Answer: Sotalol can cause QT prolongation due to blockade of hERG potassium channels. This increases the likelihood of R-on-T PVCs, triggering torsades / VF.
The Stitch trial showed a reduction in all cause mortality with CABG in HFrEF, but only at the 10 year follow up. Testing for myocardial viability remains controversial. The recent REVIVED trial failed to show a mortality benefit in HErEF, CAD and evidence of viability.
A 55 year old male is recently diagnosed with HFrEF with an EF of 25%. Coronary angiogram shows triple vessel disease with no significant left main involvement. The patient reports chest pain only when going up hills. Which of the following is true regarding this case?
A 43 y/o man presents with exertional SOB and is found to have an ASD and pulmonary hypertension. #echofirst shows a dilated RV with preserved function. RHC shows mRAP 10mmHg, mPAP 42mmHg, mPAWP 12mmHg, Cardiac output 10 L/min. What is the PVR?
#CardioTwitter
This patient has pre-capillary PH. Autoimmune screen, HRCT and VQ scan are important to rule out a secondary/contributory cause (e.g autoimmune disease, PE, CTEPH). ProBNP is an important risk stratification tool in PH. An MRI brain is not indicated.
A 39 y/o ♀ presents with SOB over the past 6 months. The JVP is up, there is a pansystolic murmur and a loud P2. TTE shows mod TR, dilated and impaired RV and an RVSP of 73mmHg. RHC shows mPAP 39mmHg, mPAWP 8mmHg and PVR 7.8 WU.
Which of the following should NOT be performed?
Pt with HLHS palliated with a Fontan, 18mm extra🫀conduit, has lower limb swelling and loose stools. JVP is +8cm. Liver not palpable. Sa02 89%, Hb 173, plt 196, bili 21, AST 43, ALT 54, GGT 71, ALP 98, albumin 22, INR 1.2. What is the best diagnostic test for this condition?
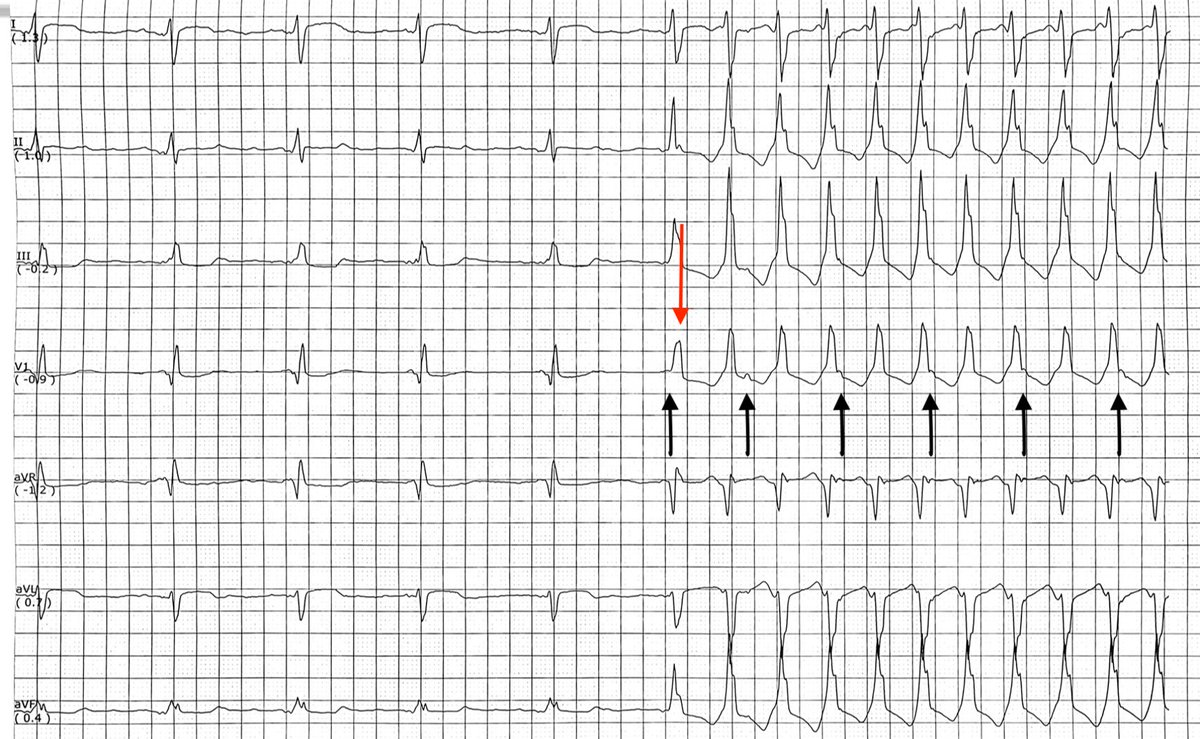
Answer: A - VT
Broad complex tachycardia. The first beat of the tachycardia is likely a fused beat (red arrow). During the tachycardia V>A is noted (P waves highlighted by black arrows), consistent with VT. Biopsy showed 2R rejection.