Radiation Oncologist at H. Clínic Barcelona.
Trained at ICO Badalona.
Graduado en Medicina en la UdL.
Barcelona-Valladolid-Castellón-Lleida-Oviedo-Phoenix
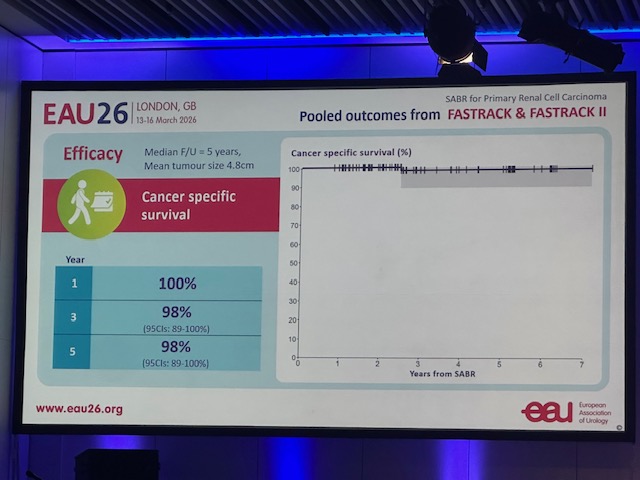
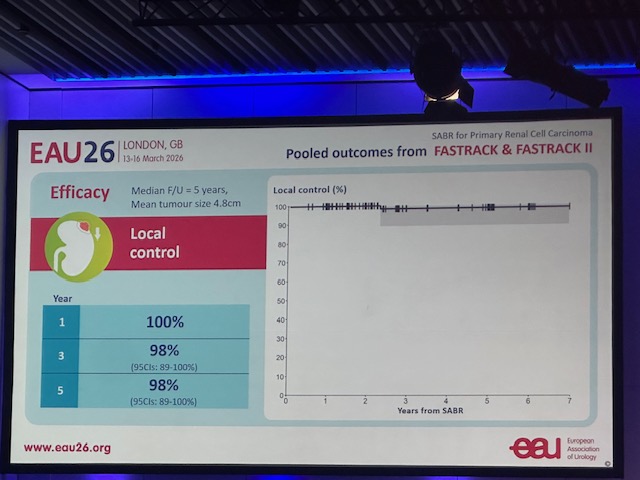
🎯 100% Local Control & 100% Cancer-Specific Survival. Long-term results of the FASTRACK II trial primary #kidneycancer.
✅ No local failures or cancer deaths
✅ Safe for high-risk/inoperable patients
✅ Kidney function preserved long-term
#ESTRO26#RadOnc#SABR@_ShankarSiva
#ESTRO26 - 📣 FASTRACKII final results, median F/U of 5 years. Thank you patients, funders, investigators - #kidneycancer#kcsm
1) 100% Local Control: No local recurrences were observed at 36, 60, or 84 months.
2) 100% Cancer-Specific Survival
3) Grade 3 AEs remain at 10%
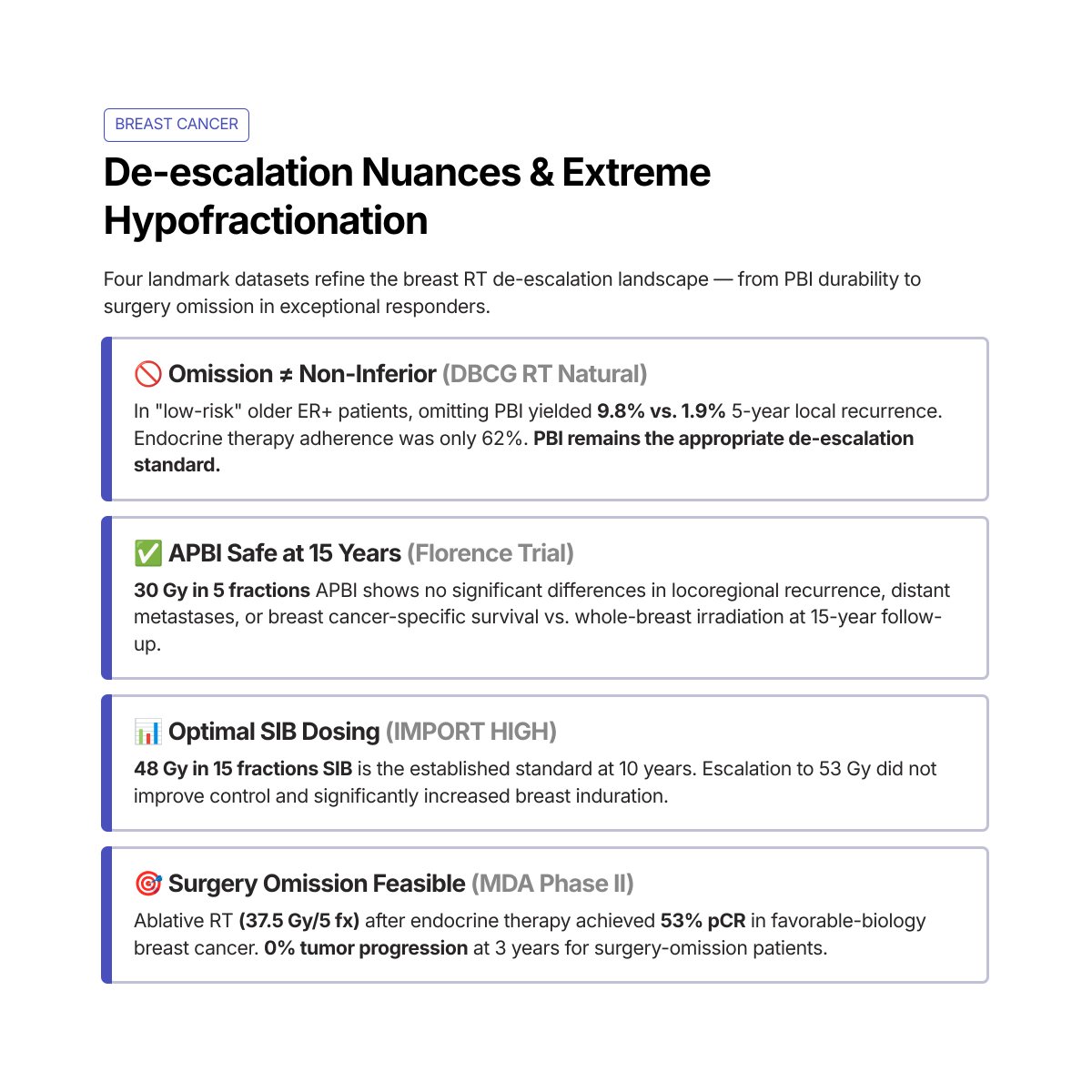
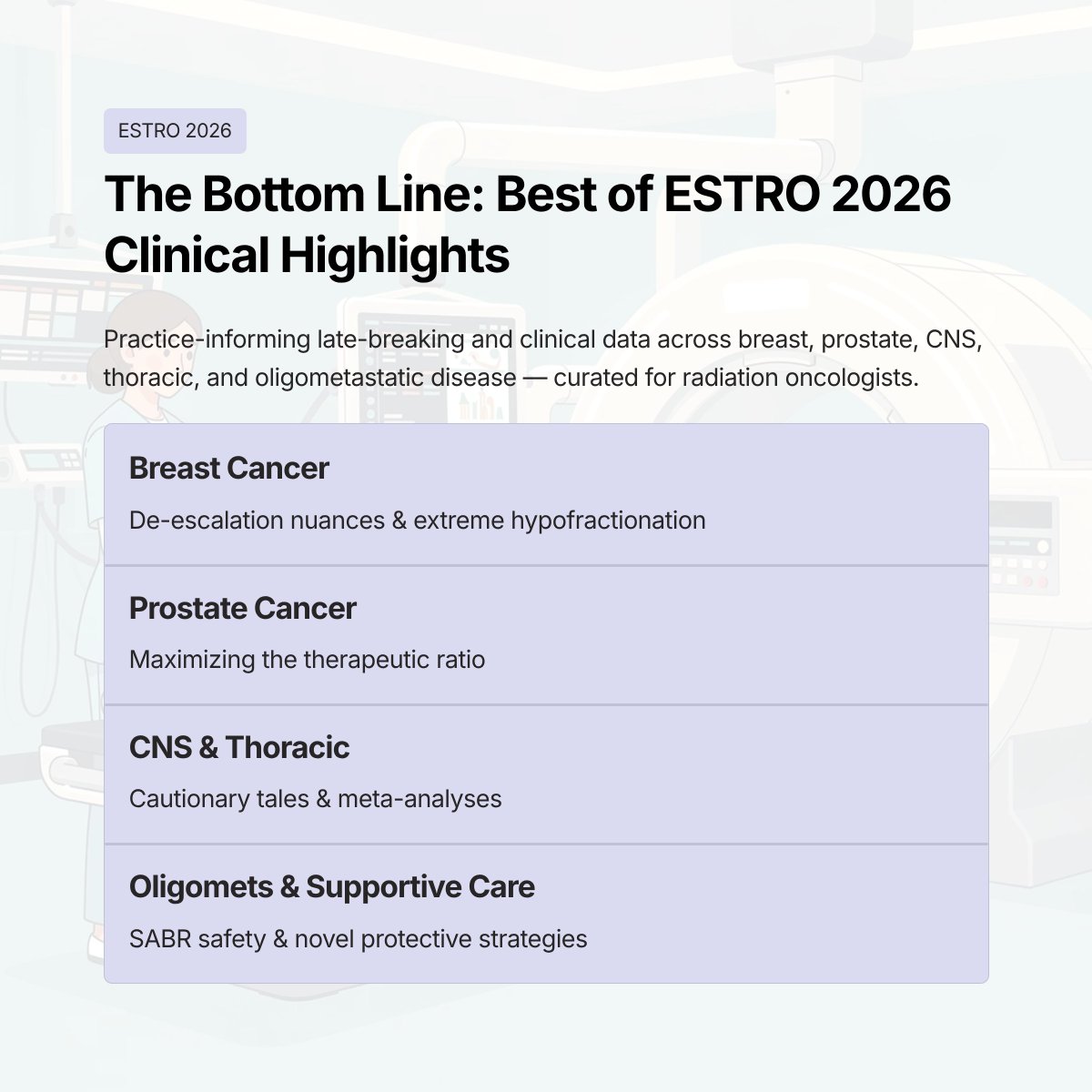
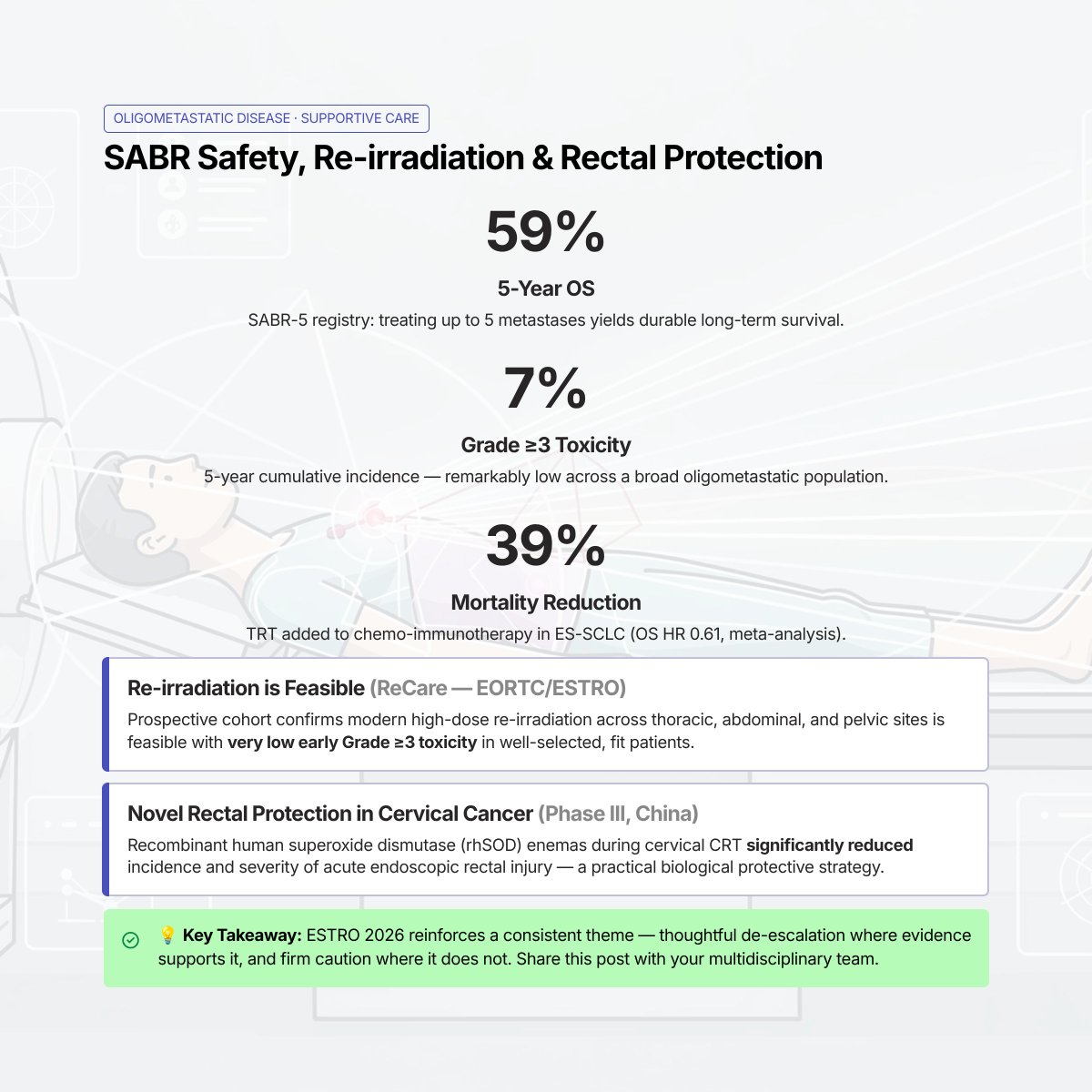
Our “Best of” #ESTRO26 outline is now live! 🚀
What key studies are we missing?
Drop any important trials, abstracts, or presentations we should add 👇
https://t.co/MyeQVhxxSk
#RadOnc#ESTRO26#ESTRO2026
Avui hem tancat quatre dies intensos d’auditoria del projecte #CATClinART EU4Health @hospitalclinic
Gràcies als auditors per la mirada experta i a l’equip OR per la implicació i l’esforç. Ha estat una experiència d’aprenentatge molt valuosa que ens ajuda a continuar millorant.
Here is Version 2.0 of when to hold systemic tx during RT. Updated & w 3 additional drug categories (ADCs, CDK4/6 inhibitors, PARPi).
More details on newer drugs in 🧵 below.
Please use this version as reference & thanks for all input/experience crowdsourcing! (1/3)
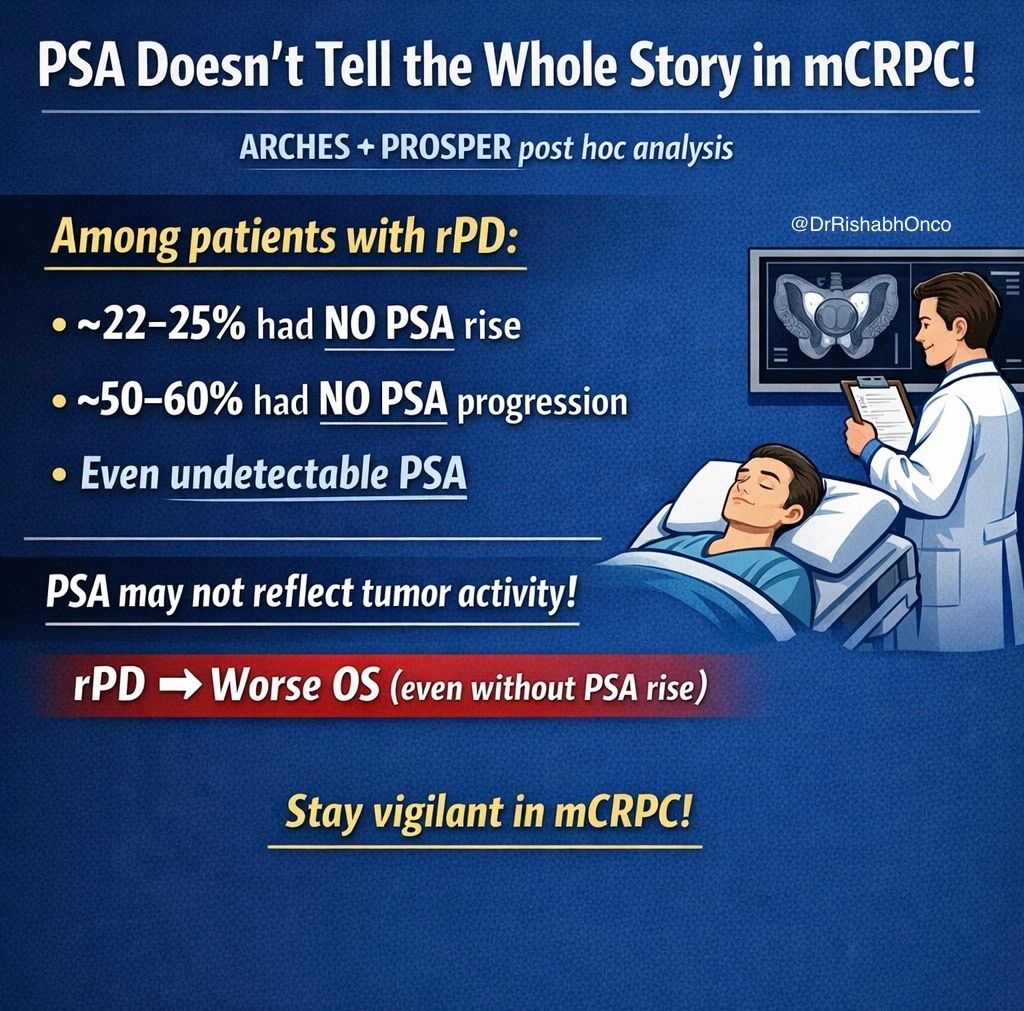
PSA is NOT enough. ⚠️
Radiographic progression can happen without PSA rise on enzalutamide.
New JCO analysis from ARCHES + PROSPER 👇
🧬 Study population
•mHSPC (ARCHES)
•nmCRPC (PROSPER)
•Enzalutamide ± ADT
•n = 2,551
💡 Key finding
➡️ PSA and imaging can be discordant
📊 What’s striking?
•~22–25% → rPD with no PSA rise
•~51–62% → no PSA progression despite rPD
•Even undetectable PSA at progression seen
📍 Liver mets more common with enzalutamide
⚠️ Prognosis
➡️ rPD = worse OS
➡️ Regardless of PSA behavior
🧠 Clinical implication
👉 PSA alone can MISS progression
👉 Imaging must NOT be delayed
📌 Practice-changing takeaway
➡️ Do periodic imaging even if PSA is stable
Because cancer doesn’t always follow PSA.
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #ProstateCancer #UroOnc
@oncoalert@asco
Fantastic news for renal cancer patients. Latest NICE guideline recommends #SABR to primary RCC for selected patients with stage IA and IB disease! https://t.co/e5HnkOwkww #radonc#medonc#SBRT
Big thanks to @_ShankarSiva who has pioneered this important treatment option
🚀 Largest prospective SABR cohort in inoperable RCC. Pooled FASTRACK trials show 98% local control at 5 years, excellent CSS, low ≥G3 toxicity and no late safety signals. A durable, non‑invasive, kidney‑sparing option—now poised for randomized comparison vs surgery. #EAU26
@jryckman3@DrSpratticus@safaviaa@US_FDA This is our work. It’s the published series with the longest follow up. Moderate hypofractionation seems complety safe, and actually the highest toxicity profile for now seems with normofractionation at longest FU
https://t.co/6WaXI1ucWN
🚨 New publication
🇪🇸 National SEOR-GI survey on Total Neoadjuvant Therapy (TNT) in locally advanced rectal cancer, now in Clinical and Translational Oncology.
👏 Congrats to Sigfredo Romero, coordinator of the SEOR GI Tumors Group.
🔗 https://t.co/NNyyYyBYyo
#RectalCancer
🔴El Dr. Mariano Barbacid y su equipo, financiados por #CRISContraelCáncer, han logrado curar el cáncer de páncreas en ratones, de forma duradera y sin efectos secundarios.
Pero necesitamos tu ayuda para que esto sea una realidad en pacientes.
DONA AQUÍ👉https://t.co/4VDU1PrRmA
Since the sudden PSA elevation didn’t make sense, we were concerned about a spurious PSA result which could be due to interfering heterophilic antibodies (https://t.co/3OBZb1uqgJ).
@Ruben_De_Groote@aleantonellibs1@RicBertolo Any idea of the denominator for the study, ie how many patients these 20 centres treated with radiotherapy over the preceding few years? That would help me understand the impact of this work.
💉 Liquid biopsy in #radiotherapy?
Tracking tumour #DNA in blood could let doctors adapt radiation therapy in real time — making treatment truly personalised.
👉 https://t.co/VHgyrMmknX
#biology
Valuable information from the NO-CUT Trial
-179 patients received induction TNT (4 cycles CAPOX-->LCCRT), 25 (14%) excluded during tx.
-----60% of these cancers were mid-rectal
-----18% were T4, and 54% were T2
-12 weeks later, restaging (n=154) showed cCR in 10.5%
-Pts with near-cCR were given another 4-5 weeks, then restaging found a cCR in an additional 20% (so 30.5% cCR overall).
-----T4 tumors had a 6% rate of cCR
-----N2 tumors had a 16% rate of cCR
-----Mid-rectal tumors had a 19% rate of cCR
-----Distal rectal tumors had a 36% rate of cCR
-The incomplete responders got TME, of which only 10 (8%) had pCR on final path.
----Of the 10 pCRs, 3 had recurrence (1 local, 1 distant, 1 both) which is high.
For watch-and-wait (n=47), regrowth occurred in 7 patients (15%), all of which had salvage TME, and 1 of which (14%) developed distant metastasis after this.
Tumor-agnostic ctDNA was drawn at baseline and then 11-17 weeks after TNT.
---95% of patients were ctDNA+ at baseline
---24% were ctDNA+ after TNT (8% of cCRs and 33% of incomplete responses)
Of the 3 patients with cCR despite being ctDNA+ after TNT, 1 had local recurrence, 1 had distant recurrence, and the 3rd transition to being ctDNA negative 5 weeks later and did well.
What does this mean (to the select few still reading)?
-With induction TNT, you have to be patient, as cCRs take more time (only 34% of cCRs present 12 weeks after TNT).
-Mid-rectal cancers may not be as responsive to TNT as distal cancers.
-When you include T4 and N2 patients in your protocol (excluded from some other studies), the cCR rate goes down, and the overall cohort does a bit worse.
-If the patient is ctDNA+ after TNT, even in the presence of a cCR, surgery is probably best, but this remains uncertain since the numbers are small.
https://t.co/gF9DtLacXH
New Evidence on ADT Duration in Prostate Cancer (JAMA Oncology, Nov 2025)
A meta-analysis of 10,266 patients shows a clear message.
Risk-based approach matters:
• 1 intermediate risk factor → 0 months
• ≥2 risk factors → ~6 months
• High-risk → ~12 months
• Very high-risk → individualize
This study challenges the old “longer is better” dogma and supports personalized ADT duration rather than fixed timelines.
🔗 https://t.co/Exlljkt77x
6/n
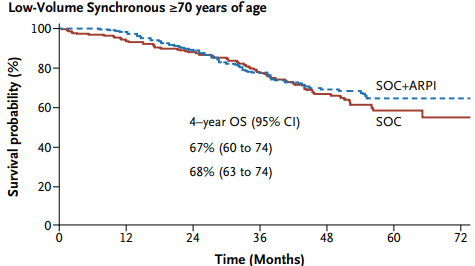
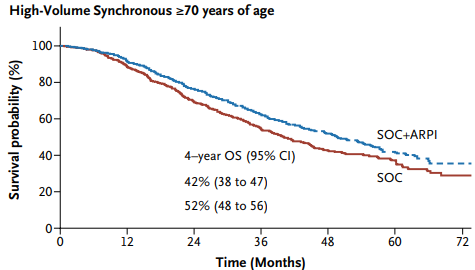
Importantly: low volume synchronous mHSPC defined by CONVENTIONAL imaging (not PSMA PET) the addition of ARPI to SOC did not improve OS in older men, with near identical 4 year OS.
However, high volume patients >70yo did derive benefit.