1/11
$CMPS is one of the highest-conviction asymmetric setups in biotech right now. Trading ~$8.4–$9 after the post-EO smashdown. Clean replicated Phase 3 data.
Genuine first-mover classic psychedelic.
Massive political tailwind from Trump EO + CNPV voucher.
Partially built commercial infrastructure that’s highly additive to a strategic buyer. Downside protected. Upside enormous.
$CMPS at Jefferies:
Spravato, despite being on a 2 billion dollar runway, is treating less than 100,000 of those as the only approved pharmacologic product that is being used in treatment resistant depression right now. So we aren't fighting for a finite number of patients. We will be opening up the doors to physicians as well as patients who have otherwise not had any options available to them for treatment resistant depression.
And so Spravato has the, J&J themselves have guided to a 3.5 billion by 2028 and I see no reason why they will not hit that number. Mostly because, again, they're only treating 100,000 out of 4 million patients right now. When we come to market bringing further awareness of the fact that there are now potentially approved products with an indication in TRD, it should be able to continue that growth quite nicely.
But it also should be noted that Spravato is highly burdensome for patients. This is an option that physicians do not offer lightly when they offer it to their patients because it requires quite an intense decision for patients to commit to. And that is twice a week in the first month, once a week for the next month, and then either once a week or every other week thereafter.
These appointments are three hours long and they are required to be driven to and from these appointments by someone else. And so this is heavily burdensome for patients and for caregivers. And so for us coming to market and providing another option at these treatment centers that are well-equipped and well-established to administer these multi-hour in-office treatments, we fully believe that this is going to open up the doors to potentially a lot more patients that are out there that currently aren't able to make a commitment to Spravato.
And Andrew, to your question specifically around why would someone choose Spravato or COMP360, again, we don't see it as a fight against each other. There are plenty of patients who are not being served. Spravato does not work for everyone.
$JNJ Spravato and $CMPS COMP360 are complementary, not competitive in market.
"And Andrew, to your question specifically around why would someone choose Spravato or COMP360, again, we don't see it as a fight against each other. There are plenty of patients who are not being served. Spravato does not work for everyone."
$CMPS at Jefferies:
Spravato, despite being on a 2 billion dollar runway, is treating less than 100,000 of those as the only approved pharmacologic product that is being used in treatment resistant depression right now. So we aren't fighting for a finite number of patients. We will be opening up the doors to physicians as well as patients who have otherwise not had any options available to them for treatment resistant depression.
And so Spravato has the, J&J themselves have guided to a 3.5 billion by 2028 and I see no reason why they will not hit that number. Mostly because, again, they're only treating 100,000 out of 4 million patients right now. When we come to market bringing further awareness of the fact that there are now potentially approved products with an indication in TRD, it should be able to continue that growth quite nicely.
But it also should be noted that Spravato is highly burdensome for patients. This is an option that physicians do not offer lightly when they offer it to their patients because it requires quite an intense decision for patients to commit to. And that is twice a week in the first month, once a week for the next month, and then either once a week or every other week thereafter.
These appointments are three hours long and they are required to be driven to and from these appointments by someone else. And so this is heavily burdensome for patients and for caregivers. And so for us coming to market and providing another option at these treatment centers that are well-equipped and well-established to administer these multi-hour in-office treatments, we fully believe that this is going to open up the doors to potentially a lot more patients that are out there that currently aren't able to make a commitment to Spravato.
And Andrew, to your question specifically around why would someone choose Spravato or COMP360, again, we don't see it as a fight against each other. There are plenty of patients who are not being served. Spravato does not work for everyone.
“Psilocybin, the psychedelic component of magic mushrooms, has previously been touted as an effective treatment for depression, anxiety, addiction, and PTSD — but now researchers say it has the potential to be used in Alzheimer’s intervention as well.
In this case study, published in Frontiers in Neuroscience, researchers focused on an 80-year-old Japanese American woman with Alzheimer’s. She had declined over the previous decade and was reduced to urinary incontinence, speaking in single syllables, and dependence on caregivers for mobility support and daily living.
She was then given a 5g dose of magic mushrooms.
During the initial phase, she was agitated, sweated profusely and entered a prolonged sleep state that suggested unconsciousness. But around hour 19, she began speaking in full autobiographical sentences, recalling life events she had been unable to articulate for years.
In the days and weeks that followed, more incredible changes emerged. She regained urinary continence, even in the evenings, and began dressing herself. She was able to make and maintain eye contact, remember social interactions, emotionally respond to others, and hold lucid conversations.”
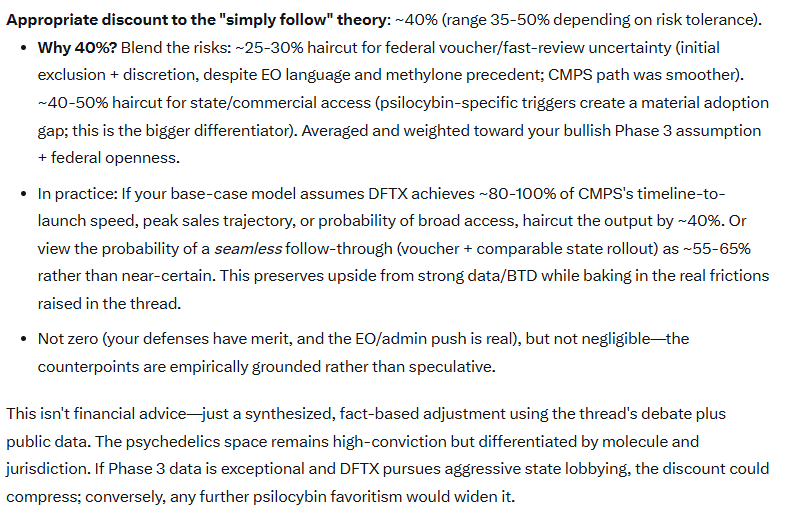
Also, a lot of the state-level momentum over the last few years has been explicitly psilocybin-focused, not "all psychedelics." Some of the trigger bills are literally written around synthetic or pharmaceutical psilocybin receiving FDA approval and DEA rescheduling. South Dakota, Pennsylvania proposals, Arizona's trigger framework, and several other state efforts are tied specifically to psilocybin formulations rather than a broad psychedelic category.
I'm saying that if Trump is getting push back on allowing fasttrack approval of drugs that do not align with the cultural moors of his base, he will kill it. There is a political angle to do with this that has to be considered. He might appease Rogan one minute, but then do an about face another.
$CMPS at Jefferies:
Q: And as I looked the other day on consensus for 2027, I saw $60 million for the entire year. If you priced it at $30,000, I was doing some math, but long story short is maybe you need 3,000 patients to get to 60 million. Would you feel confident you can get 3,000 in 2027?
Lori: I'm afraid to say just how confident I am that it would be hard to believe that that would not be achievable in the first year of launch.
Q: I figured as such. I mean, there are 7,000 centers.
Lori: There are 7,500 centers. We know for a fact that at least 1,000 of them are clamoring, is the best way we probably can describe it, to have this product as an offering for their patients. It seems like an achievable number.