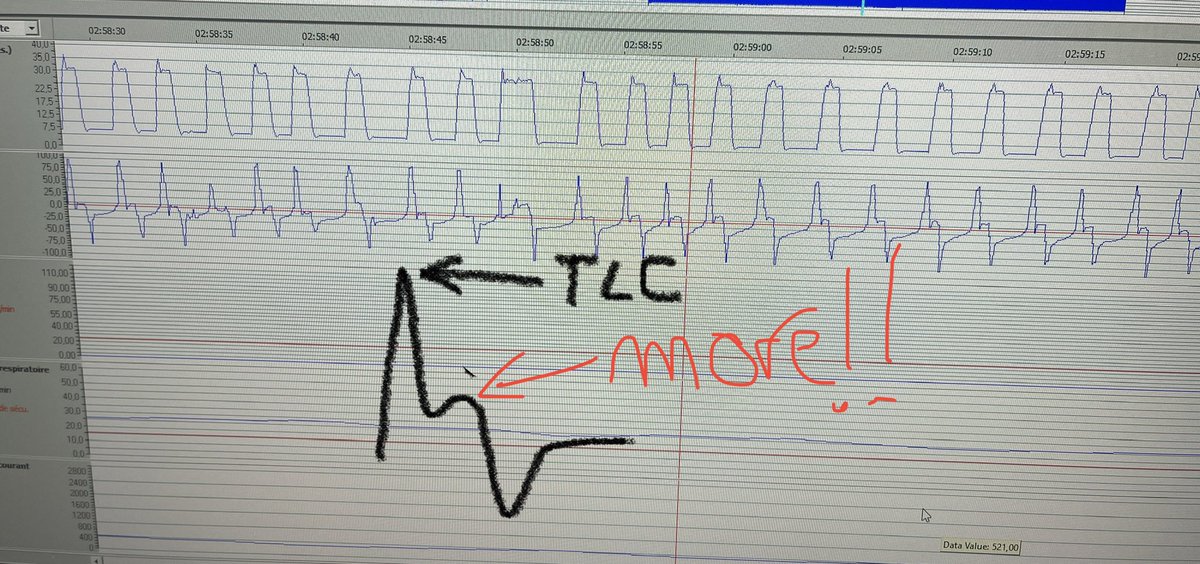
Copd are difficult patients to ventilate!!! Even if the Paco2 is normal (from 68 to 48 today!!) but even with very high IPAP sometimes the lung is at this maximum…even if the ventilator AND the patient would like more