Cardiologist, Essex Cardiothoracic centre, Professor of Cardiology ARU School of medicine. Passionate about improving cardiac arrest care, & coronary physiology
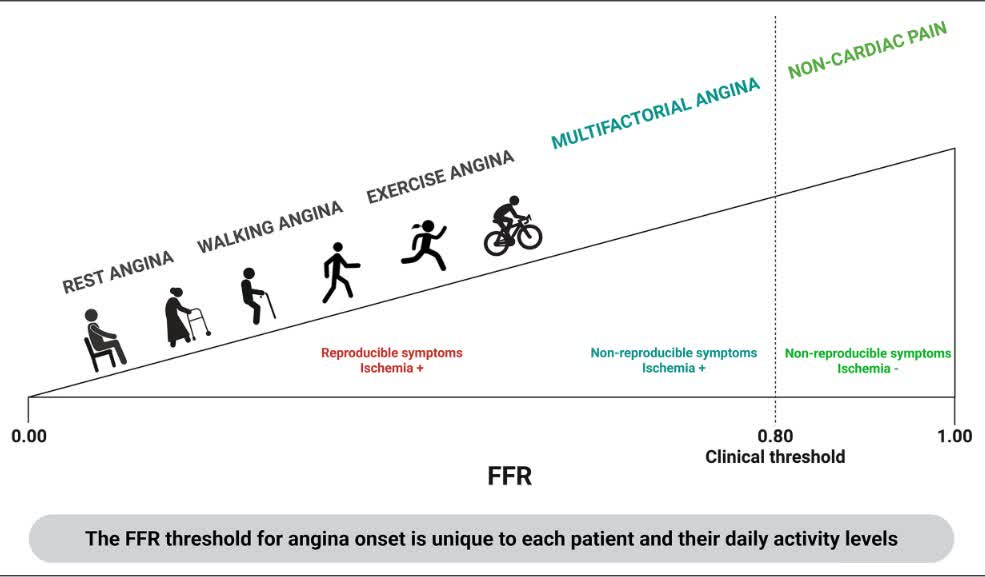
ORBITA-FIRE suggests universal Ischemia-based thresholds for FFR and non-hyperemic pressure ratio should be interpreted with caution: Integrating symptom-linked physiology may refine PCI selection and improve symptomatic response.https://t.co/oGyHMRbOLZ
This should be quite helpful for those few cases when we have to do pci when the cardiac arrest patient is on a mechanic chest compression device… which angles give a view of the coronaries?
Breaking 🚨: Essex Cardiothoracic Centre have randomised their first participant - bringing the study total to 96! 🎉 Great teamwork 🥳🥳 #BCIS4#ClinicalTrials@MSEHospitals
TPC (The Physiology Course) for the first time at EuroPCR
🫀 Following the renowned applied coronary physiology courses at the ESC Heart House in Sophia Antipolis, TPC has become the reference in applied coronary physiology
🚀 For the first time, TPC arrives at EuroPCR.
@ACSCardiology@AnasNomanMD Penumbra are a massive company worth billions. They dont want to do trials as they are selling devices and proper trial data is only a risk to them.
@stefano_garzon@JACCJournals Superb overview. Thank you. IMR is the most validated tool we currently have, until continuous MRR is validated in as many patients. It is all coming and at least we have a more reproducible "gold standard" to act as a comparator.
🧵 ORBITA-CTO
Seeing a study like ORBITA-CTO being published — regardless of its results — is a beautiful thing.
This level of commitment to producing high-quality, as-unbiased-as-possible evidence in interventional cardiology should be praised. It took 4 years to randomize 50 patients. That's dedication.
Think about what this team had to do:
Noise-cancelling headphones, deep sedation, clocks removed from every room, scripted handovers, overnight admission for both arms, dual-operator procedures lasting 3+ hours — all to protect the blinding.
Bang blinding index ≈ 0. It worked.
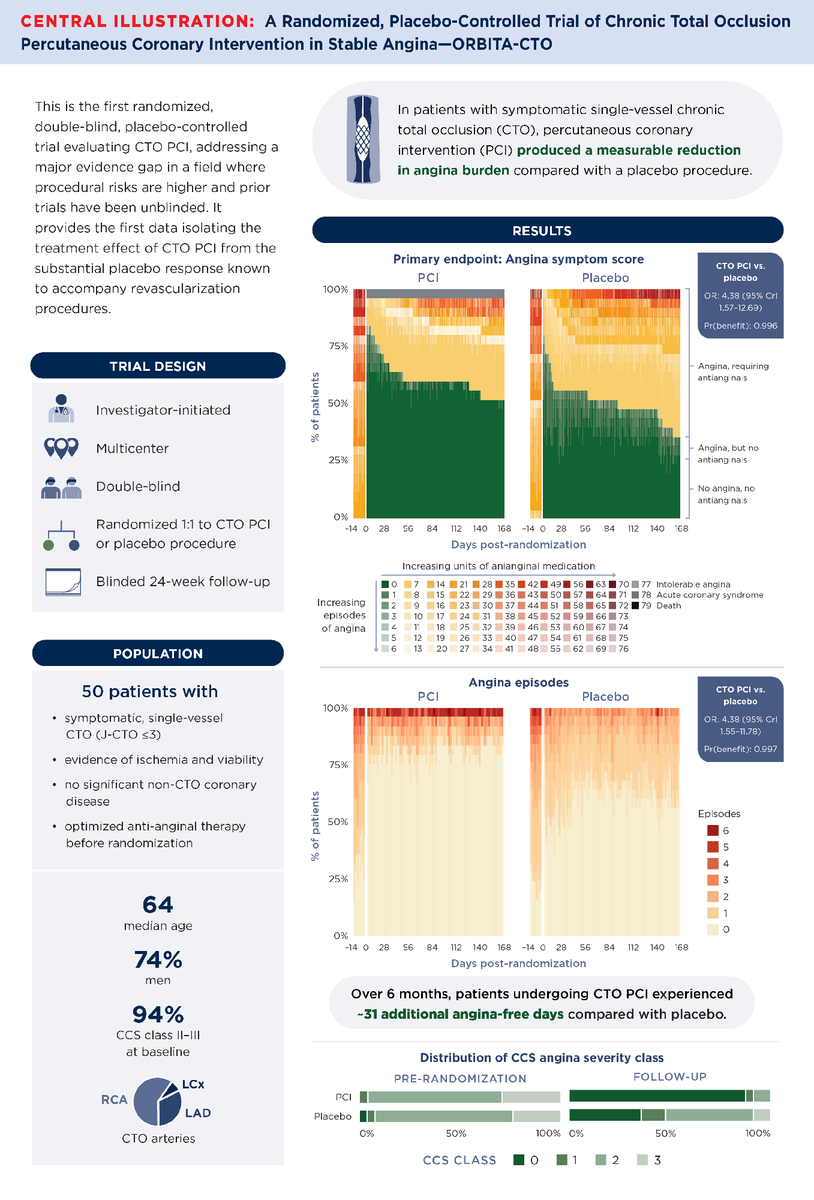
Design: 50 patients, single-vessel CTO, confirmed ischemia + viability, J-CTO ≤3, no bystander disease.
1:1 to CTO PCI or placebo after dual-injection angiography.
All anti-anginals stopped at randomization. Daily symptom tracking via ORBITA-app for 6 months. Patient-initiated re-titration only.
Primary endpoint: angina symptom score (Bayesian ordinal MOST model, daily repeated measures).
CTO PCI vs placebo: OR 4.38 (95% CrI 1.57–12.69) Pr(Benefit) = 0.996
Driven by angina frequency: OR 4.38 (95% CrI 1.55–11.78) Pr(Benefit) = 0.997
In patient-centered terms: CTO PCI yielded ~31 additional angina-free days over 6 months vs placebo.
95% CrI: 11.1–50.7 Pr(Benefit) > 0.999
That's roughly 5 extra angina-free days per month.
SAQ domains were consistent:
Angina frequency: +10.7 (CrI 1.4–20.2)
Physical limitation: +13.5 (CrI 4.5–22.3)
Quality of life: +18.2 (CrI 5.4–30.5)
Summary score: +13.7 (CrI 4.2–23.2)
All Pr(Benefit) ≥ 0.988. CCS class also improved.
Dyspnea and EQ-5D did not separate.
Procedural quality was outstanding: 96% technical success, 92% IVUS-guided, experienced dual-operator teams.
One failed PCI case — averaging 6 angina episodes/day — was included in ITT. This biased against the PCI arm.
But the treatment effect survived it.
Why does this matter so much?
EuroCTO (Werner et al.) showed CTO PCI improved symptoms vs OMT at 1 year, sustained at 3 years. But it was open-label, with 17.5% crossover from OMT to PCI.
Without blinding, the placebo contribution to symptom relief was unknown.
ORBITA-CTO quantified it.
Both arms improved — so yes, the placebo response was substantial.
But the PCI effect was immediate and sustained. The placebo group progressively needed more anti-anginals.
Now, what ORBITA-CTO does NOT prove:
1. Benefit in multivessel disease or high-complexity CTOs (J-CTO 4–5)
2. Prognostic benefit (not designed for hard endpoints)
3. Generalizability beyond expert centers with 96% success rates
4. Benefit on dyspnea or generic quality of life
I know. N=50 is small. Credible intervals are wide. This was an expert-center study with carefully selected lesions. Noted.
But 8,631 follow-up days of daily symptom data, a Bayesian framework designed for this exact scenario, and verified blinding give it far more inferential weight than sample size alone suggests.
For years, CTO PCI skeptics had a legitimate point: no blinded evidence.
That point is now addressed. CTO PCI relieves angina beyond placebo — in well-selected patients, at experienced centers. Agreed.
Hats off to the ORBITA-CTO team for doing this the hard way. Our field is better for it. And by the way, this is not me celebrating the results. I don't do CTO. But it makes me happy to see good medical science being made.
#ORBITACTO #CardiologyX #InterventionalCardiology #ACC26 @JACCJournals
Finally, a sham-controlled CTO PCI trial—and it delivers. ORBITA-CTO: small (n=50), but rigor where it matters—blinding, placebo control, symptom-level data. CTO PCI improves angina beyond placebo, with a clear reduction in episodes and more angina-free days. Not prognosis, not hard endpoints, but real symptom benefit—properly measured. #acc26
https://t.co/UgoJVoX87H
In patients with symptomatic single-vessel chronic total occlusion, percutaneous coronary intervention for coronary chronic total occlusion (CTO PCI) improves angina beyond placebo.
Get the details in #JACC: https://t.co/yX0FDuSOjl #ACC26#PCI#CTO@dr_skhan1
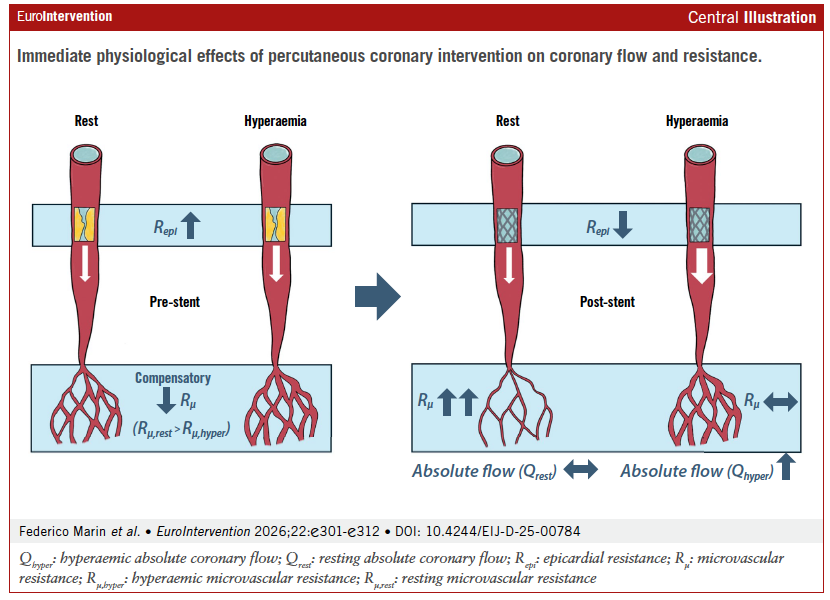
This editorial highlights Marin et al.’s study showing how PCI reshapes coronary flow dynamics in humans, reinforcing key concepts of coronary autoregulation and the physiological basis of FFR.
#CoronaryPhysiology#PCI#FFR#InterventionalCardiology@JEscaned@Guusdewaard
Original paper : https://t.co/PLy11lgRKJ
Probably the most important talk at @CRT_meeting#CRT2026 with Jeff Moses and Antonio Colombo in audience , Gregg Stone on Podium @rallamee and her group’s brilliant science again!
Invasive physiological assessment using continuous thermodilution showed that PCI reduces epicardial resistance and increased hyperaemic coronary flow, while resting flow remained unchanged due to microvascular autoregulation.
https://t.co/PLy11lhpAh
#PCI#FFR #CoronaryPhysiology
@GiovanniLuigiD1@ColletCarlos