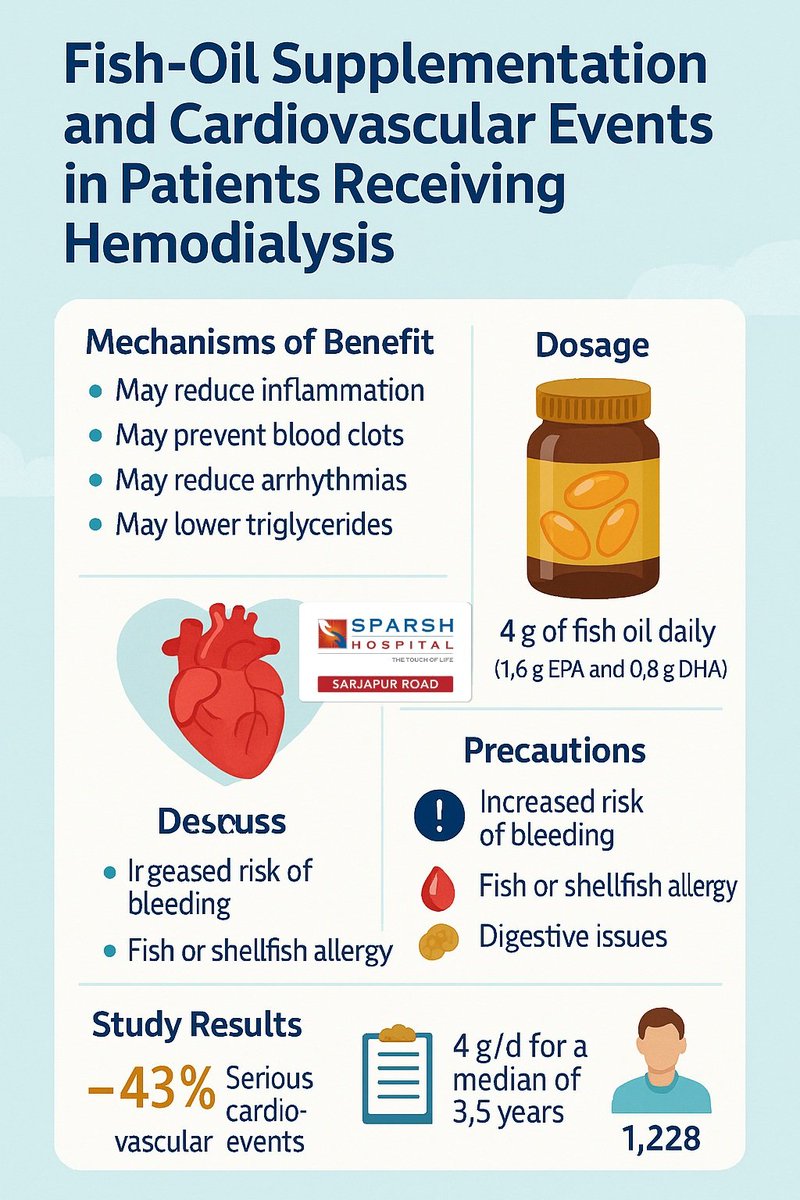
🧵 Fish Oil & Heart Health in Dialysis Patients: A Game-Changer?
1/
A major new study (PISCES trial) shows that daily fish oil supplements can cut serious heart risks by 43% in patients on hemodialysis. That’s huge. Let’s break it down 👇
Kidney Cancer: What Every Adult Should Know 🩺
As a urologist, one of the most important things I tell my patients is this , kidney cancer is often silent in its early stages.
Many people feel completely well right up until it's detected, frequently by chance on a scan done for something unrelated. Awareness is your best protection. Here's what you should understand.
🤔What is kidney cancer?
The kidneys are two bean-shaped organs that filter waste from your blood and produce urine. When cells in the kidney begin to grow uncontrollably, they form a tumour.
The most common type in adults is Renal Cell Carcinoma (RCC), which accounts for roughly 85–90% of cases. It usually develops in people between 50 and 70 years of age and is somewhat more common in men.
Why it's often missed early ⚠️
There are very few nerve endings inside the kidney, so a small tumour rarely causes pain or symptoms. This is why so many kidney cancers today are found incidentally , during an ultrasound or CT scan ordered for abdominal pain, a health check, or another condition entirely.
The good news: when caught small and early, kidney cancer is highly treatable and often curable.
Warning signs to take seriously
While early disease is usually silent, see a doctor promptly if you notice:
🔴 Blood in the urine (visible or detected on a urine test)
🔴 Persistent pain in the side, flank or lower back
🔴 A lump or mass in the abdomen or side
🔴 Unexplained weight loss, fatigue or persistent low-grade fever
🔴 Unexplained anaemia (low haemoglobin)
These symptoms don't always mean cancer , but they always deserve evaluation.
Who is at higher risk?
Obesity and a sedentary lifestyle
High blood pressure
Long-standing chronic kidney disease or dialysis
Family history or certain inherited conditions (e.g., Von Hippel–Lindau syndrome)
Occupational exposure to certain chemicals
The encouraging part 💚
Modern urology has transformed how we treat kidney cancer. Small tumours can often be removed while preserving the healthy part of the kidney (partial nephrectomy), and many surgeries are now done through minimally invasive laparoscopic or robotic techniques , meaning smaller incisions, less pain and faster recovery. For very small tumours in selected patients, active surveillance is even an option.
Advanced cases have benefited enormously from newer targeted therapies and immunotherapy.
Protect your kidneys 🛡️
Maintain a healthy weight, control your blood pressure, stay hydrated, and don't ignore blood in your urine, ever.
If you have any of the warning signs above, or if a scan has incidentally picked up a kidney mass, please don't panic but do consult a urologist for proper evaluation.
Early assessment saves kidneys, and saves lives.
Dr Bivek Kumar
#KidneyCancer #RenalCancer #UrologyAwareness #KidneyHealth #CancerAwareness #EarlyDetection #BloodInUrine #MensHealth #HealthEducation #KidneyCare
Clinical Practice Update
Testosterone Therapy & Prostate Cancer Risk
Morgentaler A, Traish AM.
Testosterone Does Not Drive Prostate Cancer: Presenting the New Framework of Androgen Adequacy vs Inadequacy.
J Urol. 2026.
This update provides an evidence-based distillation of the shifting paradigm surrounding testosterone therapy (TTh) and prostate cancer (PCa).
It is designed to assist clinicians in navigating therapeutic hesitancy, evaluating risk, and counseling hypogonadal men.
1. The Core Paradigm Shift
The traditional "Androgen Hypothesis" (treating testosterone like "gasoline on a fire") has been falsified. Clinical practice is moving toward the Saturation Model and the framework of Androgen Adequacy vs. Inadequacy.
Clinical Pearl: The prostate requires a baseline level of androgens for normal metabolic function. Dropping below the saturation point (via ADT) starves the tissue, causing regression. However, raising T levels above this saturation point does not cause hyper-stimulation or accelerated growth.
2. Critical Trial Data for Risk Counseling
When counseling anxious patients (or navigating regulatory warnings), utilize these landmark data points:
The TRAVERSE Trial (2023): In a massive RCT of 5,204 men over 14,302 person-years, PCa incidence was identical between the TTh and placebo arms (12 vs. 11 cases). High-grade PCa rates were similarly low (5 vs. 3 cases).
The Medicare Cohort Study (2025): A massive observational study of 546,964 hypogonadal men demonstrated that TTh use was associated with a 16% reduction in the hazard of developing PCa.
Biopsy Controls: Data from the REDUCE and PCPT trials confirmed that endogenous serum levels of Total T, Free T, and DHT bear no statistical correlation with baseline PCa risk or cancer grade.
3. Managing Specific Patient Populations
The historical absolute contraindications for TTh are rapidly narrowing. Based on the consolidated data of over two dozen modern trials, consider the following clinical approaches:
Patients on Active Surveillance (AS)
The Data: Multiple case-control and series studies (e.g., Kacker et al., Applewhite et al.) show no increased rate of clinical progression or definitive PSA spikes when hypogonadal men on AS are placed on TTh.
The Reality: Low endogenous serum T is actually an independent predictor of clinical progression for men on active surveillance.
Post-Radical Prostatectomy (RP) or Radiation (XRT)
The Data: Meta-analyses of high-risk populations post-local therapy show a 0% to minimal difference in Biochemical Recurrence (BCR) between TTh users and untreated controls.
The Reality: In several cohorts, TTh was an independent predictor of improved recurrence-free survival, potentially due to T-induced differentiation or antiproliferative dynamics.
4. Expected PSA Kinetics on TTh
When initiating TTh in a hypogonadal man, clinicians must anticipate and correctly interpret changes in PSA:
If Baseline T is < 250 ng/dL: Expect a modest, transient rise in PSA over the first 6 to 12 months.
This represents the benign prostate tissue returning to a state of "androgen adequacy" and upregulating its baseline biosynthetic capability.
If Baseline T is > 250 ng/dL: PSA levels typically remain flat, as the androgen receptors are already saturated.
The "Rule of Thumb": A continuous, steep linear rise in PSA after the first year of therapy warrants standard diagnostic workup (mpMRI/biopsy), as it indicates a new clonal progression independent of the exogenous testosterone.
A super Power like China never goes for a war because it know how much it will impact economically.
Trump now have to re-think on his strategy & grasping for air.
A poor developing nation like Bangladesh coming all out on waging war with India by provoking through Ismalic Radicals. The same country which helped them liberate from Terrorist country Pakistan is now killing Hindus and planning for mass massacres before even securing a vaccine for their Children is a disaster.
Bangladesh was once seen as a fast growing economy is now reduced to dust because of it's Anti India Narratives after ousting the then PM @BdAwamiLeague.
The current Bromance with Terrorist Pakistan is going to drag them down even more because the co-operation is nothing of economic or strategic but rather to create adversaries from all fronts, to counter India.
You can forget anyone you want but not your father.
I Pity the poor who have nothing to do with politics but this is your fate because you chose Yunus over Sheikh Hasina.
Crude oil worth ₹1.32 lakh crore was imported from abroad, out of which fuel worth ₹52,876 crore was exported to other countries 🤔😱
The same people who keep asking citizens to “use less petrol and diesel” never asked the companies to reduce fuel exports instead?
So austerity is only for the public, while exports and profits continue normally? Interesting model.
My lived experience taught me that many Indian women and men above 65 are one of the most regressive, dangerous, fraudulent and corrupt-to-the-core group of humans alive. Their goal is total control over every youngster in their family, and elimination of their desires, life ambitions and happiness, to the maximum possible extent. They absolutely demand respect no matter how repulsive their character(s) may be. And they use culture, religion and mumbo-jumbo to perpetuate their fraud. Time to speak up, and expose, and resist.
Must read: How Hospitals inflate bills in India
1. Doctors get paid for more treatment
The fee-for-service model ties doctor bonuses and salaries to the revenue they generate. So the system rewards extra tests and procedures, even when not needed.
2. Expensive IV drugs over cheaper oral ones
Hospitals push doctors to prescribe stronger, more expensive antibiotics. IV when oral works. Sometimes antibiotics when none are needed at all. All of it done to push up the reimbursement claim from insurers, including government schemes.
3. Unnecessary scans and tests
CT scans, MRIs, PET CTs ordered for minor stuff like simple stomach pain or suspected food poisoning. A basic clinical exam would have done the job. Same with injections for fever, when reports show no infection.
4. Patients profiled for pricing
Hospitals look at how a patient is dressed, what they do for a living, where they're from. Then they decide who can be charged more. Bills get adjusted after admission based on that read.
5. Life support extended even when recovery isn't possible
Terminally ill patients, like those with severe stroke or terminal cancer, kept on ventilators just to extract more billing. Even when doctors know there's no chance of recovery. One of the worst things he spoke about.
6. In-house pharmacy and diagnostics run as profit centres
IPD prices are higher than OPD for the same service. The hospital uses this to recover infrastructure and operational cost. That's why drugs, tests and scans inside the hospital cost way more than outside.
With foreign PE money sitting on top of most big hospitals now, this only gets worse without some regulation or check in place.
The aam junta, as usual, ends up at the receiving end. Either pay big bills to hospitals, or pay big premiums to insurers.
PS. This is also why GIC (an industry body for insurance) is driving common empanelment with hospitals. It's one of the real steps the industry is taking to negotiate better with hospitals, drive standardization, at least for insurance customers. Hope it works.
Source: Raj Shamani podcast with Dr. Reddy, founder of Continental Hospitals.
It’s not the duty of the public to compensate companies for their losses nor is it the public’s duty to provide freebies so the government stays in power. Stop this helpless act and get on with governance.
I am in the opposition and it is my duty to be critical of the government. Now that the most Hon'ble PM shri Narendra Modiji had responded & asked his own convoy to be cut by 50%, it would be unfair on my part if I don't appreciate our PM. Of course a lot, lot, lot more needs to be done: chief amongst which is cutting freebies like Ladki Behn & free lpg but let's appreciate the good.
Jai Hind Jai Bharat! Bharat Mata Ki Jai! VANDE MATARAM!
🚨 Madhya Pradesh Textbook Corporation’s new Chairman arrived in Bhopal from Ujjain with a massive convoy (>500 vehicles) to assume charge.
Meanwhile, the Prime Minister tells citizens and the CM tells ministers: “Save Petrol.” 🤡🤦♂️