@normanswan is the best MC for @ACRRM@RuralDoctorsAus#RMA22 - asks all the questions we had ever wanted to ask, has the backs of all rural docs longing for our case to be heard
‘what - do we just imagine the 2nd and 3rd dr we need to allow us workplace flexibility’??
Want to keep your rural health workforce? Value them. Reward them. Listen to their needs & wants. Give meaning & purpose. Don’t exploit their altruism #rma22@acrrm
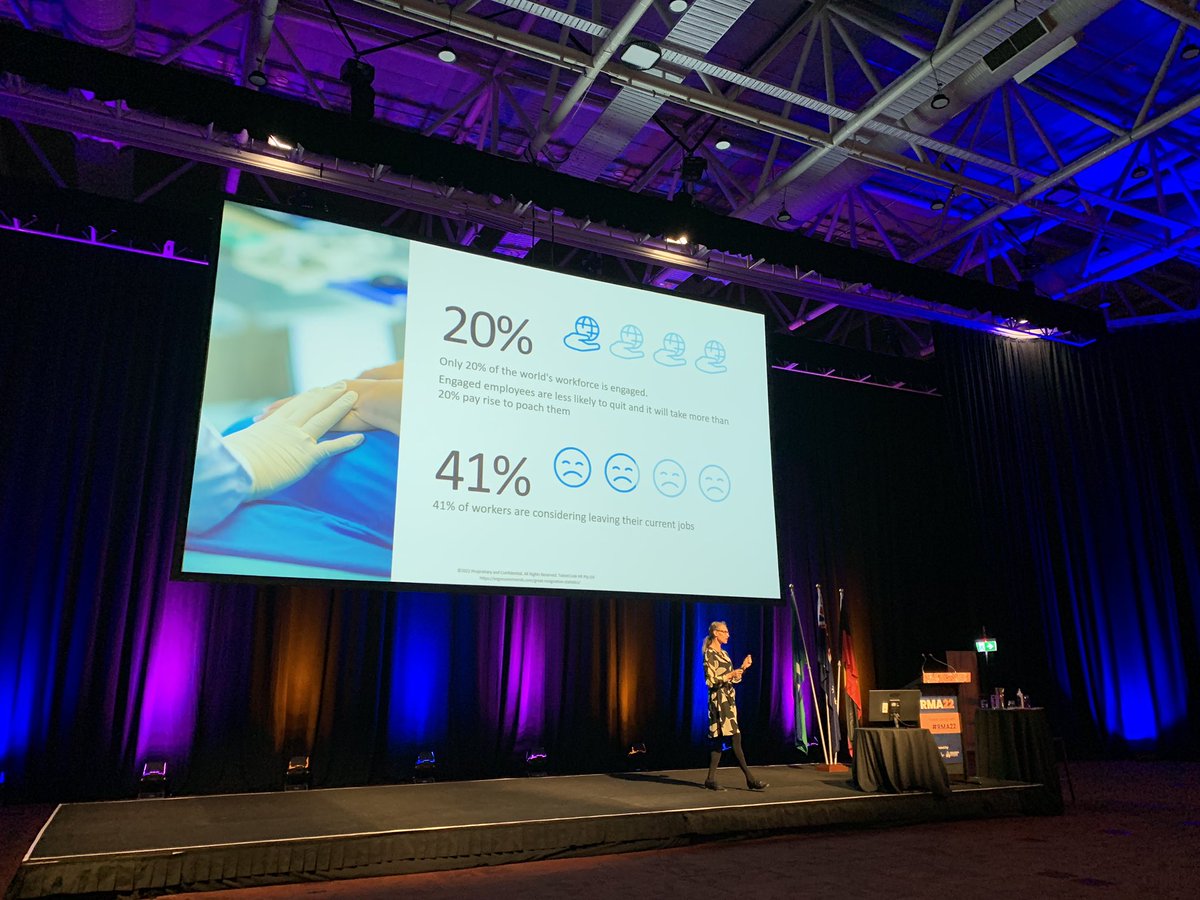
Thankyou to #RMA22 keynote Trudy MacDonald for calling out some of the important factors in employee retention and attrition - sustainability of work expectations being one of them.
Again, clinic expectations. Obstetrics on call is a welcome release from reception expectations.
#RMA22 keynote Trudy MacDonald talks attracting and retaining talent in rural and remote medicine + creating high performance culture and developing leadership capabilities.
@drlouispeachey I have really appreciated seeing people’s faces again. I agree it may be a calculated risk for some. But we miss a lot by not seeing and producing smiles and facial expressions. It’s a big mental wellbeing issue.
And there we finally have it...
Our @RuralDoctorsAus president @BelotMegan acknowledging that Rural General Practice; of seeing patients all day and then being expected to do everything else later, isn't safe or sustainable.
Undifferentiated primary care IS tough. #RMA22
Thankyou @BelotMegan@RuralDoctorsAus for calling out the overwork expected of rural docs.
Why does reception not care about burning docs out? Why ok to complain that a dr wants to ‘stop early’ when they have already seen 50 pts for the day? Why the paperwork late at night?
A non-medical friend recently asked me to describe clinic. I told her to imagine you have 20 meetings in a day, half of them new clients with urgent needs. Each requires your best self. You are late for at least 10 of them. You must prepare a report and deliverables for each one.
I once had a very sick neonate who needed resuscitation. Feeling way out of my depth, I called Dr Dan Halliday @RuralDocDan who appeared almost immediately.
The baby survived. We celebrated passing Neonatal Resus training. Absolutely thrilled to hear he is @ACRRM President!
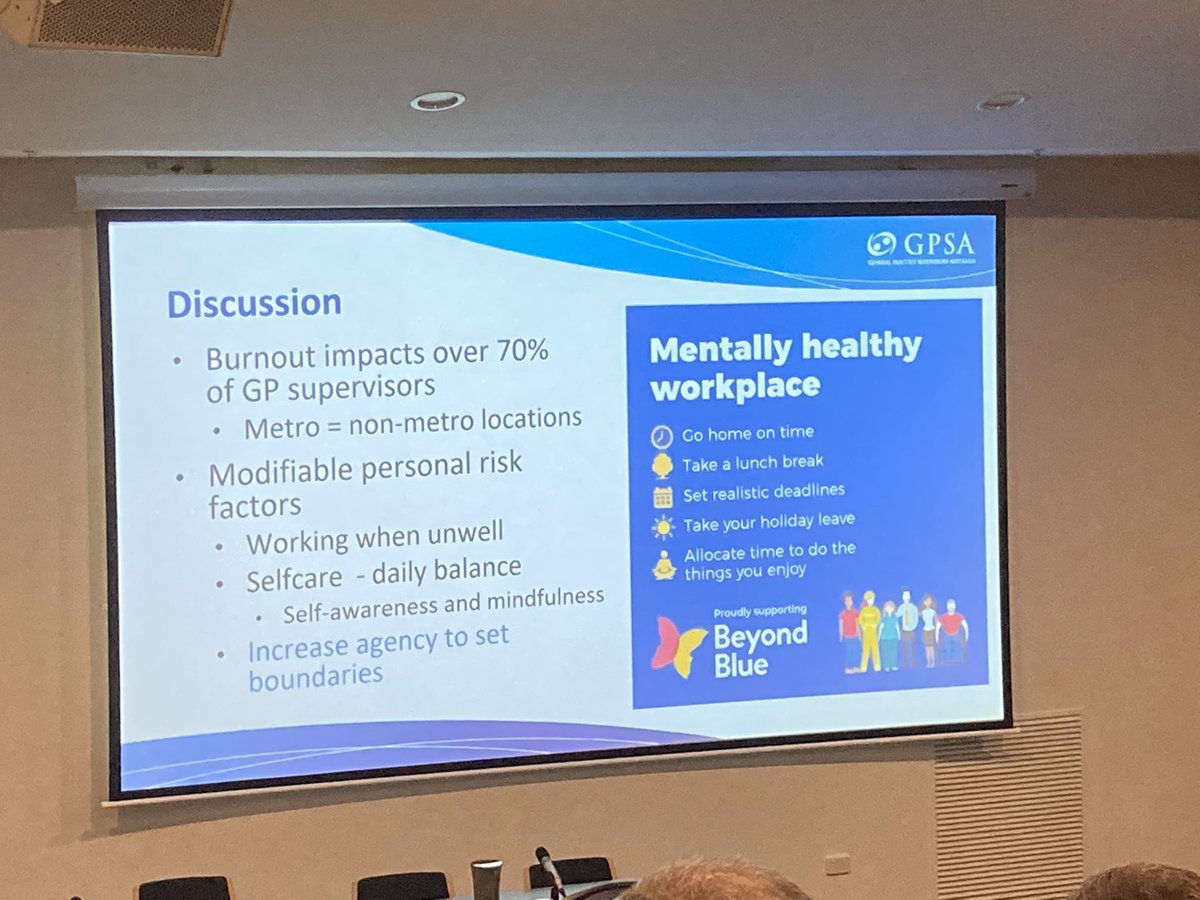
Session at #RMA22 on burnout, re elephant in the room. Hard to meet the suggestions in the blue box when reception praise the docs who see 70+ pts/day, and complain about docs who say no after 50 pts or want to go to Pilates after work or have lunch break as not ‘helping’
@ranzcog@RANZCOG_Pres@JudithGardiner6 Does RANZCOG have a plan for ensuring training provides all of the needed skills to create GPOs comfortable with practicing rurally? How are we going to replace the aging GPO workforce with trainees in many places struggling to convince their supervisors to teach them LUSCS etc?
@brookmanknight I loved the opportunity to do final two years of med school, intern/RMO year, DRANZCOG Adv and ACRRM terms all rurally. I was benefited and not at all disadvantaged.
This.
Without exception, nearly every medical practioner I know has years worth of sick-leave untouched.
If you have time off sick, the weight you carry is distributed between already over-burdened colleagues.
If you can walk, you work
(with the exception of D&V- free pass there)
Medicine relies on doctors working when sick & fatigued. On many shifts I have been more unwell than my patients. There is zero cover provided to replace sick doctors so we turn up & work. This is the culture that your under-resourced health system has created @JennyMikakos