A wide QRS tachycardia is ventricular tachycardia (VT) until proven otherwise.
The two most common causes are:
⬜ Ventricular tachycardia (VT)
🟪 Supraventricular tachycardia (SVT) with aberrant conduction
Other less common causes include:
🟦SVT with pre-excitation (WPW syndrome)
🟩SVT with baseline bundle branch block
🟨 Hyperkalemia
🟧 Ventricular pacing
A practical ECG clue:
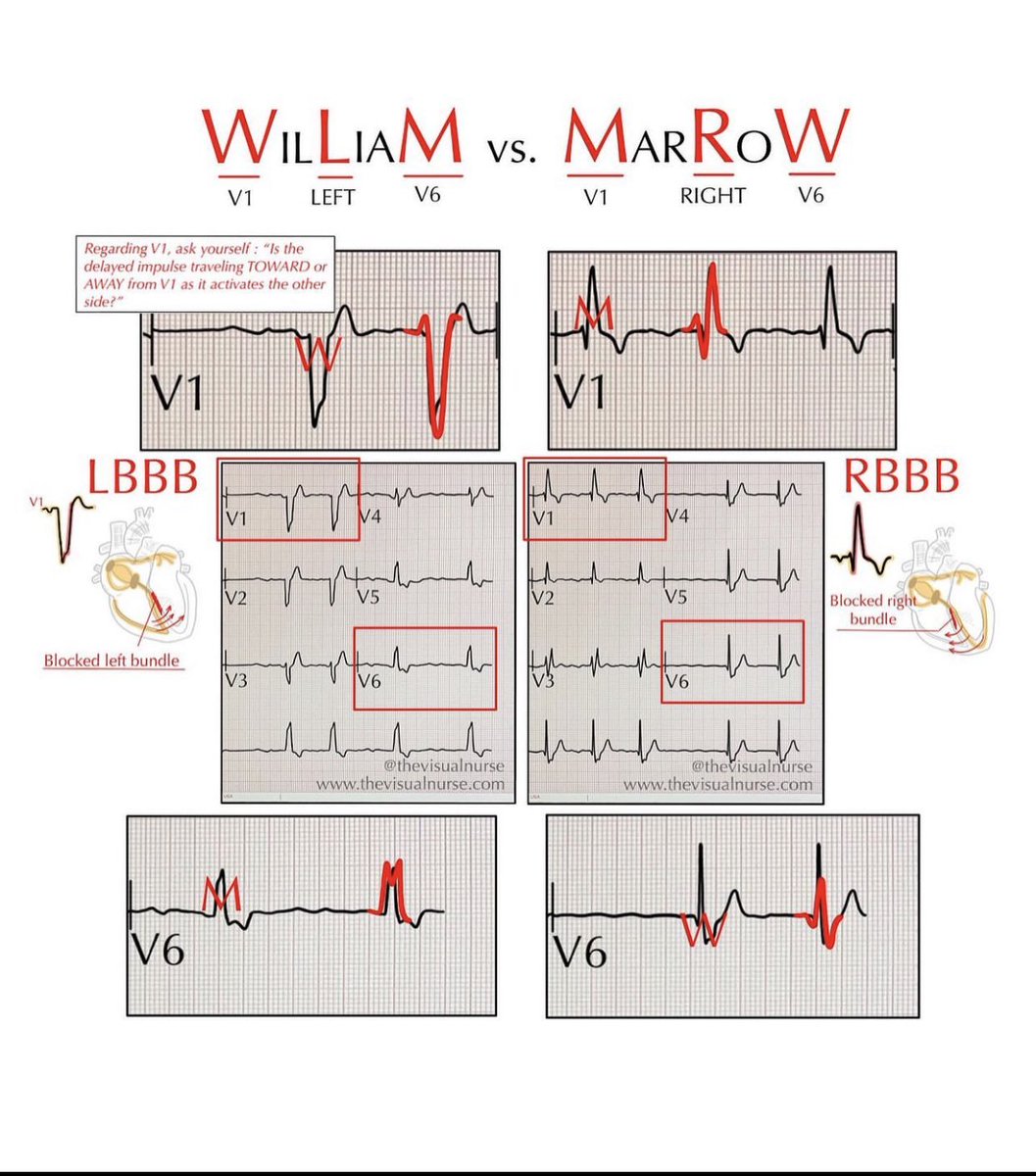
- LBBB-type wide QRS: the terminal portion of the QRS in V1 is predominantly negative
- RBBB-type wide QRS: the terminal portion of the QRS in V1 is predominantly positive
If the QRS pattern in V1 is atypical (such as an Rs or qRs pattern), the rhythm is much more likely to be ventricular tachycardia.
Key point:
Because VT is the most common and potentially life-threatening cause of a wide QRS tachycardia, it should be the default diagnosis until an alternative is confidently established.
Dexamethasone suppression testing follows a stepwise approach: screen for hypercortisolism, confirm the diagnosis, then localise the source.
#Endocrinology#InternalMedicine#CushingSyndrome
Heart failure patients can often be classified at the bedside using two simple questions:
1. Is there congestion? (Wet vs Dry)
2. Is tissue perfusion adequate? (Warm vs Cold)
This creates four hemodynamic profiles that carry important prognostic and therapeutic implications:
🟣Warm & Dry
- Normal perfusion
- No significant congestion
- Represents compensated/stable HF
🔵Warm & Wet
- Congestion with preserved perfusion
- Most common profile in acute decompensated HF
Symptoms may include orthopnea, elevated JVP, pulmonary rales, edema, and an S3 gallop
🔵Cold & Dry
- Hypoperfusion without overt congestion
- May present with cool extremities, narrow pulse pressure, or hypotension
⚫Cold & Wet
- Congestion plus hypoperfusion
- Highest-risk profile
- Often represents cardiogenic shock and requires urgent intervention
This bedside classification is more than descriptive, it helps guide treatment decisions, risk stratification, and prognosis in patients with heart failure.
Reference: Nohria A, Tsang SW, Fang JC, et al. Clinical assessment identifies hemodynamic profiles that predict outcomes in patients admitted with heart failure. Journal of the American College of Cardiology. 2003;41(10):1797–1804.
Wide QRS Tachycardia? It's Not Always VT
This ECG panel compares V₁ and V₆ leads in both LBBB-type and RBBB-type QRS morphologies across common causes:
1️⃣ Ventricular tachycardia (VT)
2️⃣ SVT with aberrancy
3️⃣ SVT with preexcitation (WPW)
4️⃣ SVT with baseline abnormal ECG
5️⃣ SVT with hyperkalemia
6️⃣ Ventricular pacing
Observe how the QRS morphology changes with each condition. Certain clues like AV dissociation, fusion beats, or extreme axis favor VT, while others may suggest supraventricular origin.
This chart is a great reference for ECG interpretation, especially in acute settings.
Reference: Zipes & Jalife, Cardiac Electrophysiology: From Cell to Bedside
Premature Ventricular Complexes (PVCs): More Than Just an Extra Beat
PVCs are early beats that originate from the ventricles rather than the normal cardiac conduction system. While often benign, they can alter cardiac rhythm, conduction, and even blood flow.
Key concepts illustrated in this figure:
⚪ A late PVC is usually followed by a compensatory pause, creating the sensation of a "skipped beat."
⚪ Some PVCs conduct backward into the atria (retrograde atrial activation), resetting the sinus node and producing a noncompensatory pause.
⚪ Depending on timing, a PVC may be followed by a ventricular escape beat or a fusion beat, where impulses from the sinus node and ventricle combine.
⚪ PVCs can also cause concealed conduction into the AV node, resulting in a slightly prolonged PR interval on the next sinus beat.
Importantly, PVCs may have significant hemodynamic consequences. Because ventricular contraction occurs prematurely, filling time is reduced, leading to a weak or absent arterial pulse. Frequent PVCs can therefore create an effective heart rate much lower than the ECG heart rate.
Understanding PVC timing and their effects on conduction helps explain why some patients experience palpitations, dizziness, or reduced cardiac output despite seemingly modest rhythm disturbances.
Reference: Braunwald's Heart Disease, 12th Edition.
Summary of the different types of ventricular complexes.
1️⃣ Interpolated PVCs
- A PVC occurs between two normal beats without disrupting the sinus rhythm.
- No compensatory pause.
- Often seen in bradycardic patients.
2️⃣ PVCs in Bigeminy
- Every normal beat (sinus beat) is followed by a PVC → Regular pattern.
- The PVC is premature and typically has a wide QRS complex.
3️⃣ PVCs in Trigeminy
- Two normal beats followed by a PVC, repeating in a cycle.
- A predictable ventricular ectopy pattern.
4️⃣ Multifocal PVCs
- PVCs originate from multiple foci, showing different QRS morphologies.
- Indicates more ventricular instability than unifocal PVCs.
5️⃣ Paired or Back-to-Back PVCs
- Two consecutive PVCs occurring without an intervening sinus beat.
6️⃣ Nonsustained Monomorphic Ventricular Tachycardia (NSVT)
- Three or more consecutive PVCs at a rate >100 bpm, but lasting <30 sec.
- Monomorphic: All QRS complexes have the same shape (single ectopic focus).
7️⃣ Nonsustained Polymorphic Ventricular Tachycardia (NSVT)
✅ Three or more PVCs lasting <30 sec, but QRS morphology varies (multiple ectopic foci).
✅ Often associated with long QT syndrome, ischemia, or electrolyte abnormalities.
8️⃣ Ventricular Fibrillation (VF), A Medical Emergency
- Chaotic, disorganized electrical activity with no identifiable QRS complexes.
- The heart is quivering instead of pumping, leading to no cardiac output.
Possible rhythms in Wolff-Parkinson-White (WPW) syndrome.
Schematic representation of possible rhythms in a patient with an accessory atrioventricular (AV) bypass tract.
A. During sinus rhythm, the ventricle may be activated by conduction over the accessory pathway (AP) and through the normal AV conduction system. The QRS complex may be narrow if ventricular activation occurs primarily via the AV node, or wide and preexcited if activation occurs mainly through the AP.
B. During orthodromic reentrant tachycardia, antegrade conduction occurs through the AV node and normal conduction system, while retrograde conduction occurs via the AP. The resulting tachycardia shows a narrow QRS complex.
C. In antidromic tachycardia, the AP serves as the antegrade limb of the reentrant circuit, and the AV node with the normal conduction system serves as the retrograde limb. The resulting tachycardia shows a wide QRS complex.
D. When atrial fibrillation (AF) occurs in a patient with a manifest accessory pathway, antegrade conduction to the ventricle may occur through either the AV node or the AP. The QRS morphology may be narrow when conduction is primarily via the AV node, or wide and preexcited when conduction occurs through the AP. The QRS morphology may vary from beat to beat during AF.
@TrackYourHeart
Source: Morton’s Cardiac Catheterization Handbook( pge 314
The STEMI vs NSTEMI paradigm may be missing the real target.
Occlusion Myocardial Infarction (OMI) refers to an acute myocardial infarction caused by a culprit coronary artery that is completely or nearly completely occluded, resulting in critically reduced blood flow to the myocardium. In simple terms, OMI identifies the patients who need urgent reperfusion because an artery is blocked, regardless of whether the ECG fulfills STEMI criteria.
A 2024 study of 334 ACS patients found that 40% of OMI patients did NOT meet STEMI criteria. Despite having an acutely occluded coronary artery, these patients were often classified as NSTEMI and experienced major delays in treatment.
Among STEMI-negative OMI patients, only 11% underwent PCI within the first 12 hours, compared with 77% of STEMI-positive OMI patients.
The concerning part is that both groups had remarkably similar disease severity:
🔺 Similar rates of PCI
🔺 Similar rates of mechanical complications
🔺 Similar rates of electrical complications
🔺 Similar angiographic evidence of acute coronary occlusion
In other words, many patients without classic ST-elevation had the same dangerous pathology that traditionally prompts emergency cath lab activation.
The authors argue that focusing solely on STEMI criteria can cause clinicians to miss a substantial number of patients with acute coronary occlusion. Instead, ECG interpretation should focus on identifying OMI patterns, including hyperacute T waves, de Winter pattern, posterior MI, reciprocal changes, modified Sgarbossa criteria, and other STEMI equivalents.
The artery does not care whether the ECG meets STEMI criteria.
Time is myocardium. The goal is not simply to find ST elevation. The goal is to identify acute coronary occlusion and restore blood flow before irreversible myocardial injury occurs.
Perhaps it is time to shift the conversation from STEMI vs NSTEMI to what truly matters: OMI vs NOMI.