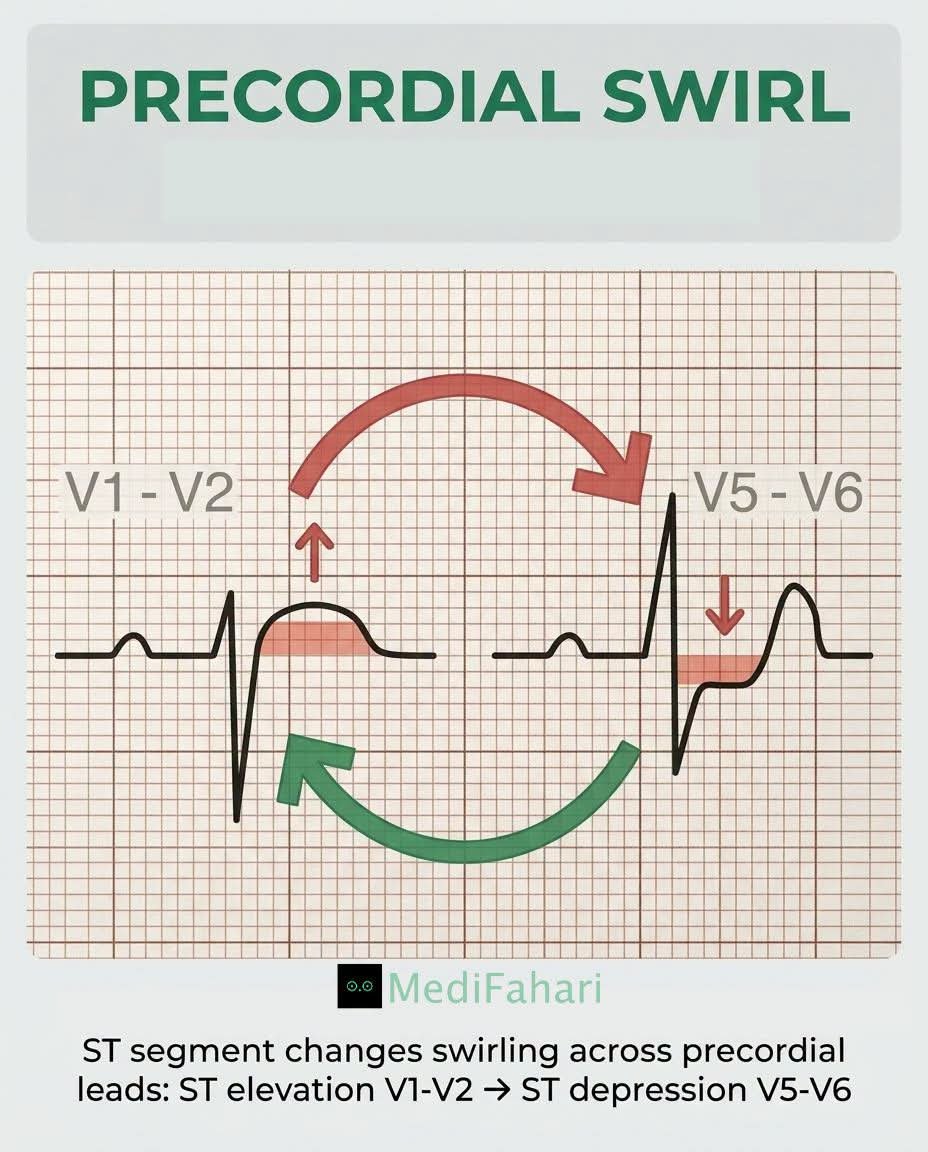
Not every coronary artery occlusion with present with ST elevation, and not every ST elevation means coronary occlusion. Treat the Occlusion and patient not ST elevation, a blocked artery needs cath lab NOW! Even without ST elevation. Time is myocardium.❤️ #OMI vs STEMI paradigm
Some people criticize #MedX for misinformation. But it's also one of the best places to learn and just as importantly, to unlearn.
At first glance, this telemetry strip looks like torsades de pointes. Thousands voted for TdP. But a closer look tells a different story.
This is telemetry artifact masquerading as torsades de pointes
Rationale:
- QRS complexes continue to march through the arrhythmia. True torsades replaces the native ventricular rhythm. It does not allow normal QRS complexes to appear at regular intervals throughout the episode.
- The clinical context doesn't fit well.
The patient had normal electrolytes, no QT-prolonging medications, and no cardiac history. While torsades can occur unexpectedly, these findings lower the pretest probability.
- Artifact has common explanations. In an elderly patient with pneumonia, shivering, coughing, movement, or loose telemetry electrodes can produce dramatic waveforms that mimic polymorphic VT.
The most important lesson is simple:
Treat the patient, not the monitor
A 86-year-old with pneumonia develops this telemetry pattern. Electrolytes are normal, no culprit drugs, and no cardiac history. What rhythm are you seeing, and what would you do next?
In the ruins left after an old battle arises something new. The TB -aspergillosis unholy sisterhood. The battle doesnt always end with antiTBs. Always follow up for postTB complications
Spot the aspergilloma
🫁 ARDS… or something else?
Every intensivist has faced it.
A patient arrives with acute hypoxemic respiratory failure, bilateral infiltrates, severe oxygenation impairment, and fulfills all clinical criteria for ARDS.
But what if it is not ARDS?
A timely review published in Intensive Care Medicine reminds us that approximately 8% of patients meeting ARDS criteria have no identifiable classical ARDS risk factor, and some of these patients harbor highly treatable diseases that require a completely different therapeutic strategy.
The authors propose a practical diagnostic framework for identifying ARDS mimickers, particularly when the presentation includes:
🔹 No clear ARDS risk factor
🔹 Subacute symptom onset
🔹 Extrapulmonary manifestations
🔹 Diffuse alveolar hemorrhage
🔹 Unexpected radiologic patterns
The major categories include:
✅ Immune-mediated diseases
• ANCA-associated vasculitis
• Anti-GBM disease
• Idiopathic inflammatory myopathies (anti-MDA5, antisynthetase syndrome)
✅ Drug-induced lung injury
• Amiodarone
• Chemotherapy
• mTOR inhibitors
• Immune checkpoint inhibitors
✅ Neoplastic pulmonary infiltration
✅ Idiopathic disorders
• Acute eosinophilic pneumonia
• Organizing pneumonia (OP)
One of the most useful concepts from this review is that diagnosis should not rely solely on the chest CT.
Instead, intensivists should combine:
📌 Detailed history and medication review
📌 Extrapulmonary examination (skin, joints, muscles, kidneys)
📌 Autoimmune testing
📌 Bronchoscopy with BAL
📌 Pattern recognition on CT imaging
The article highlights several time-critical diagnoses not to miss:
⚠️ Anti-MDA5 dermatomyositis and antisynthetase syndrome
ICU mortality approaches 50%, and up to 20% of patients require VV-ECMO. Early aggressive immunosuppression is essential.
⚠️ ANCA-associated vasculitis and anti-GBM disease
Prompt recognition of diffuse alveolar hemorrhage and initiation of immunosuppression can be life-saving and kidney-saving.
⚠️ Immune checkpoint inhibitor pneumonitis
A rapidly growing cause of severe respiratory failure in oncology patients that often responds to corticosteroid therapy if recognized early.
The key message is simple:
Not every patient fulfilling ARDS criteria has diffuse alveolar damage.
When classical risk factors are absent, the diagnosis should trigger curiosity rather than closure.
Because sometimes the difference between survival and mortality lies in recognizing the mimicker.
Question for the ICU community:
What is the most memorable ARDS mimicker you have encountered in your practice?
Reference 📚
Bay P, Gibelin A, de Prost N. Acute respiratory distress mimickers: a practical approach for intensivists. Intensive Care Medicine. 2026. DOI: 10.1007/s00134-026-08496-1.
❤️ Pressure-Volume Loops at the Bedside: Are We Finally Measuring What Really Matters in Cardiogenic Shock?
For decades, cardiogenic shock management has focused on cardiac output, blood pressure, filling pressures, lactate, and cardiac power.
A fascinating multicenter study published in the ASAIO Journal proposes a practical bedside method to estimate pressure-volume (PV) loop energetics using only pulmonary artery catheter and echocardiographic data, avoiding the need for invasive conductance catheters.
Why does this matter?
Traditional hemodynamic variables tell us about flow and pressure.
PV-loop analysis tells us about:
📌 Ventriculoarterial coupling (VAC)
📌 Ventricular efficiency
📌 Stroke work (SW)
📌 Potential energy (PE)
📌 Pressure-volume area (PVA)
📌 Myocardial energetic demand
These parameters may provide a much deeper understanding of whether a therapy truly unloads the failing ventricle.
Key Findings
🔹 Microaxial flow pump support in AMI-related cardiogenic shock
The most striking observation was a reduction in arterial elastance and improved ventriculoarterial coupling, accompanied by increased stroke work but decreased pressure-volume area.
This translated into an improvement in estimated ventricular efficiency from approximately 32% to 40%, suggesting genuine ventricular unloading and lower energetic expenditure.
🔹 IABP support in AMI-related shock
IABP improved ventriculoarterial coupling and reduced filling pressures but produced a more modest energetic effect compared with microaxial support.
🔹 Heart failure-related cardiogenic shock
The physiological response was far more heterogeneous. Changes in pressure-volume area and ventricular energetics were inconsistent, highlighting that device effects may depend strongly on shock etiology.
Why This Study Is Important
This work reinforces a concept increasingly discussed in advanced heart failure and shock programs:
The goal is not simply increasing cardiac output.
The goal is improving systemic perfusion while simultaneously reducing myocardial oxygen consumption and ventricular workload.
A patient can have a higher cardiac output while still operating at an unfavorable energetic state.
Pressure-volume analysis may reveal this hidden physiology.
Practical ICU Takeaway
When evaluating mechanical circulatory support, we should ask three questions:
1️⃣ Is systemic perfusion improving?
2️⃣ Is ventricular filling pressure decreasing?
3️⃣ Is ventricular energetic demand falling?
Only when all three occur simultaneously can we confidently say that true ventricular unloading has been achieved.
The future of cardiogenic shock management may be less about isolated hemodynamic variables and more about understanding the complete interaction between the ventricle and the arterial system.
Reference 📚
Ortega-Hernández JA. ASAIO Journal. 2026. DOI: 10.1097/MAT.0000000000002737.
Medicine becomes art when science meets the heart. It is the gentle, humane soul of healing—where compassion and dignity breathe life into every treatment. To mend the body, we must first touch the heart with kindness, reminding each person they are seen, valued, and never alone
Uganda’s Unpaid Medical Interns: A Crisis at the Heart of Public Healthcare
Uganda’s public health system is facing a deepening moral, legal, and policy crisis following the government’s refusal to pay medical interns. At the center of this dispute are young doctors who, after years of intense and costly training, are expected to shoulder the backbone of hospital care, without pay. The decision has far-reaching consequences for healthcare delivery, medical education, and the future of the profession in Uganda
Medical interns in Uganda are not observers or trainees in a casual sense. They are frontline healthcare providers. In many public hospitals, interns cover critical staffing gaps, run wards, attend to emergencies, clerk patients, prescribe under supervision, and provide round-the-clock care.
In practice, interns do most of the regular medical work that keeps hospitals functional, especially in regional referral hospitals where shortages of senior doctors are chronic. Demotivating interns through non-payment directly undermines patient care, increases preventable deaths, and overburdens the few fully employed doctors who remain. Refusing to pay interns while continuing to rely on their labor amounts to institutionalized exploitation.
Before internship, a Ugandan medical doctor spends at least five years at university, followed by internship as a mandatory requirement for full registration. Medical education is among the most demanding and expensive courses in the country. By the time students reach internship, many come from families already financially exhausted. Internship pay is therefore not a luxury, it is basic subsistence, covering rent, food, transport, among others.
Denying interns pay after such prolonged investment effectively turns medical training into a pathway of debt, distress, and despair. The situation poses a sharp dilemma, especially for government-sponsored medical students.
On one hand, the state argues fiscal constraints and frames internship as “training.” On the other hand, it compels graduates to serve, posts them to hospitals, assigns shifts, and disciplines them as workers. This contradiction raises fundamental questions. If internship is compulsory national service, why is it unpaid? Why should interns offer an unpaid service in government hospitals? What’s government’s commitment to universal healthcare?
Uganda’s approach stands in stark contrast to practices across much of Africa. In Kenya, Medical interns are salaried government employees, with formal contracts and monthly pay. In South Africa, Interns receive structured remuneration and are fully integrated into the public service payroll. In Rwanda, Internship is funded as part of national health workforce planning, with clear state responsibility. In Ghana, House officers (interns) are paid and recognized as essential health workers.
In these countries, governments acknowledge a basic truth: you cannot sustain a health system on unpaid labor.
Uganda’s refusal to pay interns risks isolating the country, accelerating brain drain, and making medicine unattractive to talented students, especially those from poor backgrounds.
The unpaid internship policy has consequences beyond medical interns themselves. Patients suffer from demoralized staff and service disruptions
Rural and public hospitals face collapse as interns withdraw labor. Medical students reconsider their career choices or plan to leave the country. Public trust in health governance erodes.
Uganda cannot claim commitment to universal healthcare while refusing to pay the very doctors who keep hospitals running. Internship is not charity work; it is essential labor performed after years of specialized training. Government decision undermines its health system, exploits young professionals, and jeopardizes the future of medical education in Uganda.
Paying medical interns is not merely a budgetary decision; it is a test of justice, foresight, and national priorities.
Medical interns are doctors under apprenticeship, not free labour.
Unpaid internship is not reform. It is exploitation.
Pay interns. Protect training. Protect patients.
//END//
“PaO₂/FiO₂ and SpO₂/FiO₂ ratios revisited: Useful, misleading, or both?” in the Journal of Intensive Medicine. A review exploring the strengths, pitfalls, and future of oxygenation metrics in ARDS and respiratory failure.
https://t.co/etYyBGzhys