I just want to have a conversation where someone doesn't melt down and utter veiled threats, hurl abuse or sling insults.
I want to have a conversation that doesn't automatically end when the other person runs out of excuses.
Either this bearded male Nazi is actually a woman, or no male is a woman.
Turns out those are your only two options. There is no middle way. Every elected Democrat believes there to be a middle way.
Alas, there is not.
If, as women are always told, there is NO CONFLICT between 'trans rights' and women's rights then Amnesty are wrong to characterise 'gender critical' women's rights groups as 'anti-rights'.
If there IS a conflict between 'trans rights' and women's rights then Amnesty has taken the side of 'trans rights' and is therefore anti-women's rights.
This would make Amnesty itself 'anti-rights'.
Hello all. A quick update from me.
My sex screen assay is progressing well.
I promised rapid: I can detect SRY from a cheek swab in about 30 minutes. I am currently testing whether I can drop it to 10 minutes without compromising reliability.
I promised cheap: The current cost per assay is about £2. I am currently testing whether I can drop this to below the pound line, and it’s very promising.
I promised accessible: The assay could be run by any grassroots sports coach, school nurse, and my Mum.
I promised on-site: This is where my lab efforts are currently focussed. I’ve always held “from the UK to Uganda” as a principle, and ensuring easy deployment is crucial. I’m currently learning a lot of materials science…
The other main push is setting up various blinded, larger-scale tests. This will require lots of form filling.
If anyone wants to help me hit my final budget target, my crowdfunder is here.
I have really had enough of women being told to feel bad about having anything of our own while men's stuff just carries on being men's stuff without the slightest apology or attempt to make male-only environments safer or more inclusive
Trans people are not a historically oppressed group because they are not a group and they have never been oppressed. There is no history of discriminatory state action against them. There are no rights they don't have. Their only grievance is the existence of sex segregated facilities designed for the safety and privacy of women. What the transgender movement calls "rights" are imperious demands to allow anyone who claims to be something they are not to violate sex-based boundaries and coerce others to affirm them as they thing they are not, inherently an assault on the civil rights and liberties of others that masquerades as a civil right belonging to themselves and as a psychic necessity they require for their survival, which in turn serves as a pretext for threatening suicide and committing violence in pursuit of that alleged imperative to survival.
They are a psychiatric diagnosis that was inflated into an astroturfed identity category in the last thirty years by a small cabal of wealthy male sex fetishists who wanted to cross-dress full time and conspired to brainwash a subpopulation of autistic and gender nonconforming children into medically harming themselves with drugs that stopped their maturation, creating an army of hostages that could be used to blackmail the state into coercing the whole world into granting their imperious demands. Along the way, this cabal corrupted medicine and science and law, turning each of these institutions into a font of misinformation in the service of trans activists goals. Literally nothing that issues from these discourses is true, from denials that men have athletic advantages over women to claims that blocking the puberty of children has ever had an evidence base.
Treating any of this like it is real, like it is a civil rights movement, inexorably will result in the infliction of a cascade of absurdities and cruelties on actual vulnerable populations -- woman and children -- above all those confused children who are being brainwashed from the earliest age the falsehood that any of them can change sex.
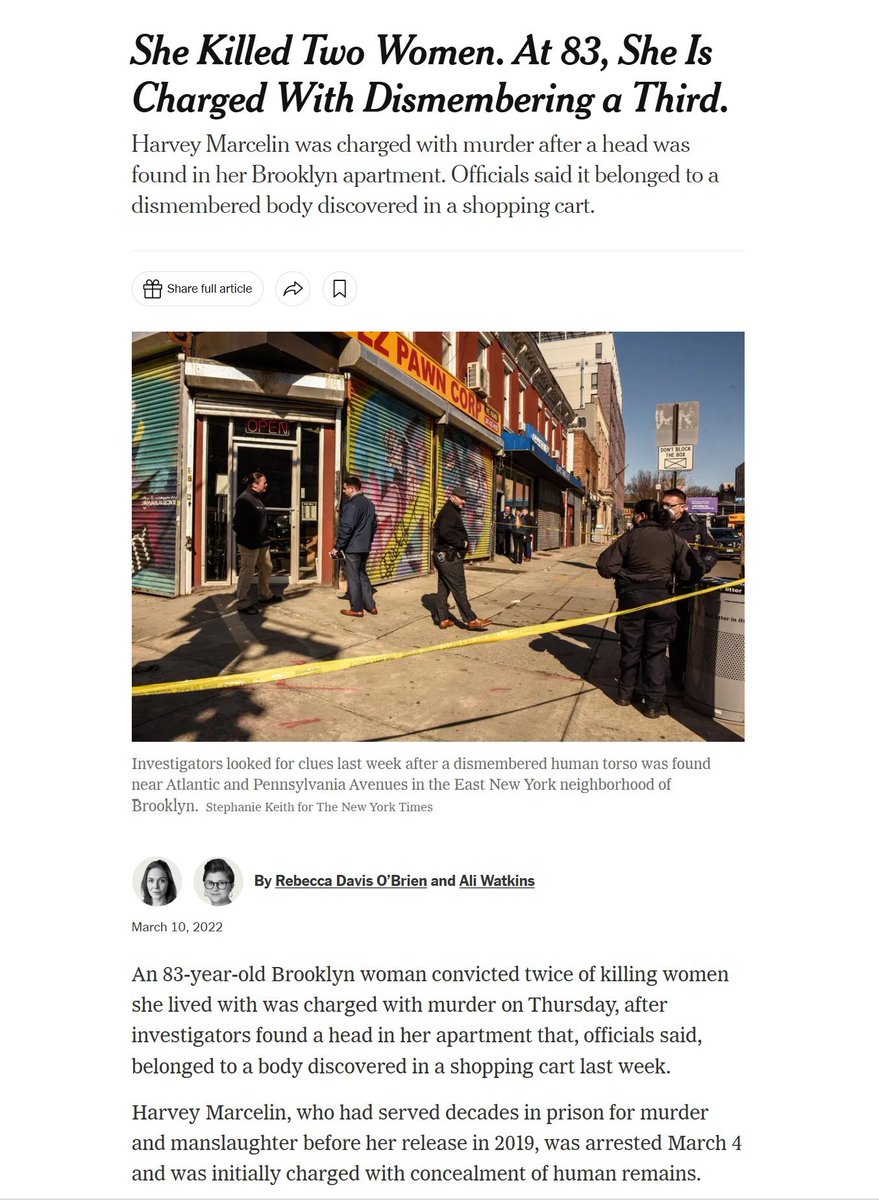
Harvey Marcelin is a male serial murderer of women. He has murdered three women over the course of his life. He is a man.
In 2022, the New York Times honored his gender identity by referring to him as "she" and "her," soon after he was arrested for beheading and dismembering the third woman of the three women he has murdered in his life.
Marcelin no longer calls himself a woman in 2026, so the New York Times now refers to him as "an elderly man."
Marcelin was always a man.
He was a man when he was born.
He was a man when he murdered his girlfriend in 1963. He was a man when he was released from prison in 1984. He was a man when he murdered another woman that lived with him in 1986.
He was a man when he began pretending to be a woman while in prison. He was a man because pretending to be something you are not does not make you into the thing you are pretending to be.
He was a man, and a serial murderer of women, in 2022 when he was granted access to a woman's shelter over the concerns of women who were terrified by the prospect of having to share living quarters with a male serial murderer of women.
He was a man whom an employee of the women's shelter tried to deny access to the shelter.
He was a man for whom the shelter overrode the judgment of that employee and punished her, in order to comply with New York City Human Rights Law, which forbids any woman from drawing a boundary between herself and any man who says that he is a woman, and grants a right to any man who says he is a woman to violate sex-based boundaries.
He was a man who had a "human right" that the state of New York protected to enter private spaces reserved for the protection of women.
He was a man when he beheaded and dismembered yet another woman weeks later.
He was a man when he appeared for trial two days ago acknowledging that he is now a man, a fact that was always true.
He was a man when the New York Times honored his gender identity in 2022 by calling him a woman.
He was a man when he said he was a woman. He was a man when he acknowledged the fact that he is a man.
Nothing's changed. I was being honest about how I feel about an individual trans woman I know, who was a gay man pre-transition, and who I met for the first time post-transition. Objectively speaking, she has physical characteristics that make it fairly obvious she wasn't born female, but she's a gentle, funny person I've never referred to as anything other than 'she' and 'her'. I find it perfectly easy to reconcile my fond feelings towards her, and my experience of her as someone with very female-coded energy, with a belief that she hasn't literally changed sex (and incidentally, she doesn't believe she's literally changed sex, either).
The test we didn't know we were taking
There are moments when a society's institutions are asked to do something difficult. Not difficult in the sense of requiring resources or technical expertise, but difficult in the sense of requiring them to hold a position under social pressure, to say that the evidence is not yet sufficient, that caution is warranted, that the wellbeing of children requires a slower and more careful response than the prevailing mood demands. Those moments reveal something about the institutions that ordinary times conceal.
The response to gender identity claims in children has been one of those moments. And the institutional record, taken as a whole, is not a comfortable one.
What was required was not complicated. It was the ordinary application of the standards that paediatric medicine applies in every other context. Evidence of efficacy before widespread adoption. Assessment of long term outcomes before irreversible intervention. Serious engagement with comorbidities before treating the presenting claim as the primary clinical focus. Safeguarding frameworks robust enough to withstand the pressure of a persuasive and emotionally compelling advocacy movement. These are not high bars. They are the baseline. In this case, across a significant range of institutions and over a significant period of time, they were not met.
Medical royal colleges adopted position statements endorsing the affirmative model without conducting the systematic evidence reviews that would normally precede such endorsements. Professional bodies responsible for the regulation of clinical practice allowed a generation of practitioners to be trained in an approach whose evidence base was, as the Cass Review would later confirm, weak, and whose long term outcomes were unknown. Universities adopted policies, revised guidance, and rewrote safeguarding frameworks in response to advocacy rather than evidence. Schools were asked to implement social transition protocols for children without parental knowledge or consent and largely complied. The press, with honourable exceptions, treated clinical scepticism as a culture war position rather than a legitimate scientific stance for the better part of a decade.
The mechanism was not primarily corruption or bad faith. It was something more insidious and in some ways more troubling. Institutions signalled virtue by their compliance and were rewarded for it. Dissent was reframed not as a clinical or evidential position but as a moral failing, as bigotry, as a refusal to accept the humanity of vulnerable children. The costs of speaking carefully were immediate and social. The costs of not speaking carefully were deferred and clinical, and fell on children who were not in the room when the decisions were made.
This dynamic is not unique to this debate. It is recognisable from other episodes in which institutions abandoned their ordinary epistemic standards under social pressure. What is distinctive here is the specific population that bore the consequences. The children who passed through the Tavistock Gender Identity Development Service during its years of unrestricted operation were among the most psychologically vulnerable children in the country. The Finnish national register data, the most methodologically rigorous evidence available, shows that psychiatric morbidity in gender referred young people rose after clinical intervention. The gap between them and their peers did not narrow. It widened. The institutions that should have been most alert to that risk were among those most captured by the framework that obscured it.
The legal record is part of this picture. Bell v Tavistock in 2020 found that it was highly unlikely a child under sixteen could give informed consent to puberty blockers, a finding that raised immediate and serious questions about what had been happening in practice. The response of the relevant institutions was not a pause for reflection. The Court of Appeal overturned the ruling on procedural grounds the following year and practice continued largely unchanged until the Cass Review forced a reckoning that the institutions themselves had not been willing to initiate.
None of this is an argument that everyone who supported the affirmative model was acting in bad faith. Many were not. Many were responding to what appeared to be a genuine humanitarian imperative, to children in distress, to families seeking help, to a clinical framework that presented itself as settled and evidence based and was endorsed by bodies whose authority they had reason to trust. The failure was not primarily one of individual moral character. It was one of institutional structure, of the mechanisms that are supposed to ensure that advocacy does not substitute for evidence, that social pressure does not override safeguarding, that the interests of children are not subordinated to the reputational interests of the institutions claiming to serve them.
That is a harder failure to face because it implicates systems rather than individuals, and because the systems that failed are the ones that a functioning society depends on to get difficult questions right. Medical regulation, clinical training, academic publishing, legal oversight, press scrutiny, parliamentary accountability. Each of these has a role in the ordinary functioning of epistemic and safeguarding standards. In this case each of them, to varying degrees and with honourable exceptions, did not perform that role adequately.
The Cass Review, the Scandinavian clinical restrictions, the HHS systematic review, and the changing regulatory landscape represent a belated correction. They are welcome. They are also, for the children who went through the system during the years when the correction was most needed, too late to matter.
A moral litmus test is only useful if you read the result. The result here is legible. The question now is whether the institutions that failed it are capable of understanding why, and of building the structural safeguards that would make a comparable failure less likely next time. That work has not yet seriously begun.
A cell layer that has developed to protect your body from the outside doesn’t work like a cell layer that has developed to protect your body from the inside.
The cells lining my vagina are not the same cells, and they don’t have the same function, as the ones wrapping your penis.
There’s a name for what happens when you subject dry-adapted “outside skin” to wet-adapted “inside conditions”.
Further reading: trench foot.