Lp(a) vs CAC: Which One Wins?
Many clinicians assume that elevated Lp(a) makes CAC scoring less useful because Lp(a) is associated with non-calcified plaque.
This new study of 11,319 individuals suggests otherwise.
✅ Elevated Lp(a) increased risk across all CAC strata.
✅ CAC remained a powerful risk discriminator.
✅ Even with Lp(a) >50 mg/dL, individuals with CAC=0 had remarkably low absolute event rates over ~15 years.
The highest risk?
Lp(a) >50 mg/dL + CAC ≥300
(HR 6.12).
Perhaps the lesson is simple:
Lp(a) tells us who is biologically predisposed.
CAC tells us how much of that risk has actually become disease.
And those are not the same thing.
#LpA #Prevention #CardiacCT #CAC #Atherosclerosis #Cardiology #CardiovascularPrevention #Imaging #CCTA
🫀⚡ We’ve spent decades saying: “Use echo for shunts… maybe MRI if you’re serious.” Photon Counting CT just entered the conversation.
I've been saying for 2 decades. Cardiac CT is not just for coronary arteries.
This elegant Radiology case series shows something simple but powerful:
👉 PCCT + iodine maps can directly visualize cardiac shunts and flow.
Not infer them.
Not suspect them.
👉 See them.
Three different scenarios:
👉 coronary artery fistula
👉 anomalous pulmonary venous return
👉 interatrial communication
All clearly depicted with:
⚡ low-keV reconstructions
⚡ iodine maps
⚡ direct visualization of contrast jets
Let’s translate
Echocardiography:
👉 operator-dependent
👉 acoustic windows
👉 indirect flow assessment
MRI:
👉 powerful
👉 but longer, complex, less available
PCCT?
👉 anatomy + flow information in one fast acquisition
The real game changer is iodine mapping
Because it allows:
👉 visualization of contrast distribution
👉 identification of shunt pathways
👉 direct depiction of flow jets across defects
As clearly shown in the figure on page 1, where iodine maps highlight the abnormal connections and the contrast jet traversing them.
My take
This is not about replacing echo or MRI.
It’s about something more interesting:
👉 collapsing anatomical and functional imaging into one modality.
Because once you can:
👉 see the structure
👉 see the contrast
👉 infer the flow
…in a single dataset,
the traditional boundaries between modalities start to blur.
Bottom line
Photon Counting CT is not just improving coronary imaging.
It is expanding into:
👉 structural and congenital heart disease
with a level of clarity that is hard to ignore.
⚡ The future question may not be:
“Which modality should I use?”
But:
👉 “Which modality gives me everything at once?”
#PCCT #PhotonCounting #CardiacCT #CongenitalHeartDisease #CardiacShunts #IodineMapping #Radiology #Cardiology #ImagingInnovation
🫀 What a great case!
70-year-old woman with metastatic [withheld].
What’s the diagnosis? 🤔
Check out the full blog post: https://t.co/ESiwmtaseY
#Radres#Cardiology#RadTwitter#CardiacMRI#MedEd
Crazy. The Medicare allowed payment for a doctor to read a coronary CT angio is about a hundred bucks. But Medicare will pay an AI company $1000?
How did this happen?
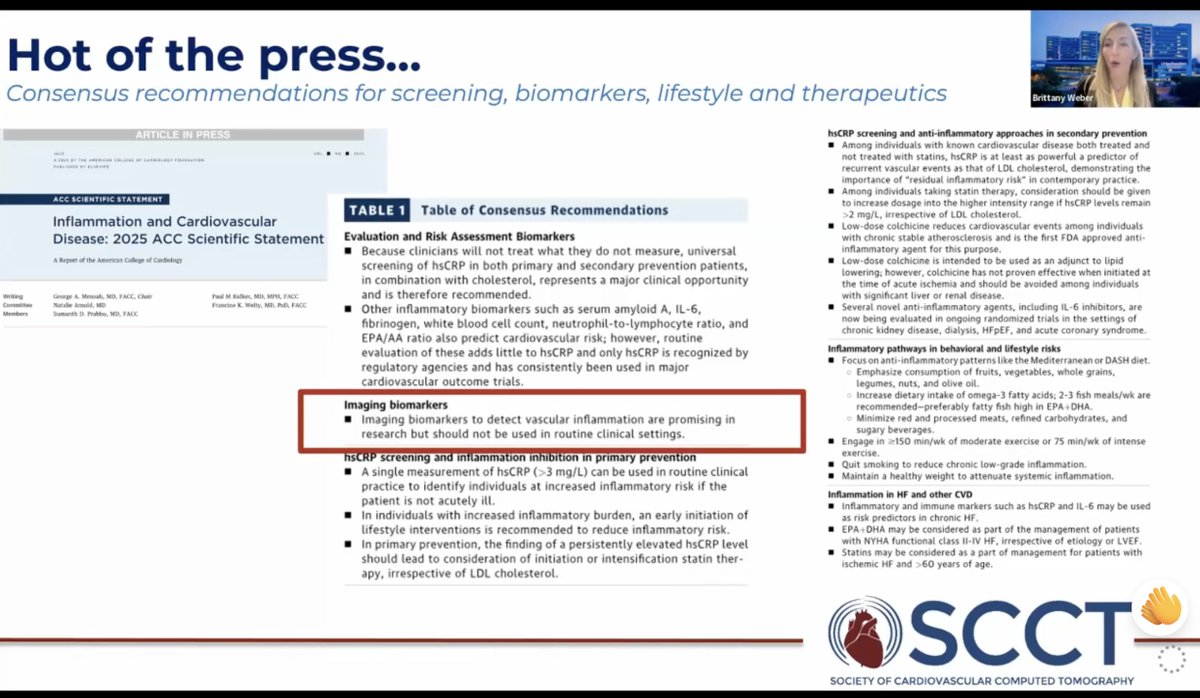
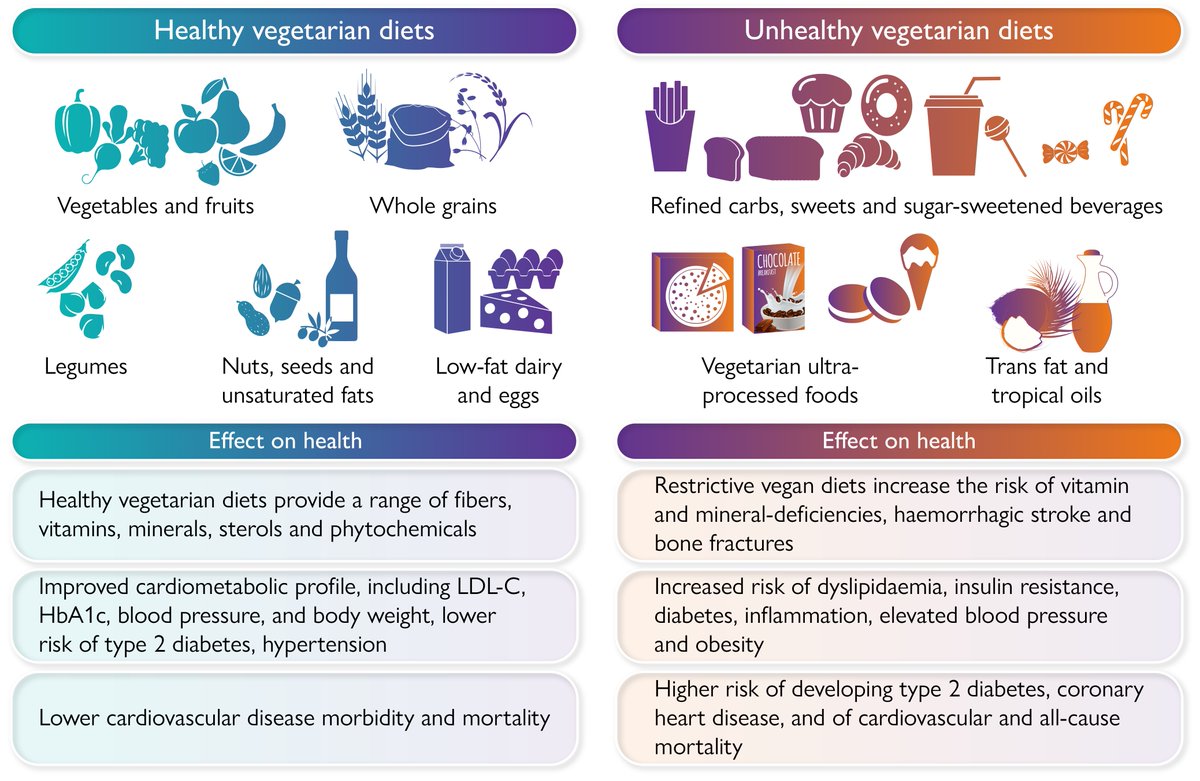
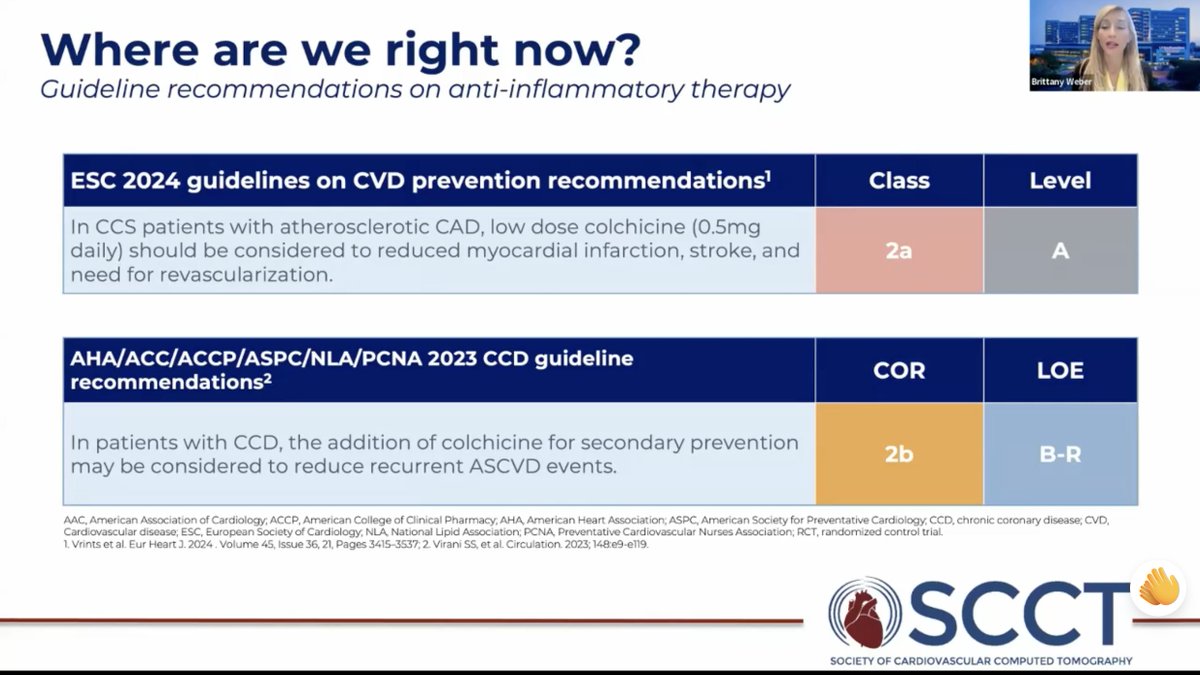
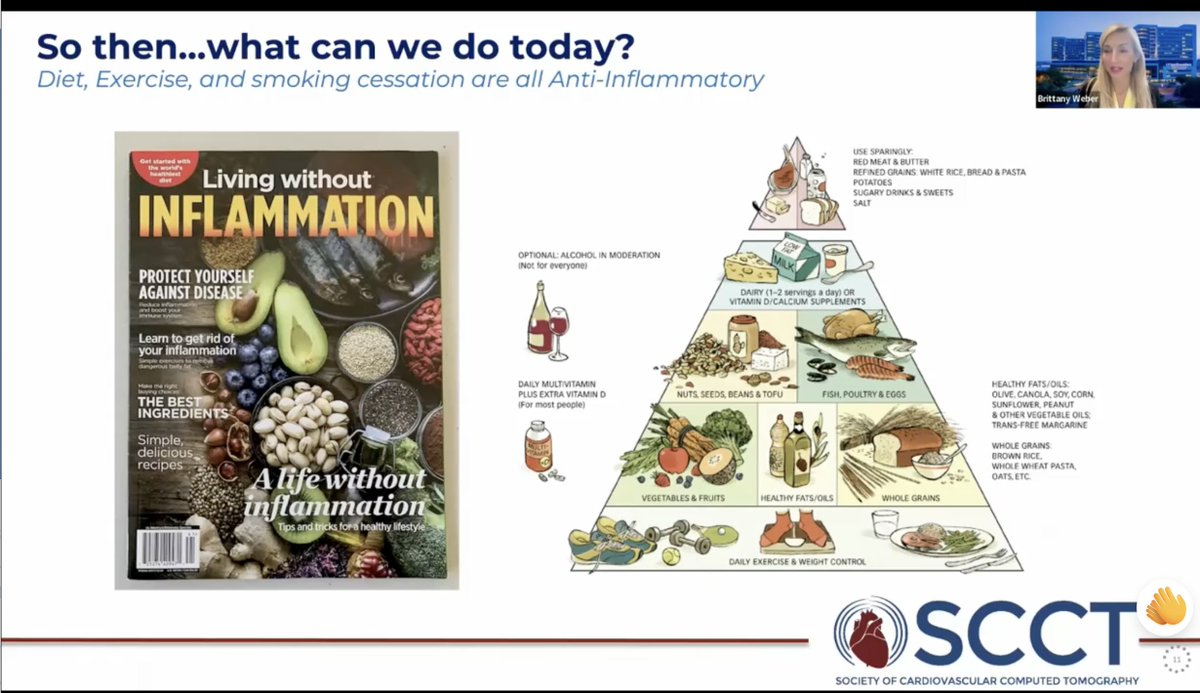
"Diet, exercise, and smoking cessation are all anti-inflammatory" @Bweber04
👏Great summary of current state of screening and treatment of inflammation @Heart_SCCT@UTSWMedCenter
Excited to share our @JACCJournals#JACCIMG paper led by ⭐️@Bweber04 on AI detection of CAC on chest CT among 2,546 individuals with IMID (SLE/RA/Psoriasis) who did not have hx of ASCVD ~50% had CAC --> most not on statin!
➡️Over 8 yrs, AI CAC provided robust a/w MACE + ACM
*ACC Imaging Council Survey: Define what the job market looks like* - https://t.co/Kmld24UBZj
Hi everyone, if you have just a few minutes today, the ACC Imaging Council would love if it you could fill out the following brief survey.
We are aiming to gather *anonymized* data on how advanced cardiac imagers jobs are:
1. Structured (# clinic days, # imaging days, call etc.)
2. Valued (MGMA, Doximity, MedAxiom data does not stratify by advanced imaging vs general rads/cards)
We hope to share the results with everyone in the community to help you understand your local and national market and empower you to better advocate for yourself in any new or retention contracts to come.
The amount of value this survey will add will completely depend on participation, so please share widely with your colleagues and friends in advanced cardiac imaging!
I would appreciate a RETWEET
Best,
Your friends on the ACC Imaging Council
#ACCImaging @ACCinTouch@RonBlankstein@WilliamZoghbi@mdicarli
https://t.co/DAZhKBGomb
#ACCImaging pic for the attention
@mmamas1973@DrMarthaGulati@iamritu@onco_cardiology@OKhaliqueMD@rooshaparikh@Doc_Tiger
Very nice discussion on relapsed #SCLC by Dr. @Arohatgi at #WCLC24. ADCs showing promise and easier to deliver than a BiTE like tarlatamab. No clear biomarker but encouraging efficacy. But we need randomized data to provide clear perspective.
i mean it when i say that the Apple Vision Pro will be a game changer for education
here’s how I studied the heart 5 years ago vs how I can study it today, credit to the visionOS app Insight Heart
the contrast in experience and comprehension can’t be denied
Loved working with 🌟 @ACCinTouch FIT @abavishi23 on this sports cardiology piece 👇on advising symptomatic athletes on their training regimen during their diagnostic evaluation. #SportsCardio
https://t.co/rG2Vno1OqD
Last week's Medicine Grand Rounds video presentation is now available for viewing on our #WUDeptMedicine YouTube Channel.
Farhan M. Katchi, MD, FACC @FKatchiMD@WashUCardiology@MIRImaging@WUSTLmed presented.
Click the link for the presentation> https://t.co/rN8Tg6FQS6
Join us Thursday, December 14th for Medicine Grand Rounds. Farhan M. Katchi, MD, FCC @FKatchiMD@WashUCardiology@WUSTLmed presents:
"Evolving Role of Coronary CT Imaging to Predict Cardiovascular Risk"
We hope you'll join us to support the speaker. Link> https://t.co/aOS4sEOxpR
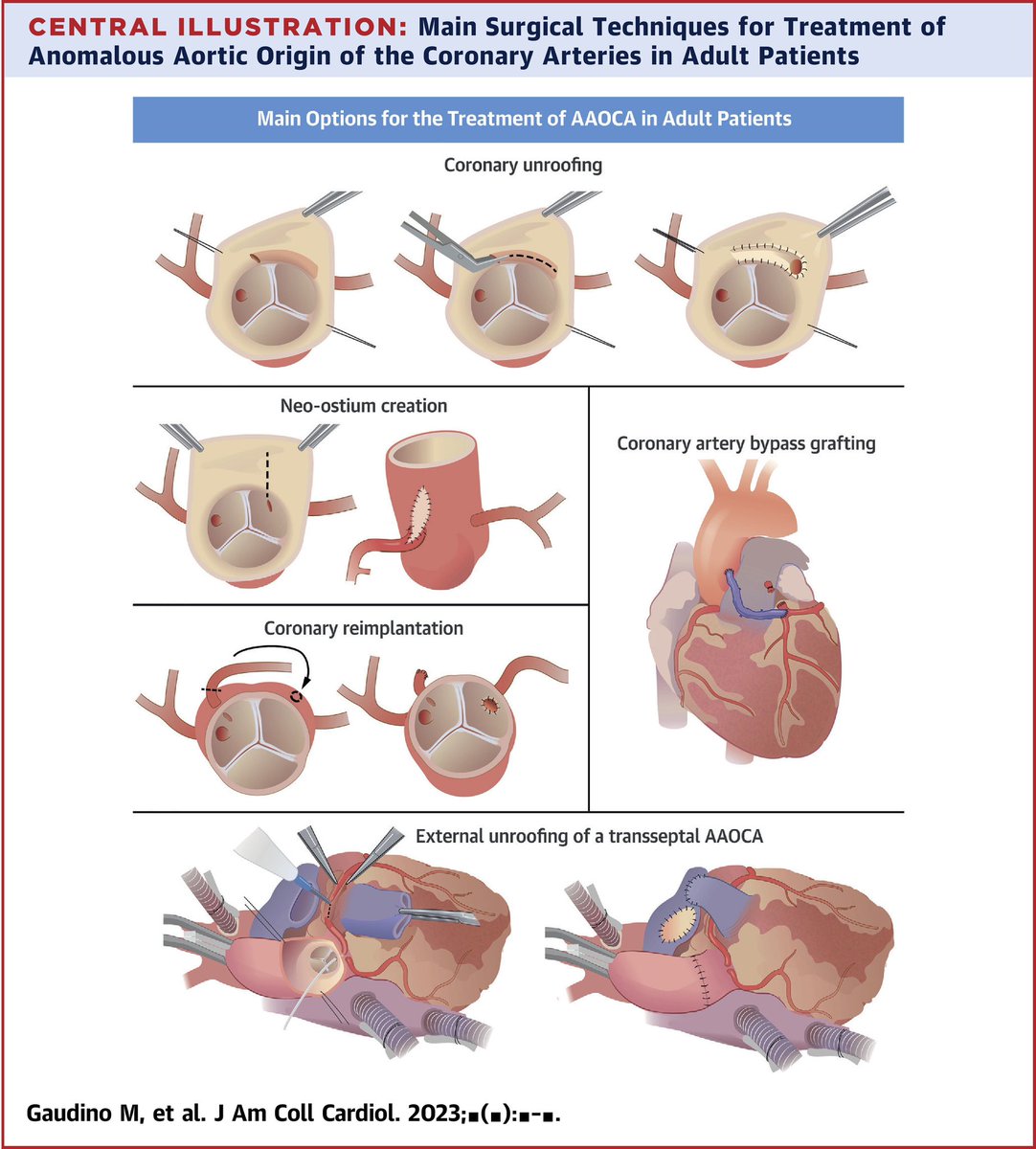
@JACCJournals Answer: Single coronary with anomalous LM arising from the RCA with a transseptal/subpulmonic course and a long intramyocardial segment.
Given recurrent CP, pt underwent external unroofing.
Avoid CABG alone in pts w/ good forward flow due to high likelihood of graft failure.


![IHSCardiac's tweet photo. 🫀 What a great case!
70-year-old woman with metastatic [withheld].
What’s the diagnosis? 🤔
Check out the full blog post: https://t.co/ESiwmtaseY
#Radres #Cardiology #RadTwitter #CardiacMRI #MedEd https://t.co/eNWPTBiBbV](https://pbs.twimg.com/media/HJxZLhYWgAAUrMR.png)
![IHSCardiac's tweet photo. 🫀 What a great case!
70-year-old woman with metastatic [withheld].
What’s the diagnosis? 🤔
Check out the full blog post: https://t.co/ESiwmtaseY
#Radres #Cardiology #RadTwitter #CardiacMRI #MedEd https://t.co/eNWPTBiBbV](https://pbs.twimg.com/media/HJxZLPiXEAASDgs.png)







































![IHSCardiac's tweet photo. 🫀 What a great case!
70-year-old woman with metastatic [withheld].
What’s the diagnosis? 🤔
Check out the full blog post: https://t.co/ESiwmtaseY
#Radres #Cardiology #RadTwitter #CardiacMRI #MedEd https://t.co/eNWPTBiBbV](https://pbs.twimg.com/media/HJxZL0BWsAAiqqK.png)