Bronchovascular texture pattern on quantitative CT reveals airway and vascular remodeling in post-COVID-19 Lungs
🚨"Your lungs still remember COVID, 3–4 years later."
➡️Interesting USA study(pulmonary function tests (PFTs) and inspiratory/expiratory CT scan),
➡️Longitudinal study of 80 post-COVID survivors (81% pre-Alpha strain) scanned at ~5 months (V1) and 3–4 years (V2) post-infection vs 78 healthy controls,
➡️Pulmonary function tests mostly normal, but persistently lower DLCO at both time points,
➡️Early abnormalities (functional small airway disease % and ground-glass opacity %) largely resolved by V2,
➡️BUT, persistent structural remodelling at 3–4 years:
→Increased bronchovascular texture percentage, airway narrowing + wall thickening, shift from large to small airways, and small-to-large vessel redistribution,
→a signature of microvascular pathology, consistent with the known endothelial tropism of SARSCoV2 and the persistent perfusion abnormalities seen in long COVID!
➡️These changes correlated with significantly worse quality of life (SGRQ) and ongoing symptoms (fatigue, cough, brain fog, hypertension),
➡️Reinfections / Vaccination:
The study does not address reinfections or vaccination status at all,
‼️So, AGAIN, even years after a single COVID infection, lungs show irreversible structural scarring that early markers missed, directly tied to real, lasting symptoms(L0ngC0vid)!
#AvoidSars2 #AvoidReinfections
https://t.co/MkhCY5c9LL
@catladyactivist I'm only here to stay informed. I'll miss your posts, unlike some who use X as a sounding board to spew our their bitterness and anger on repeat.
Oh look ! The pesky EU refusing to buy UK food containing pesticides and fungicides which it has banned, but which the UK allows "under its Brexit freedoms"
"Freedom" to use dodgy chemicals, eh ?🤡
and of course that's the EU "punishing" the UK again. Of course it is ...
When it first came out, city folks would use glyphosate to edge driveways, sidewalks , patios, around A/C units and along the foundation of homes. They would pour the herbicide along the perimeter, never worrying about a danger to themselves since told glyphosate was so mild you could drink it. Today, farmers use glyphosate sometimes twice on a field, first time early in the season to rid the field of broad leaf weeds and the second time to dry the crop before harvesting. In America tons of glyphosate are sprayed annually. Imagine the damage to soil & plant eco-systems and to mitochondria in humans. Health is wealth. Know everything in and on your food.
I'm a cardiologist. For months I've been telling you that inflammation is the fire behind heart disease — not just cholesterol. That we've been treating the smoke while the fire kept burning.
Penn Medicine just built the fire extinguisher.
They took the most powerful immune technology in cancer medicine — CAR T-cell therapy — and flipped it. Instead of engineering killer cells to destroy tumors, they engineered regulatory T cells to suppress the chronic arterial inflammation that causes heart attacks.
Published in Circulation. The results stopped me cold.
In CAR T cancer therapy, doctors extract your T cells, genetically engineer them to recognize a specific target, and infuse them back into your body as precision-guided missiles. It has cured previously terminal blood cancers. The technology won its developers a Nobel Prize.
The Penn team asked a question no one had asked before: what if we aimed this at the arteries?
They engineered regulatory T cells — Tregs, the immune cells whose job is to calm inflammation rather than cause it — to specifically target oxidized LDL. OxLDL is the molecule that starts the entire atherosclerotic cascade. It infiltrates your artery wall, triggers macrophages to gorge on it and become foam cells, releases inflammatory cytokines, recruits more immune cells, and builds the plaque that eventually ruptures and causes a heart attack.
OxLDL is the match that lights the fire. These engineered CAR Tregs are designed to find that match and snuff it out — at the arterial wall itself.
The results in mouse models of atherosclerosis:
Blocked macrophage foam cell formation — the cellular process that builds plaque. Dramatically reduced arterial wall inflammation. Prevented over 70% of plaque buildup compared to untreated controls. And critically — preserved normal immune function everywhere else.
That last point is essential. Previous anti-inflammatory approaches to atherosclerosis failed because they suppressed the entire immune system — leaving patients vulnerable to infections and other complications. Colchicine works modestly. Canakinumab in the CANTOS trial reduced events but increased fatal infections. The immune system is a sledgehammer. You can't just turn it down globally.
CAR Tregs solve this by being targeted. They don't suppress your whole immune system. They patrol your arteries specifically, calming the inflammation at the exact site where it's causing damage — and leaving the rest of your immunity intact.
One infusion. Targeted. Precise. The cells do the work.
Lead author Robert Schwab of Penn Medicine put it directly: "If we can get the immune system to see OxLDL and provoke an anti-inflammatory response, it would reduce inflammation and essentially stop the pathogenesis in its tracks."
Senior author Avery Posey: "Our study shows for the first time how CAR T cell technology could be used to treat the underlying cause of the most common form of heart disease — the leading cause of death worldwide."
As a cardiologist who has spent twenty years treating the downstream consequences of arterial inflammation — the stents, the bypasses, the cardiac rehab, the second heart attacks — I need you to understand what this represents.
Every treatment I currently have manages the damage after the fire has burned. Statins lower the fuel supply. Blood pressure meds reduce the mechanical stress. Stents prop open arteries that have already narrowed. These save lives. I use them daily.
But none of them put out the fire itself.
CAR Tregs are engineered to extinguish the inflammation at its source — inside the artery wall — before the plaque builds, before the vessel narrows, before the rupture, before the heart attack.
This is the shift from managing disease to correcting the biological process that causes it. At the cellular level. With living medicine.
This was demonstrated in mice, not humans. The leap from mouse models to human cardiovascular trials is enormous and filled with failures. Manufacturing CAR T cells is currently expensive — roughly $400,000 per treatment in cancer. Scaling this for a disease that affects billions would require a manufacturing revolution. Long-term safety of engineered immune cells patrolling human arteries for years or decades is completely unknown. Human trials are likely years away.
But 70% plaque reduction. With preserved immune function. Targeting the exact inflammatory mechanism I've been writing about for months. Published in Circulation — the flagship journal of the American Heart Association.
The trajectory is unmistakable.
Gene editing to permanently lower cholesterol. Personalized mRNA vaccines to hunt cancer. GLP-1 drugs rewiring metabolism. Cellular reprogramming to reverse aging. And now �� living immune cells engineered to extinguish the inflammation that causes the number one killer on earth.
Every one of these treats the root cause instead of managing the downstream damage. Every one of them was impossible a decade ago. Every one of them is in trials or approaching trials right now.
I've held dying hearts in my hands in the cath lab at 3 AM. Hearts that were destroyed by inflammation I could see but couldn't stop.
The day I can infuse a patient with cells engineered to stop that inflammation before it ever builds the plaque — that's the day cardiology changes forever.
We're not there yet. But the fire extinguisher just passed its first test.
@Daily_Record Aneurysms are on the rise. Covid is a vascular disease. It causes vascular injury and aneurysms. How can public health continue to ignore this?
Global prevalence of post-COVID-19 condition (Long COVID): a systematic review and meta-analysis of observational studies
🚨The “mild COVID-19” myth is dead!
🚨We have a double ongoing Pandemic(C0vid-19/L0ngC0vid)!
➡️Shocking systematic review and meta-analysis UPDATE (27 prevalence estimates, >200,000 participants, up till Febr 2026) to estimate global prevalence of Long COVID.
➡️Overall pooled prevalence: 30.8% (95% CI 26.8–35.0%)
➡️Extreme heterogeneity: prediction interval 14.0–54.8%, indicating high variability across studies.
➡️Key subgroups:
- Hospitalized cohorts: 37.9% (95% CI 29.5–47.1)
- Non-hospitalized/community/mixed: 26.2% (95% CI 22.0–30.9)
- WHO-defined PCC: 22.8% (95% CI 14.3–34.4)
- Broader symptom-based definitions: 39.7% (95% CI 30.5–49.5)
➡️With a sensitivity (cohort-level) analysis yield at ~31.0%, confirms the main results are solid!
➡️Prevalence varied by region, follow-up duration, and ascertainment methods, studies spanned pre- and post-vaccination eras and variant waves.
➡️Conclusion of the paper:
Long COVID/PCC imposes a SUBSTANTIAL post-acute public health burden.
Due to extreme heterogeneity, the pooled estimate is a descriptive summary of diverse evidence rather than a precise global figure.
The authors call for standardized definitions, harmonized surveillance, transparent reporting (including key variables), rehabilitation pathways, and multidisciplinary care.
➡️Evaluation of vaccination/reinfection impact:
The article provides no data, subgroups, or quantitative evaluation of vaccination status, prior infection, reinfection, or hybrid immunity.
These factors are noted in the introduction and discussion as potentially influential sources of heterogeneity but were not constantly reported in the primary studies.
‼️OK, high heterogeneity but still……..nearly one in three people who contract SARS-CoV-2 develop Long COVID, a massive, enduring burden that neither vaccination campaigns nor natural reinfections have meaningfully curtailed according to the best available global evidence.
This is not a minor or rare sequela, and don’t forget …..many are still unaware of their lingering/silently developing “POST-COVID-19” pathology, with reinfections giving an extra push!
We have a widespread chronic public health failure demanding urgent, resource-intensive action beyond infection prevention, that remains a must! DAMM IT…..WAKE UP!
#AvoidSars2 #AvoidReinfections
https://t.co/rh9XZSpTOQ
Everyone is normalizing the vast & serious adverse health affects of
C O V I D
including premature death
just so they don’t have to admit they gave up their health & lives for capitalism.
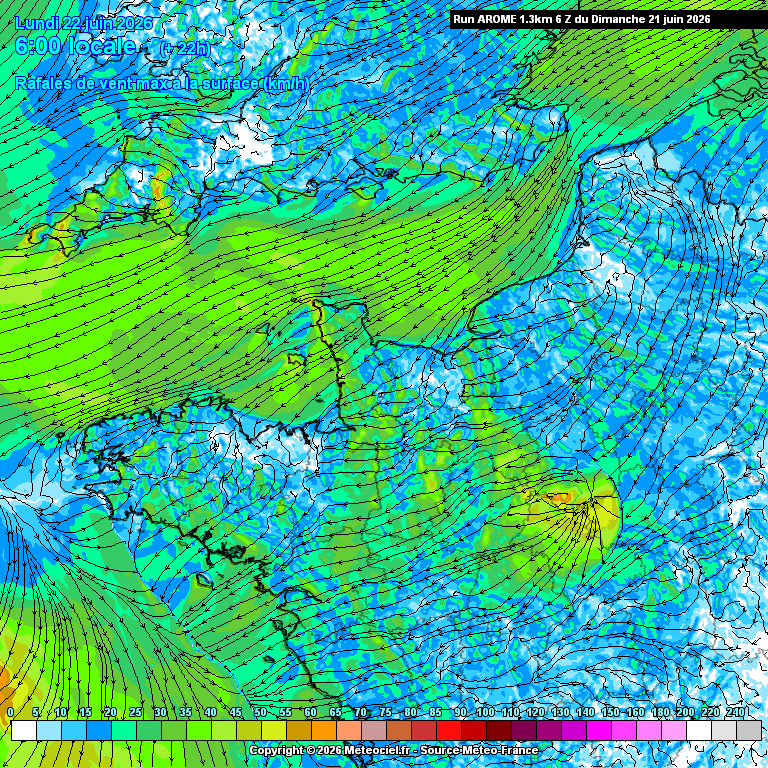
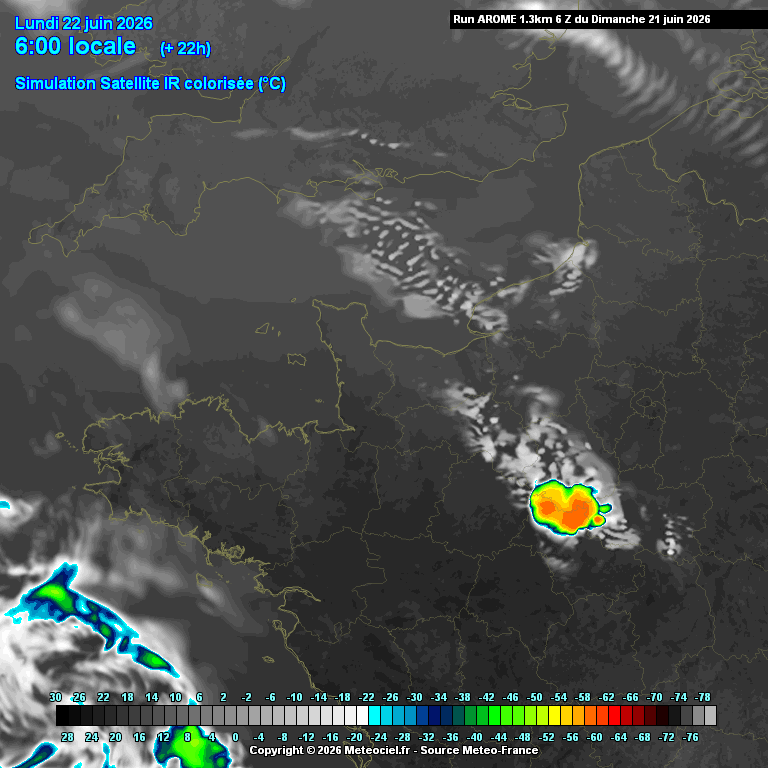
Des heatbursts («bouffées de #chaleur descendante») sont probables la nuit prochaine entre les Pays-de-la-Loire & le Centre VDL.
C'est un phénomène très rare en Europe, où des #orages secs se forment.
Ils peuvent faire passer la température nocturne de ~23°C à + de 35°C en 10min.
Comme si cette #canicule n'était déjà pas suffisamment insupportable et exceptionnelle, ces orages secs peuvent rendre les nuits irrespirables, voire létales pour des personnes sensibles, fragiles, âgées, en bas âge etc.
Lorsque ces orages se forment, la pluie s'évapore avant de tomber au sol mais l'air refroidi qui accompagne les précipitations lui continue sa chute et compresse l'air en surface.
Il peut ainsi être ressenti comme un courant d'air chaud sous le nuage.
Au petit matin, il pourrait faire 33 à 34°C sous ces orages demain, contre 23 à 24°C autour, ce qui est déjà très élevé, pratiquement conforme aux normales de saison d'un après-midi de juin.
According to a top science journal, called Science, vascular (blood vessel) dysfunction is a leading pathway by which #COVID causes neurologic symptoms.
https://t.co/UZeo8nLc9l
1/2
Underrated life advice: Let people be wrong about you. You don't need to correct every opinion. You don't need to win every argument. You don't need everyone to understand your choices. The people who matter will figure it out. The rest were never your real friends anyway.