Rooting for all you #newdocs starting #residency this week!
#Internyear can be stressful.
My best tip comes from @JamesClear:
Aim to be 1% better each day.
Follow up on that patient.
Read a bit each night.
Lock in your system.
After 365 days, you’ll be 37x better.
Pull up for a long thread about this @voxdotcom article with the subtitle "What the fight between @AnthemBCBS and anesthesiologists was really about." 1/12 🧵 @anesthesianews https://t.co/oO7rkW7YRg
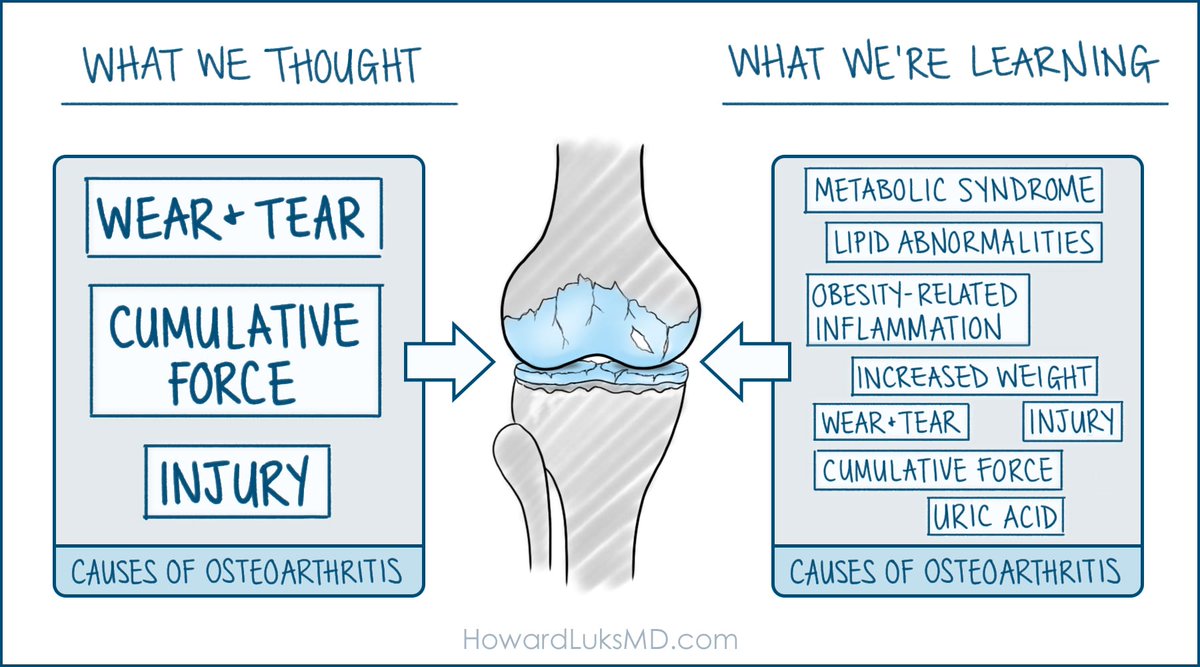
Osteoarthritis is poorly understood... and often managed even more poorly.
Osteoarthritis is the gradual loss of cartilage or cushioning on the ends of our bones. The cartilage cushions the forces of weight bearing and provides a near frictionless interface between the bones of our joints.
Inflammation often follows the loss of cartilage. Knees with more inflammation and swelling have more pain than dry knees.
Cartilage breakdown can begin for many reasons. Contrary to popular thought, cartilage does have complex repair mechanisms in place. But genetics, prior trauma, or surgery can upset those processes. When these processes go awry, cartilage loss can result.
The severity of the arthritis is based on how it impacts your life--- not necessarily by the appearance of your X-ray. I know people who run on bone-on-bone arthritis... yet I know others who are crippled by far more mild osteoarthritis.
Therefore, I usually do not allow the X-ray's appearance alone to define the severity. Why? Because remaining active with an arthritic joint will often enable you to keep that joint longer than someone who is far more sedentary.
This is the reason why telling people to stop moving, stop exercising, or even stop running after they're diagnosed with osteoarthritis is poor advice.
Our overall health and well-being also affect the onset and progression of osteoarthritis. People with big bellies, type 2 diabetes, pre-diabetes, fatty liver, and so on have a high degree of systemic inflammation. Osteoarthritis is more common in this group; it is typically associated with more swelling and pain, and it will progress faster.
Those inflammatory mediators make their way into our joint fluid. A complex series of interactions with macrophages and other cells in our joints can initiate or accelerate the arthritic process and increase the amount of inflammation (and pain) in our joints.
Our joints are not as fragile as you might think. Even after they've become arthritic, our joints will treat us better if we treat our whole body better and maintain our mobility and strength.
A recent paper on GLP-1 medications in the management of people with obesity and osteoarthritis shows that pain scores drop significantly over time and that improvement is sustained. Interestingly, the pain can improve before the dramatic weight loss. GLP1 medications are well known for their ability to "fix" metabolic dysfunction and improve metabolic health.
There's still much more to learn about osteoarthritis. But one thing is sure: the healthier and more active you are with your arthritic joint, the longer you are likely to keep that natural joint.
Genetics should have been listed in the graphic... my bad.
@BStulberg FWIW: here’s the study on the UPF; she could have added more context.
https://t.co/TutofU09dQ
“A higher consumption of UPF (>4 servings daily) was independently associated with a 62% relatively increased hazard for ACM. For each additional serving of UPF, ACM increased by 18%”
Orthopedic Truths:
Tennis Elbow
Stupid name
Most people who have it don't play tennis.
Nearly every person will get it.
The most common cause of lateral elbow/upper forearm pain.
It will resolve almost everyone on its own.
Without "treatment".
But it might take 6-12 months.
Yep, 6-12 months.
It may not resolve in some people.
Some people have minimal symptoms.
Some have severe pain.
Some people deal with pain well.
Some don't.
Most people are in our office because they're afraid of hurting themselves or they have a fear of the unknown.
If you tell them the proper story about tennis elbow, most are relieved and will go on to live their active lives without needing anything.
The pain when lifting with your palm facing down is real.
It also will amaze you how often the outside of your elbow contacts doors, etc.
Lift with your palm up... no pain.
The examination is straightforward.
The diagnosis is straightforward.
MRI imaging isn't needed.
It always says, "partial thickness tears.... yada, yada, yada...."
MRI findings are rarely a reason to have surgery.
Basically... there's very little reason to operate on these at all.
Besides... there are plenty of surgeries described to manage this... most involve releasing/removing the offending tendon-- the ECRB... so why would a tear need to be "fixed" 😂
It can be super annoying... I'll agree to that.
It's worse in people who lift a lot for work.
Some people might insist that something be done.
That's fine...
But far, far, far too many are offered injections as a first-line treatment.
Steroid injections are not kind to tendons.
They're not kind to the lateral ligaments, either.
If not appropriately placed, steroids dissolve the fat under your skin.
That pale dimple with veins running through it is unsightly.
Tendons really don't like steroid injections.
A steroid injection might feel great for a few weeks or months... but the pain often returns.
Not in everyone, though.
So... it might have worked for you.
But it made many others worse.
PRP injections, anyone??
Maybe
It won't cause harm.
You should never pay > $500-1000.
It could work...
Then again...
so do placebos
I'm not calling PRP injections placebos...
But, you know, maybe???
Physical therapy?
Meh...
But anything that distracts you while nature runs its course is valuable.
Braces?
Meh...
That damn placebo effect again
Try it... no harm, no foul.
Red light, laser, blue/purple pulsed lights... whatever.
Shockwave therapy... maybe.
Hard to find... and it hurts... but it might help.
This very common yet annoying ailment is so prevalent.
Most everyone is going to get it.
Carry on...
No need to rest or stop activities unless the pain is too spicy.
Everyone on IG has a cure: save your money, and if you can move on, wait it out.
As usual... it's always far more complex than most people think.
@DrTimothyTiu Love when the peer to peer is due by 5pm today and you call them 6 times with no response and then they send over the denial at 3:30pm with 1.5 hrs to spare
@AyooshPareekMD@jxnlco Agree with @AyooshPareekMD. I’m hopeful you saw a clinician to help to rule out carpal tunnel, ulnar neuropathy, and other potential progressive neurologic conditions. These things can be insidious and don’t always show up on routine tests!
@ChrisCampMD @AJSM_SportsMed @JacobOeding@AyooshPareekMD@bennwachukwumd@DrKrych @mayoclinicsport @MayoOrthoRes@MayoOrtho@aossm1972 Very important work for our field and optimistic it will become more accessible for our patients with contributions to the literature like this.
Still have much work to do re:
1) optimizing/standardizing PRP formulation/dose
2) understanding nuances of non- vs responders
Grateful to learn from Singapore’s sports medicine guru Dr. Mandy Zhang this past month.
Got a fresh perspective on #sportsmed, #shockwave and #orthobiologics and gained a new colleague in the field!
@FitFounder Great info! I point all my patients with back pain to the McGill Big 3.
Many will ask how to stay active despite the back pain and I recommend cycling, swimming, and other low impact exercises. Yoga, tai chi as well for balance and flexibility.
I had a Vietnamese patient in clinic a month ago. We shared stories common to our heritage.
Today she came back for follow-up, with an awesome surprise.
A whole batch of homemade eggrolls. 😵
She said she was so grateful to have a doctor who is Vietnamese. 🙏
Made my day!
Congrats future docs on #MatchDay2024!
As you prep for the next chapter, reflect on:
Who helped get you here?
What principles led you along the way?
When did you feel most alive?
Where do you see your mission field?
But most importantly: start with WHY.
Let this guide you!