They wheeled him in.
Final-year medical student.
Previously healthy.
Yesterday he was on rounds.
Today he could barely sit upright.
His face was an unnatural red.
Not the flush of embarrassment.
The flush of systemic inflammation.
Hands cold.
Clammy.
Trembling.
He tried to answer questions.
The words came slowly.
As if his brain were wading through fog.
“High fever.”
“Vomiting.”
“Almost fainted.”
BP: 82/48
Pulse: 132
Temp: 39.4°C
A red rash covered his trunk.
Flat. Diffuse. Blanching.
It looked harmless. It was not.
Dr X asked only one question:
“When was the last procedure?”
“Cosmetic scalp graft. Three days ago.”
Three days.
That was all it took.
“Expose the scalp.”- Dr X.
The graft sites were inflamed.
No dramatic abscess.
No pouring pus.
Just violated skin.
And beneath it, a toxin factory.
Dr X’s voice changed.
Two large-bore IV lines.
Blood cultures.
Full labs.
Lactate. Coags.
30 mL/kg crystalloids.
Fluid rushed in.
His pressure barely moved.
“Prepare norepinephrine.”
Vancomycin.
Clindamycin.
A student whispered,
“Why clindamycin?”
Dr X did not raise his voice.
“Because this isn’t just infection.”
“This is toxin.”
“These bacteria don’t just invade.”
“They hijack the immune system.”
Superantigens.
They force millions of T-cells to activate at once.
No precision.
No control.
A cytokine explosion.
Capillaries leak.
Blood pressure collapses.
Organs begin to starve.
The rash is not cosmetic.
It is the skin reflecting internal vascular failure.
“Diagnosis?” asked a student.
“Toxic Shock Syndrome.”
Not rare.
Not dramatic in appearance.
But merciless.
“Triggers?” - a student.
Dr X looked at the scalp again.
“Sometimes it’s a tampon.”
“But often…”
-A minor procedure.
-A surgical wound.
-A burn.
-A postpartum infection.
-Nasal packing.
-A small laceration."
The wound may be trivial.
The collapse is not.
“In one to two weeks,” he continued quietly,
“if he survives…
the skin on his palms and soles may peel.”
Desquamation.
The body shedding the memory of the storm.
Dr X paused.
Then, slowly:
“Remember the pattern.
-High fever.
-Sudden hypotension.
-Diffuse erythroderma.
-GI symptoms.
-Recent invasive exposure.”
“If you wait for cultures…”
He looked at the students.
“…the toxin will not wait for you.”
The trolley had rolled toward the ICU.
Monitors. Vasopressors. Lines.
Twenty-three years old.
A future doctor.
Nearly undone by a few millimeters of broken skin.
Dr X signed the notes.
Then he said, almost to himself:
“The most dangerous wounds are the ones that look small.”
@vmuecke_k@kbv4u@ninawarken@GKV_SV Die Fahrtkosten sind exorbitant im Vergleich zur einfachen medizinischen Leistung. Wenn das Pflegeheim oder der Dienstarzt nur 20% davon bekämen, würde jeder Katheter ambulant versorgt werden. Dann gäbe es nur ein Gerangel und Gedränge darum, wer den Wechsel machen darf.
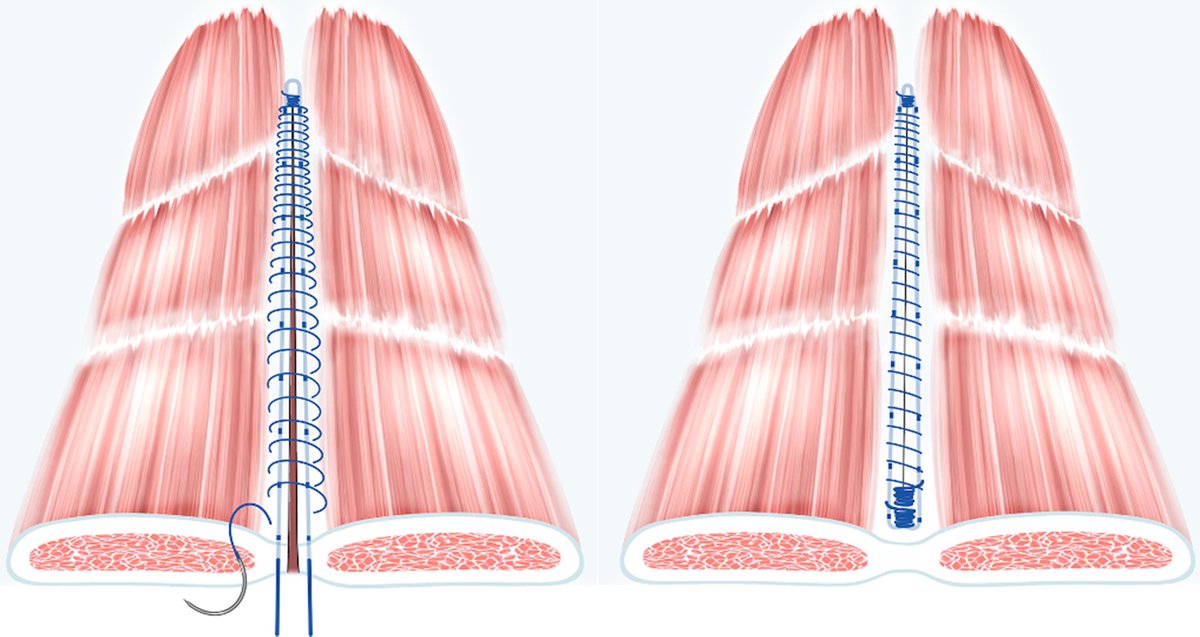
Reinforced tension-line suture after laparotomy: long-term results of Rein4CeTo1 randomized clinical trial
➡️https://t.co/AqYmnd5yex
The aim of this randomized clinical trial was to investigate whether a reinforced tension-line (RTL) suture reduces 3-year computed tomography-detected incisional hernia incidence. The RTL technique significantly reduced the incidence of incisional hernia compared with the standard facial closure technique in patients undergoing open colorectal cancer surgery. The incisional hernia incidence was 6 of 43 (14%) in the RTL and 21 of 58 (36%) in the standard facial closure group.
👏👏👏Charlotta L Wenzelberg , Peder Rogmark , Olle Ekberg , Ulf Petersson , Carl-Fredrik Rönnow
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @BJSAcademy@BJSurgery@eurohernias #hernia #hernia @herniaistanbul@BritishHernia@HerniaIndia@awrsurgeons
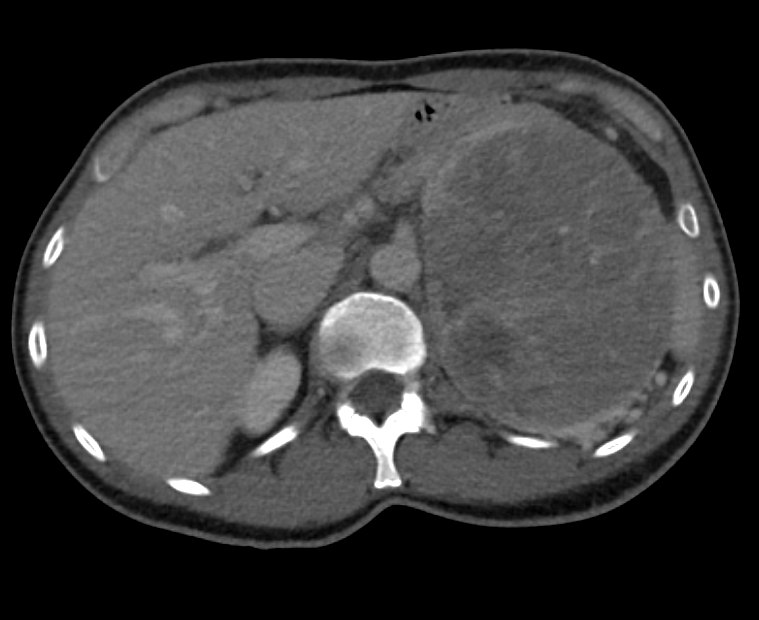
Male, 70 years old, status post cadaveric donor kidney transplantation 12 years ago, presented with decreased urine output for 2 weeks. Serum creatinine increased from 0.7 to 2.6 mg/dL.
Ultrasound & CTNC was done.
What is Diagnosis? (? transplant ureter inguinal hernia)
In muscle-invasive bladder cancer, ctDNA-guided atezolizumab led to longer disease-free survival (9.9 vs. 4.8 months), as well as to longer overall survival (32.8 vs. 21.1 months), than placebo among ctDNA-positive patients. Full IMvigor011 phase 3 trial results and Research Summary: https://t.co/nbCPzF4Pxy
NO ONE should pay to submit an abstract to a scientific conference.
Your abstracts should not be a revenue stream for medical societies.
Please, stop this NOW🙏
@GaliBillyyoung Unfortunately, pain is not a key symptom. In case of ischemic priapism, the erection is unpleasant, but for many patients it is not grave enough to seek medical help. Education in risk patients is key to preventing damage to the penis. https://t.co/22IDJ23LvS
Reminder that you’re NOT obligated to spend 2-3 hr robotically lysing adhesions before giving yourself permission to convert.
Conversion rate tends to become a thing that everyone feels they need to minimize, and it leads to a lot of time spent in heroic 🤖 adhesiolysis.
The first e-book edition of the Urology Textbook is ideal for offline reading and quick reference. With over 1300 pages and hundreds of illustrations, it’s the perfect companion for #residents and medical students.