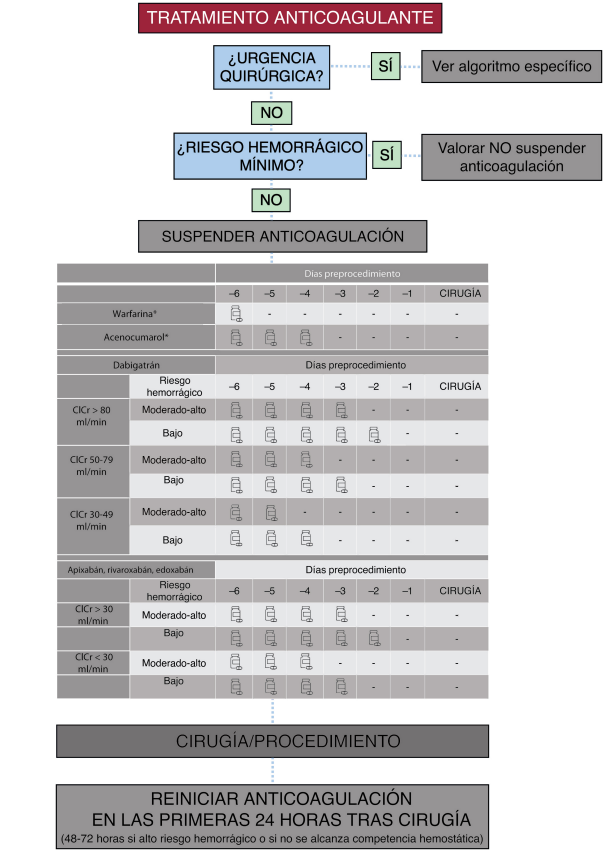
Manejo de Hemorragias en Pacientes Bajo Anticoagulación 🩸💊
🔰📚Acute Cardiovascular Care 2026
https://t.co/9AkjsSS2IK
Enlace a Articulo Completo👇🏻🆓✅
https://t.co/xumUMHaxVK
🫀The failing right ventricle:
the most misunderstood chamber in critical care
For years, we focused on the left ventricle.
But in the ICU, the real killer is often the right ventricle.
->What is acute RV failure?
👉 Not just “weak contraction”
It’s a hemodynamic collapse syndrome:
RV dilation
↓ LV preload
↓ cardiac output
↑ venous congestion
➡️ → multi-organ failure
->The key pathophysiology (the vicious cycle)
1. ↑ Afterload (PE, ARDS, PH)
2. → RV dilation
3. → Septal shift → LV underfilling
4. → ↓ CO → hypotension
5. → ↓ RCA perfusion
6. → RV ischemia
👉 And the cycle accelerates
->The most important concept
👉 The RV does NOT tolerate pressure
Handles preload very well
Fails rapidly with afterload
➡️ Even small ↑ PVR → collapse
->Main causes you MUST think first
🔴 Pulmonary embolism
🔴 RV myocardial infarction
🔴 ARDS / mechanical ventilation
🔴 Decompensated pulmonary hypertension
🔴 Post-cardiac surgery
->Diagnosis is NOT obvious
There is no single sign.
👉 It requires suspicion + integration:
Clinical: congestion + hypoperfusion
ECG + biomarkers
POCUS (your best friend 🤓)
Hemodynamics
->Echo mindset (fast ICU approach)
👉 Don’t overcomplicate
Look for:
✔ RV dilation
✔ Septal shift (D-sign)
✔ TAPSE ↓
✔ Venous congestion
The real ICU mistake
❌ Treating RV failure like LV failure
->Management principles
👉 Think in 4 pillars:
1. Preload — “not too much, not too little”
Hypovolemic → small fluid
Congested → REMOVE fluid
👉 CVP is not a target, it’s a warning
2. Afterload, THE key target
✔ Treat PE
✔ Optimize ventilation
✔ Reduce PVR
👉 If afterload stays high → RV will fail
3. Contractility
Dobutamine
Milrinone
Levosimendan
👉 Choose based on context
4. Perfusion pressure
👉 Norepinephrine is your anchor
✔ Maintains coronary perfusion
✔ Supports RV function
->Ventilation: the silent killer
⚠️ Positive pressure = ↑ PVR
👉 Over-ventilate → worsen RV failure
->When nothing works
👉 Think early:
VA-ECMO
RV assist devices
🤓Key insight
This is NOT just a cardiac problem.
👉 It is a ventriculo–arterial coupling failure
When:
Ees / Ea ↓ → RV collapses
🤓Bottom line
✔ RV failure is preload dependent BUT afterload sensitive
✔ Small mistakes → rapid collapse
✔ Early recognition + physiology-based treatment saves lives
->Clinical mindset
👉 Don’t ask:
“Is the RV failing?”
👉 Ask:
“Why is the RV failing and, what is driving the afterload?”
📃Reference
Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 https://t.co/gri8ZaHHsI
El #HUCA realiza con éxito el primer trasplante de corazón de un donante en asistolia en Asturia.
El receptor ya ha recibido el alta.
Un avance posible por el trabajo de los equipos sanitarios y la generosidad del donante y su familia
#Trasplantes#DonaciónDeÓrganos#Asturias
Meta-analysis of four randomized trials found β-blockers did not reduce mortality, recurrent #MyocardialInfarction (MI), heart failure, or revascularization in patients with preserved left ventricular ejection fraction after MI. https://t.co/KZrArvkwIM
Withdrawal of heart failure therapy after atrial fibrillation rhythm control with ejection fraction normalization: the WITHDRAW-AF trial https://t.co/MyFxT5VxcX
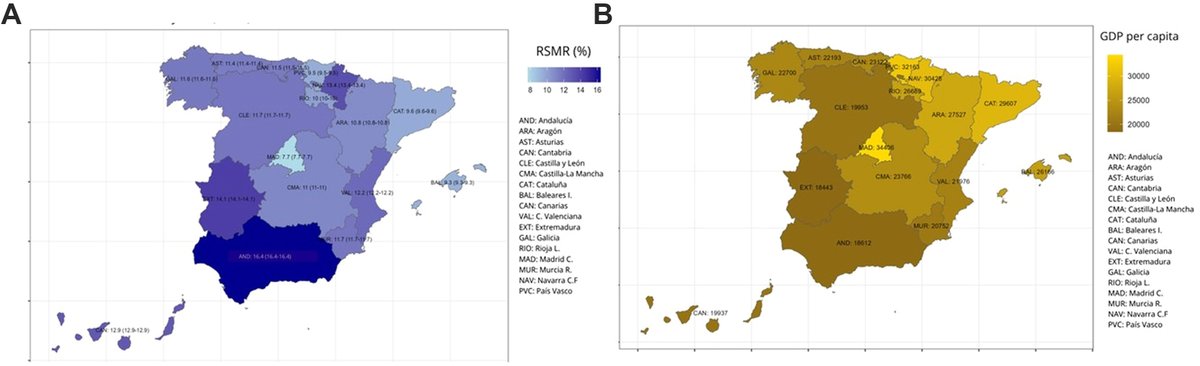
La mortalidad por insuficiencia cardiaca se duplica entre CCAA según su PIB. Este estudio publicado en @TheLancet demuestra que por cada incremento de 1000€ en el PIB per cápita regional, la mortalidad hospitalaria por IC disminuye 0,77 %
🔬IMAS y SEC
🔗https://t.co/c8fdR7G0Tf
🫀🚗 ¿Supone un peligro la #balizaV16 para las personas con marcapasos o DAI?
No. Como otros objetos cotidianos con imán, requiere seguir unas precauciones básicas.
👉 Estas recomendaciones ya figuran en los manuales de las personas portadoras de marcapasos o DAI.
El HUCA reduce un 43% la mortalidad a 30 días tras el alta por insuficiencia cardiaca y la sitúa en el 4,3%
🩺El hospital refuerza la atención integral a esta patología
Más ℹ️👇
https://t.co/zdxvgWlD9u
#MAIC@Boehringer@AntaresConsult@astursalud
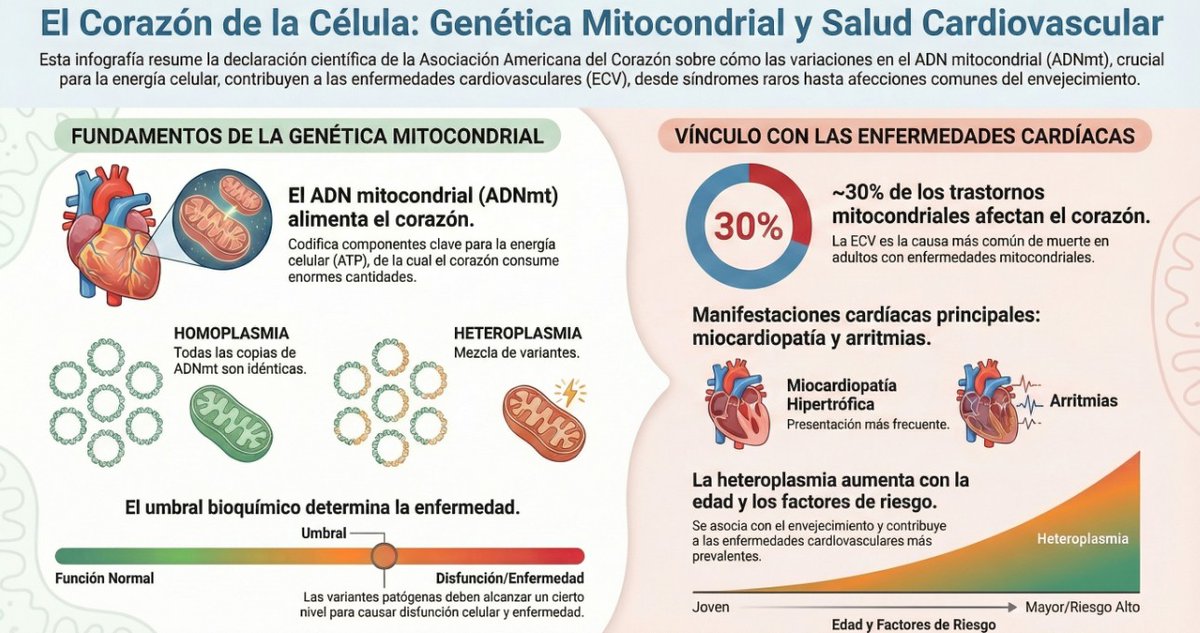
🆕 Cuándo sospechar miocardiopatías o arritmias mitocondriales en consulta: pistas clínicas y estrategia genética.
📕 Circulation
🔓 Resumen del artículo en https://t.co/JkKOl3oFhN
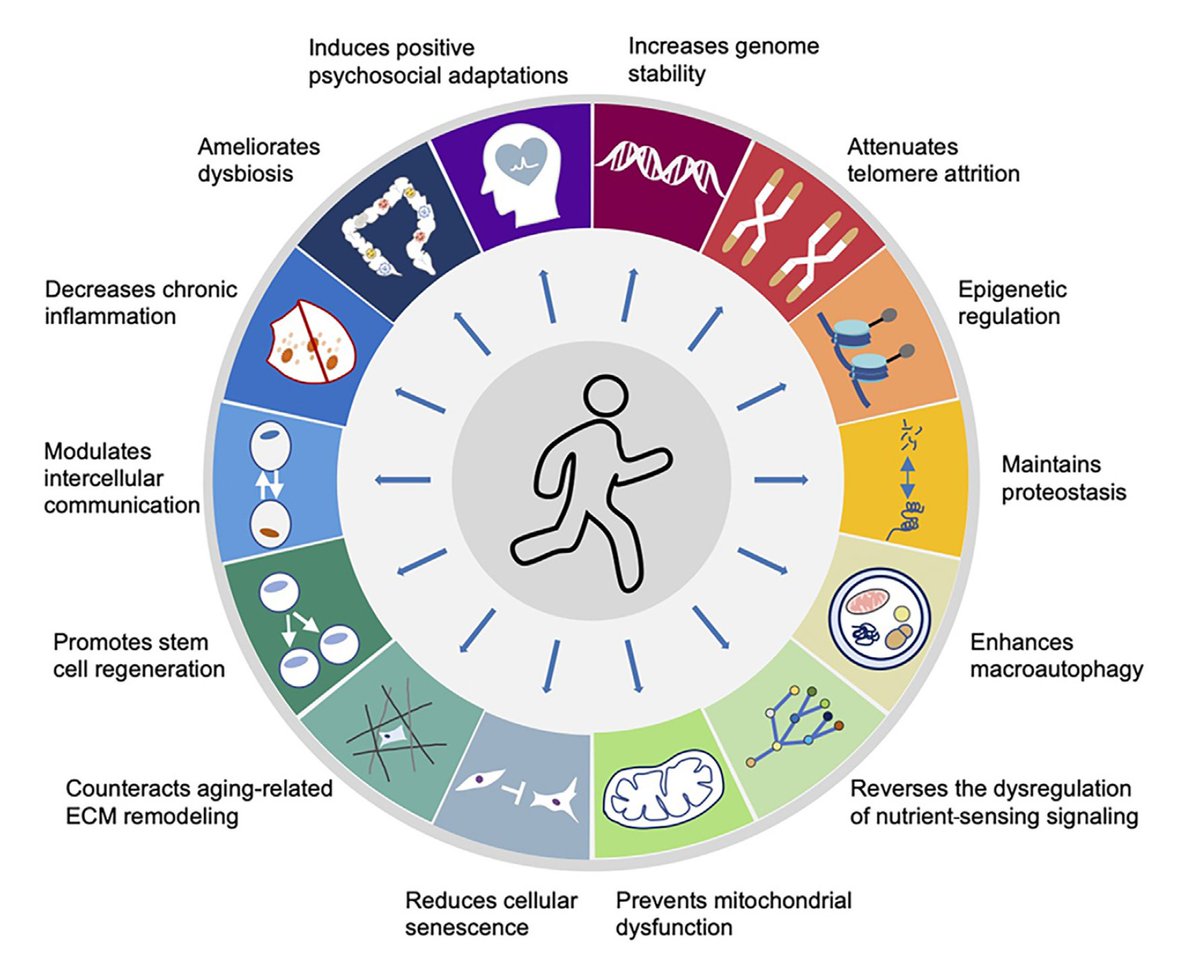
🆕 Ejercicio y envejecimiento cardiovascular: mecanismos y prescripción en mayores - beneficios y dosis óptima.
📕 J Sport Health Sci
🔓 Resumen del artículo en https://t.co/tDOPI75ndY
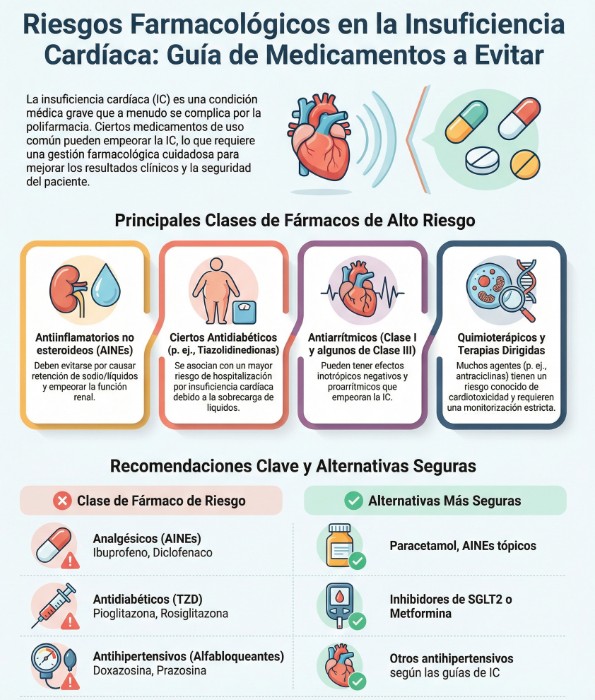
🆕 Fármacos que empeoran la insuficiencia cardíaca: qué evitar y con qué sustituir.
📕 Eur J Heart Fail
🔓 Resumen del artículo en https://t.co/hg0T2frp0r
Muchos fármacos comunes pueden descompensar la insuficiencia cardíaca: AINE/COX-2, tiazolidindionas, verapamilo/diltiazem (en FEVI reducida), clase I y dronedarona.
✅ Alternativas: iSGLT2 y arGLP-1 en diabetes, betabloqueantes + IECA/ARA-II/ARNI y dihidropiridínicos para HTA, amiodarona/betabloqueantes en arritmias. Revisa interacciones y monitoriza función renal y QT.
#Cardio #IC #SeguridadDelPaciente
Imprescindible 👇
Ya está disponible nuestro nuevo documento de consenso sobre cuidados paliativos en la IC avanzada ❤️🩹👏👏.
Un trabajo liderado por la asociación, con la participación y aval de @sociedad_SEHAD y @secpal_.
Consulta el documento aquí:
https://t.co/RknUVmfmK3”
Insuficiencia Cardíaca de FEVI Reducida. Update 2025 @TheLancet 🫀💯
🔵La IC sigue siendo un problema global: afecta a 60-70 millones de personas y continúa siendo una de las principales causas de hospitalización y muerte CV. ☠️🫀💥
🔵IC-FEVI R ➡️ ~50% de todos los casos de IC. Se define por FEVI <40%, con presentación típica de disnea, ortopnea, bendopnea, fatiga y signos de congestión.
🔵Dx: medición de NT-proBNP como primer filtro (alto valor predictivo negativo), confirmar con ecocardiograma.
🔵Tto: diurético para congestión e inicio rápido y juntos de los 4 fármacos que cambian la historia natural de la enfermedad ➡️ ARNi o IECA/ARA2 + B-bloqueador + ARM + iSGLT2. 💊💊💊💊✔️
🔷️Otros tto para pacientes seleccionados: Ivabradina, Veraciguat, hidralazina + ISDN, digoxina, TRC/DAI.⚡️
🔗https://t.co/TnUFdlj2i8
🔗https://t.co/vWK4KBQ4XV