@AmitSegal no one is stopping your dumbass , or your country to invade and fight a ground war in iran for regime change fuck face. it’s not in the interests of the american taxpayer or the american servicemen or the american people. got that fuck face ?
Cold plunges are the epitome of influencer 'lifemaxxing' nonsense. The @hubermanlab claim about a 250% dopamine surge is a misunderstanding. It's a measure of dopamine in the body, not the brain and just reflects shivering and the need to pee. There's no good evidence for the Wim Hof Method. It blunts muscle growth, and the cardiac strain can be dangerous. It's great if your goal is being cold but otherwise is just a performative waste of time - better to spend the time reading classic books.
Tens of millions of people in the U.S. have elevated Lp(a), an inherited and largely hidden driver of heart disease.
A drug trial to address it is expected to report results soon. 🔗 https://t.co/wmgLRY3jrZ
RAS finally getting drugged is one of the great stories in modern biology, and almost nobody outside oncology understands why it's such a big deal.
YOU'LL LEARN SOMETHING AWESOME TODAY.
i am going to keep this as understandable (and simple) as i can.
OPEN THE THREAD.
🧵
This has quietly been a miracle month in medicine.
In the last 5 weeks we’ve got news on:
- retatrutide, the triple agonist GLP-1 from Lilly, basically melting fat and body-wide inflammation at record levels
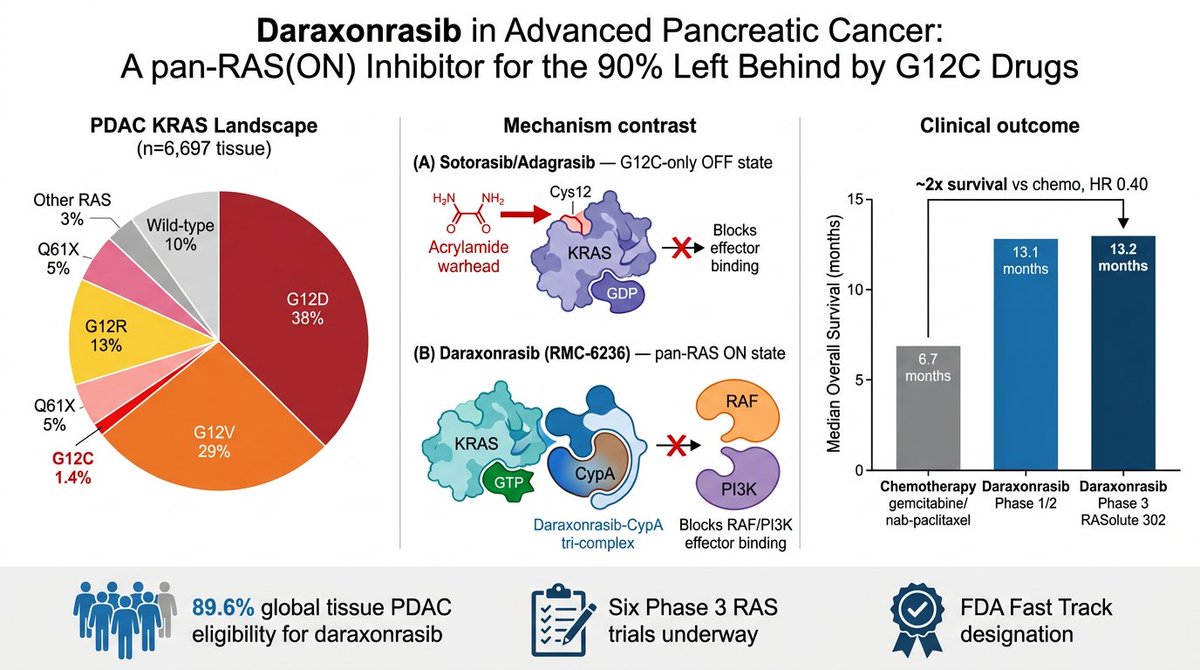
- RevMed’s new pancreatic cancer drug showing unprecedented abilities to extend life
- small trial of a one-and-done PCSK9 gene editing therapy for slashing LDL cholesterol
- Mayo’s AI-assisted radiology showing vastly improved cancer detection
- this new therapy for metastatic solid tumors
This stuff is at varying levels of evidence. Retatrutide is ~100% on its way, other stuff needs more clinical trial data. But put it together and we’re maybe on the verge of majorly reducing the mortality of heart disease and cancer, the two leading causes of death in America.
Presented at #ASCO26:
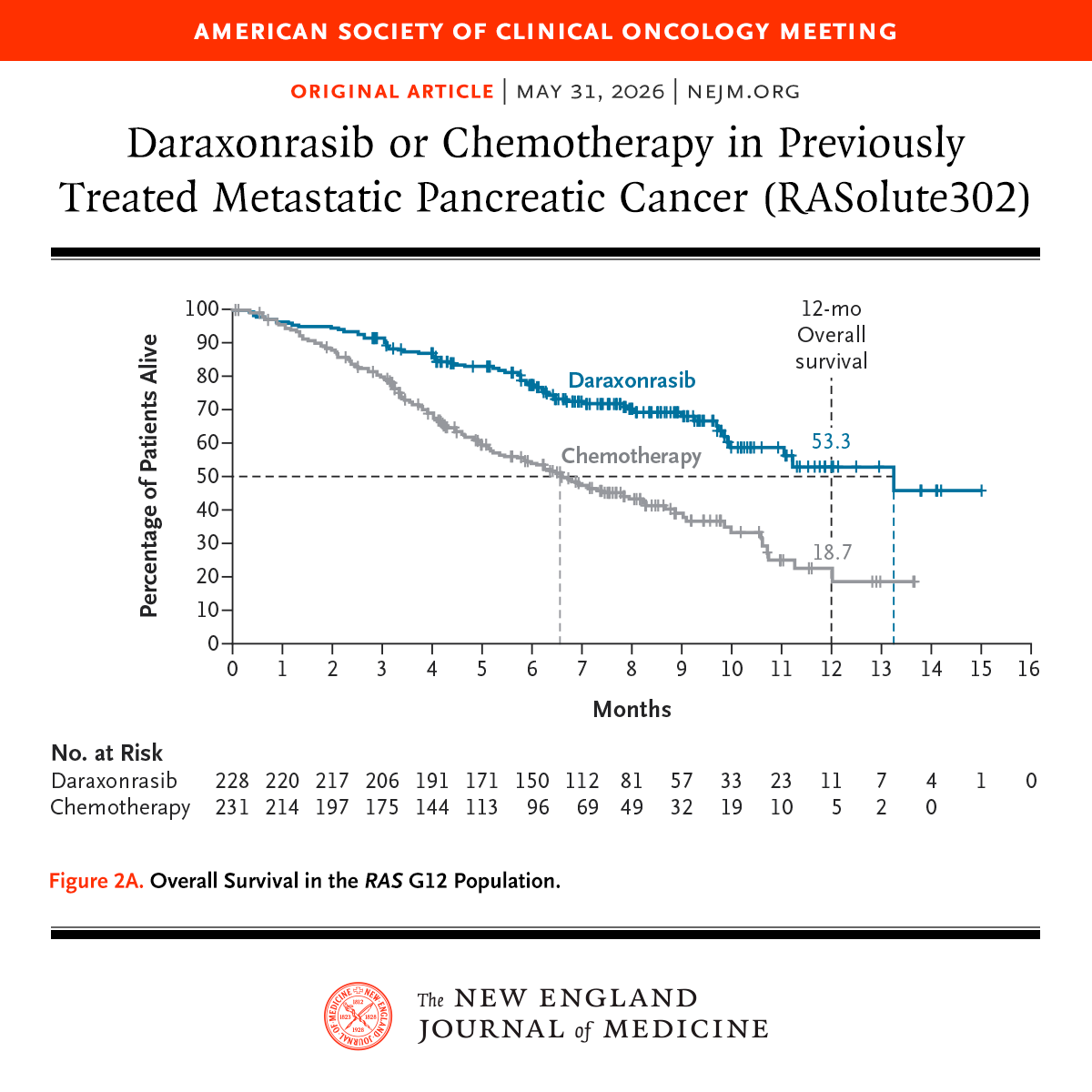
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
Retatrutide, a triple receptor drug for GLP-1, GIP, and glucagon, is the most powerful weight loss drug yet. A significant issue is too much weight loss among the trial participants. New randomized trial results announced today with 28% body weight loss.
gift link https://t.co/82tRkOvQ49
💊 Practical algorithm for diuretic resistance in acute HF from #HeartFailure26— this is the slide to save!
Start: Furosemide 120-160 mg
↓ Still congested?
Add Chlortalidone 12.5-50 mg/24h
↓ Still congested?
Tailor to the problem:
• Metabolic alkalosis → Acetazolamide 120-500 mg/24h
• Hyponatremia → Tolvaptan 15-50 mg/24h
• rLVEF + hypopotassemia → MRA 25-100 mg/24h
And running through the whole algorithm:
➕ Add iSGLT2 throughout
➕ Add sacubitril/valsartan if LVEF <49%
➕ Consider parenteral route if oral absorption is the issue
Clean. Practical. Evidence-based. 💯
(Adapted from de la Espriella R et al. Nefrologia 2021)
#CardioTwitter #HeartFailure #Cardiology #Diuretics #HFrEF
🫀⚠️ SCOT-HEART changed cardiology with one simple idea:
👉 First scan. Then treat.
This is going to generate some hitching to some colleagues within the community 😁. Sorry about that.
And 10 years later…
the message is even more disruptive.
For decades, we built cardiology around:
👉 ischemia
👉 stress tests
👉 flow limitation
Find ischemia.
Open arteries.
Simple.
Except… it didn’t reduce hard events consistently.
SCOT-HEART helped expose the problem:
👉 Atherosclerosis—not ischemia—is the real disease.
At 10 years:
👉 coronary CT guidance reduced:
- coronary death
- non-fatal MI
despite:
❌ NO increase in revascularization
Let that sink in.
Patients did better NOT because we opened more arteries.
They did better because:
👉 we identified plaque
👉 intensified prevention
👉 treated biology earlier
The most important number may not be stenosis anymore.
It may be:
👉 total plaque burden
👉 plaque phenotype
👉 lipid-rich disease
👉 adverse plaque features
The paper says it clearly:
Patients with:
⚠️ low-attenuation plaque
⚠️ positive remodeling
had dramatically higher event rates.
This is the paradigm shift
From: ❌ ischemia-centered cardiology
To: 👉 plaque-centered prevention
And the implications are enormous.
Because suddenly:
👉 non-obstructive CAD matters
👉 “normal” stress tests become insufficient
👉 anatomy alone becomes incomplete
Even more interesting
The next frontier is already here:
⚡ Photon Counting CT
⚡ AI-driven plaque analysis
⚡ Radiomics
⚡ Quantitative phenotyping
My take
SCOT-HEART did not simply validate coronary CT.
It challenged the entire logic of modern cardiology.
We used to ask: 👉 “Is this lesion ischemic?”
Now the real question is: 👉 “How biologically dangerous is this patient?”
Bottom line
The future is not:
👉 detect stenosis
👉 react late
It is:
👉 detect atherosclerosis early
👉 personalize prevention aggressively
⚡ Because myocardial infarction often starts long before ischemia appears.
#SCOTHEART #CCTA #Cardiology #Atherosclerosis #PlaqueImaging #Prevention #PhotonCounting #AI #PrecisionMedicine
The 2026 ACC/AHA Dyslipidemia Guidelines now officially promote coronary artery calcium as a Level 1 class of recommendation - not once, but 6 times. The final step in the 36 year journey since Agatston published the first paper in 1990. @khurramn1@RonBlankstein@rblument1
CAC testing has become a big part of my prevention practice. I don't use it to decide whether to look for ischemia - a history can do that for most pts. I use it to decide intensity of therapy. I believe pretty firmly that most pts with CAC >0 should be driven to LDL <55.