Our paper is out: By analysing health records from millions of real-world patients from the literature, we can now finally answer the questions about the long-term outcomes of ECT. What we found, consistently, across well-designed studies from the UK, Canada, US, Sweden, Denmark, and Taiwan, is that ECT does not increase the risk for dementia, heart attacks or stroke, and is associated with a significant reduction in overall mortality.
https://t.co/lC13i5ANBD
The draft GMC Order 2026 consultation just dropped. Buried in it is a fundamental change to who can be awarded a Certificate of Completion of Training (CCT).
This matters enormously. Let me explain why.
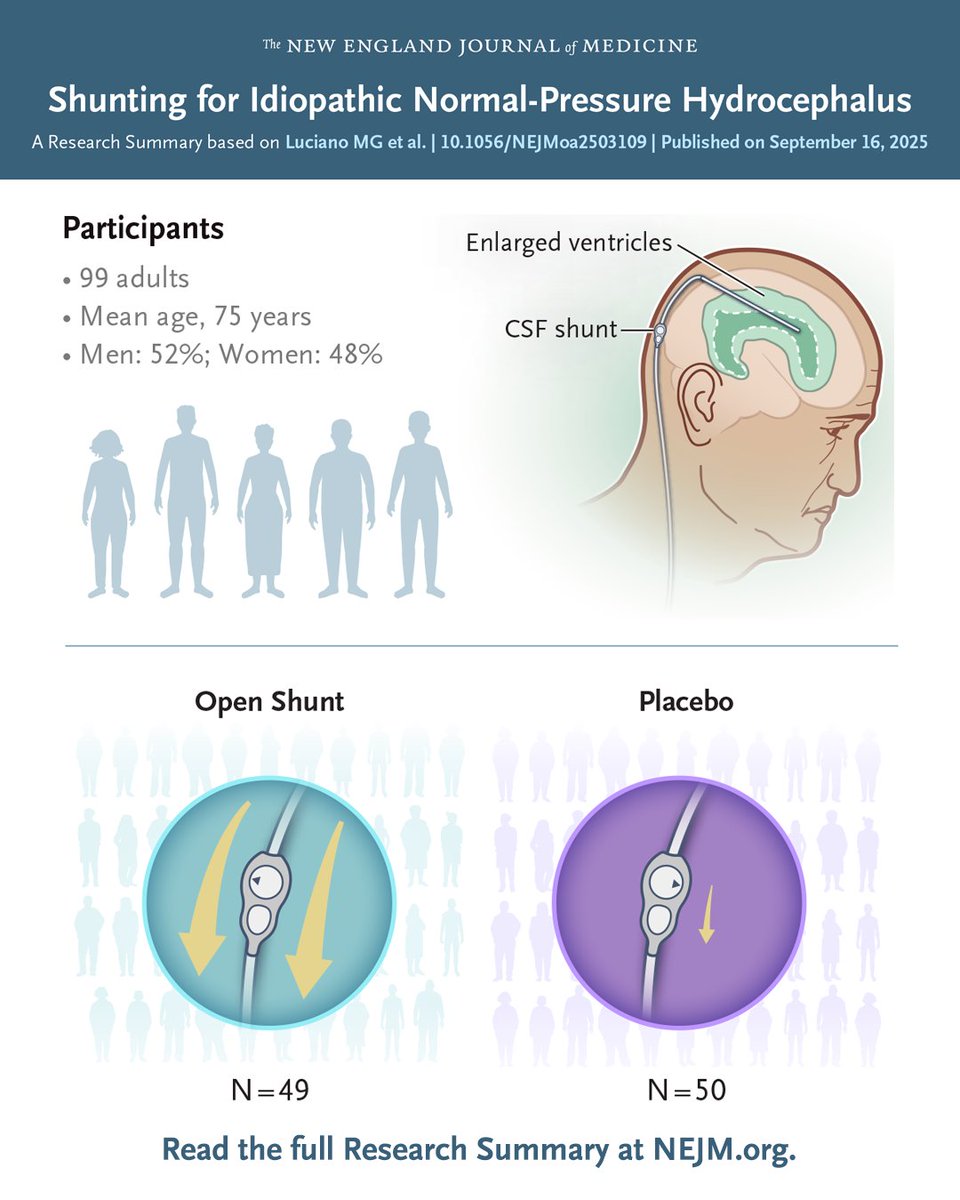
In patients with idiopathic normal-pressure hydrocephalus responsive to CSF drainage, shunting improved gait and balance at 3 months, but not cognition or incontinence, and was associated with some procedure-related risks. Full PENS trial results and Research Summary: https://t.co/vEG6BOTvaO
A fantastic comprehensive review article w/ everything you need to know about Idiopathic Normal-Pressure Hydrocephalus just dropped in the NEJM. Hydrocephalus refers to a condition where cerebrospinal fluid accumulates excessively in the brain’s ventricles, resulting in enlarged chambers that contribute to disrupting walking, cognition and bladder control. Johnson and Williams describe in their new New England Journal of Medicine paper that idiopathic normal-pressure hydrocephalus is a common, frequently missed and potentially reversible neurologic condition in older adults.
Key Points:
-Idiopathic normal-pressure hydrocephalus presents w/ a triad of gait and balance changes, urinary urgency and cognitive slowing, however each feature has an extensive differential diagnosis on its own.
- Prognostic testing w/ cerebrospinal fluid drainage or infusion methods improves selection of candidates who are likely to benefit from shunt surgery.
- Programmable cerebrospinal fluid shunt systems remain the most effective treatment and can improve gait quality of life and survival when used in appropriately selected folks.
My take: Nailing the diagnosis is so important in iNPH, and it is frequently a tricky endeavor for even an experienced clinician. One thing I would add to this article is that a fair number of folks with 'big ventricles' actually have Parkinson's disease, so don't forget considering the possibility of a levodopa trial in select persons who present for shunting. Here are 5 points that resonated w/ me: 1- Recognizing the gait pattern is essential because a wide-based slow shuffling walk frequently precedes memory or bladder issues and can be the earliest clue. 2- Imaging matters ,however it is not enough since enlarged ventricles alone do not confirm the diagnosis and this finding needs to be paired w/ symptoms and w/ testing. 3- A large-volume lumbar puncture can help by temporarily improving walking, which usually signals a higher likelihood of responding to a shunt. 4- Shunt surgery can meaningfully improve daily function, especially the gait and fall risk. Importantly, it should be performed at experienced centers using adjustable valves. 5- Delays in diagnosis can worsen outcomes because waiting too long may reduce the chance of symptom improvement and increase long-term disability.
https://t.co/ns7T6p5WUC @NEJM@movedisorder@FixelInstitute@UF@SfNtweets@ParkinsonDotOrg@PdAvengers@DBSThinkTank
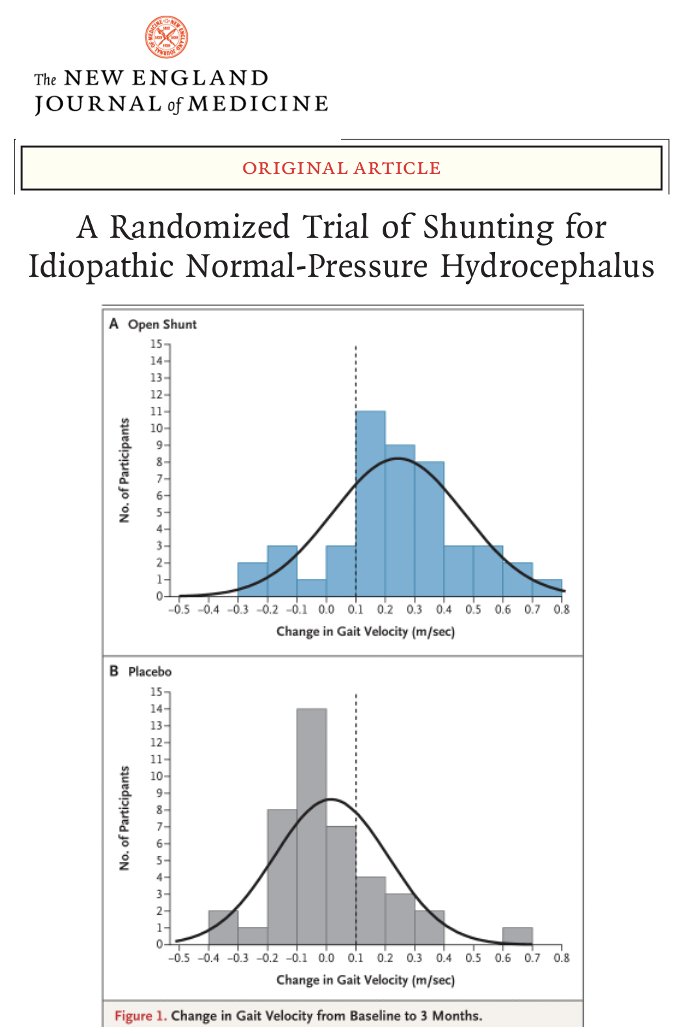
To shunt or not to shunt, that is the (NPH) question? The first large randomized trial of shunting for normal pressure hydrocephalus (NPH) just dropped in NEJM, and there was clear benefit for walking, and it favored the group receiving shunts. Spoiler alert: Walking improved, however thinking (cognition) and bladder function did not.
Key Points:
- NPH is a condition usually presenting in older adults where fluid builds up in the brain and it associated w/ trouble walking, memory and thinking challenges as well as bladder incontinence.
- Shunting significantly improved walking speed and balance compared w/ placebo.
- No meaningful change in cognition or bladder control observed at 3 months.
- Risks included subdural bleeding and headaches, underscoring the need for careful follow up.
My take: NPH has always been a tricky area for clinicians when trying to decidr 'to shunt or not to shunt.' Here are 5 points that resonated w/ me: 1- Shunting in well selected persons can restore some walking ability in NPH. 2- Thinking did not improve at 3 months. 3- Incontinence showed no clear benefit. 4- Risks to always discuss w/ people considering shunts should include bleeding and headaches (as not uncommon). 5- Walking gains may possibly reduce falls and boost independence, however we must be careful as sometimes improved walking w/o improved balance, can actually trigger falls.
https://t.co/yCnSCpclPL @FixelInstitute@ParkinsonDotOrg@alzassociation@SfNtweets@SfNtweets@NEJM
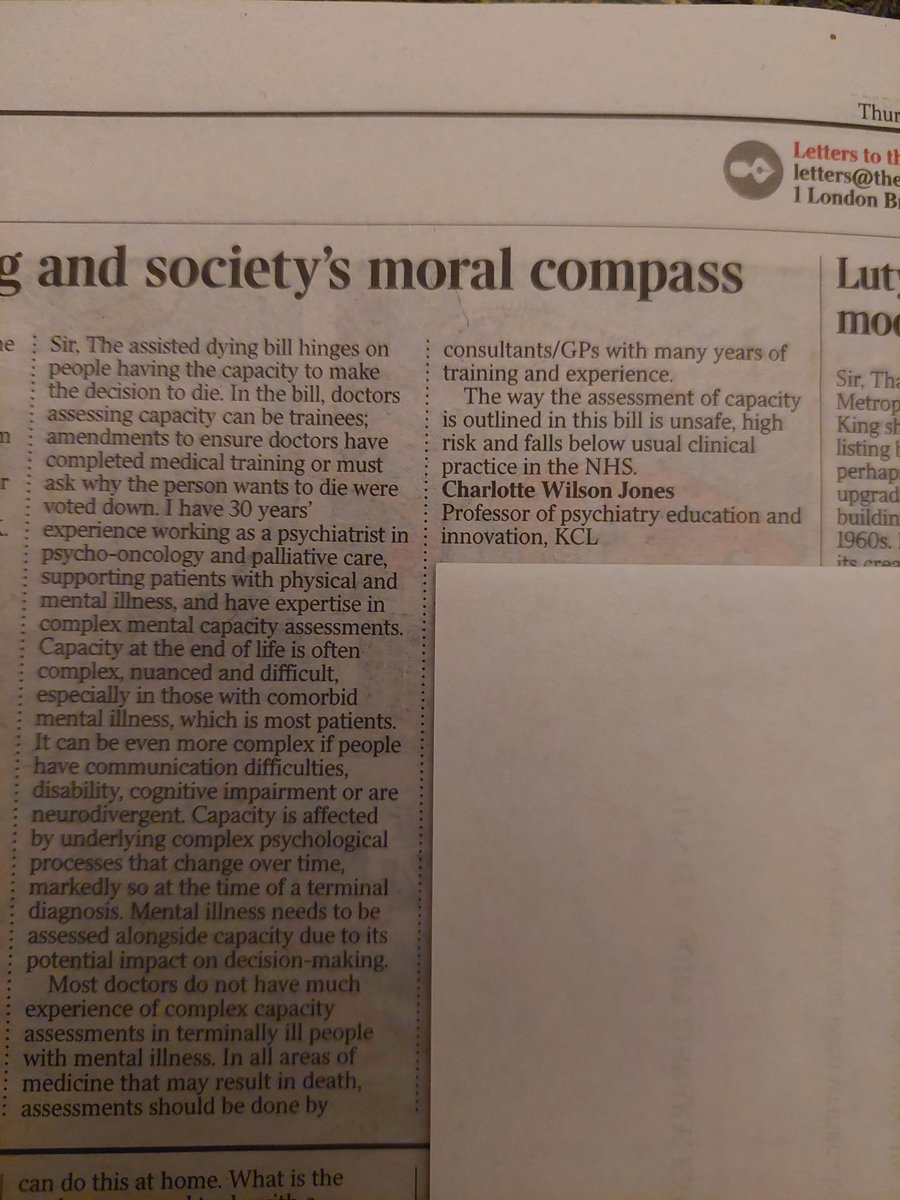
My letter in The Times today. Having capacity is key to #Assisted Dying bill. Capacity safety amendments were voted down. Capacity can be complex & difficult even with years' of experience.
Medicine and #psychiatry in this country changed significantly today.
Let’s hope this shift doesn’t come at the cost of quality #palliative care, or lead to premature, unnecessary deaths among the vulnerable, poor, and mentally ill.
Time for the Lords to earn its keep…
Pleased to have written this blog with @drclarabel - Women are consistently at higher risk of dementia. Increased health equity for women could reduce dementia cases, especially in low and middle income countries where higher dementia risk in women was strongest. Have a read!
Sex differences in dementia risk and risk factors.
New international study suggests:
- dementia risk was higher in women than men
- greater risk in women was most pronounced in LMICs
https://t.co/bLDWCuJ4M9
Always lovely to have babies at our conferences! We ensure there’s private rooms to feed / pump/ nap etc Here’s a little 3 month old enjoying the #arukclinicalconf#workingmum#womenindementia
Great to talk to NYTimes on dementia risk reduction. Even better US CDC is acting on it. Proud of the work of our colleagues @UCLPsychiatry and worldwide on @TheLancet dementia commission. Dementia Prevention Method May Be Behavioral, Not Prescribed https://t.co/SusEZwMQno