@MrMBB333
August 12, 2026.
Total solar eclipse at perigee-syzygy (magnitude 1.039).
Perseid maximum same night. 6-planet morning alignment.
Saturn-Neptune still within orb of 0° Aries conjunction.
Ascending lunar node at 0° Aries. Triple null crossing
— synodic, ecliptic, tropical — simultaneously.
Solar Cycle 25 at max. Recurrent coronal hole activity
predicted for the eclipse window based on 27-day solar
rotation. G4-G5 conditions possible. Magnetosphere
cumulatively stressed from repeated G4+ activity since
June.
D-layer collapses during totality. f₃ shifts from
20.8→21.0 Hz (measured: Pal 1999, Sátori 2016). With
concurrent CME influence: f₃ sweeps 20.0→21.5 Hz.
That's the Ca²⁺ cyclotron window (Liboff 1985). 100
Perseid meteors/hour create plasma channels in the
D-layer-collapsed ionosphere the same night.
Background state:
- AMOC at 1,600-year minimum (Science Advances, 2026)
- SAA at largest recorded extent, splitting into two lobes
- Earth rotation at reversal point (shortest days ever
recorded → now decelerating)
- Inner core "undergoing transformation" (Nature
Geoscience, Feb 2025)
- El Niño +6°C subsurface (IRI Columbia)
Every system you study is at an extreme value. On the
same day. With a total solar eclipse at perigee. And
Perseids hitting a collapsed ionosphere.
You cover all of these topics separately. Have you
looked at them together? On this specific date?
81 days.
@StefanBurnsGeo
August 12, 2026.
Total solar eclipse at perigee-syzygy (magnitude 1.039).
Perseid maximum same night. 6-planet morning alignment.
Saturn-Neptune still within orb of 0° Aries conjunction.
Ascending lunar node at 0° Aries. Triple null crossing
— synodic, ecliptic, tropical — simultaneously.
Solar Cycle 25 at max. Recurrent coronal hole activity
predicted for the eclipse window based on 27-day solar
rotation. G4-G5 conditions possible. Magnetosphere
cumulatively stressed from repeated G4+ activity since
June.
D-layer collapses during totality. f₃ shifts from
20.8→21.0 Hz (measured: Pal 1999, Sátori 2016). With
concurrent CME influence: f₃ sweeps 20.0→21.5 Hz.
That's the Ca²⁺ cyclotron window (Liboff 1985). 100
Perseid meteors/hour create plasma channels in the
D-layer-collapsed ionosphere the same night.
Background state:
- AMOC at 1,600-year minimum (Science Advances, 2026)
- SAA at largest recorded extent, splitting into two lobes
- Earth rotation at reversal point (shortest days ever
recorded → now decelerating)
- Inner core "undergoing transformation" (Nature
Geoscience, Feb 2025)
- El Niño +6°C subsurface (IRI Columbia)
Every system you study is at an extreme value. On the
same day. With a total solar eclipse at perigee. And
Perseids hitting a collapsed ionosphere.
You cover all of these topics separately. Have you
looked at them together? On this specific date?
81 days.
@realericmoutsos Well, he found the antichrist. The Antichrist Is a system, not a person. Only systems can rule the world.
We think like the system = mark on head
We work for the system = mark on hand
Words have been twisted & weaponised against White people.
Antiwhite propaganda is used to shame, guilt & silence White people to weaken us & control us.
Ignore the labels, share & speak your truth.
The Systemic Blind Spot of Medicine
1. Methodological Caution and Its Consequences
When research restricts itself to stating:
• “This is not proven”
• “This cannot be the cause”
• “This is just coincidence”
• “This is insufficient for causality”
this leads to the following consequences:
• Lack of initiation of new research projects
• Disregard of therapeutic successes
• Blocking of potential paths of discovery
• Loss of opportunities for affected individuals
This excessive caution represents a systemic blind spot in medicine.
The statement “We must not claim that it is causal” is often misunderstood as “Therefore, it is not relevant.”
As a result, severe structural effects arise:
• Research no longer focuses on the phenomenon.
• Funding is not provided.
• Physicians disregard the subject.
• Patients are not taken seriously.
• Successes fall out of the scientific spotlight.
⸻
2. Causes of Scientific Blockades
Scientific culture often reacts with restraint out of fear of:
• Oversimplified explanatory models
• Unsubstantiated promises of cures
• Stigmatization of patient groups
• Heterogeneity of clinical populations
• Misinterpretation by the media
• Possible assignment of blame
These fears lead to:
• Excessive caution
• Neutralization of innovative hypotheses
• Research-related passivity
This dynamic does not stem from malicious intent but represents a structural problem within science itself.
It hinders processes of knowledge formation and blocks the analysis of potential healing pathways.
The consequence:
Caution itself becomes the barrier.
The fear of false knowledge prevents the emergence of new knowledge.
⸻
Cause of ME/CFS – Systemic Pathophysiology
Complex diseases typically arise from dynamic systems, not from single isolated factors.
The Functional Cascade
Autonomic breathing dysfunction → Functional oxygen deficiency → Cellular malfunction → Chronic symptomatology
This model describes a logically coherent and systemically consistent chain of dysfunction, progressing from a clearly defined primary disturbance through several physiological mediators to cellular damage and chronicity.
⸻
3. The Trigger (Factor 1): Reprogramming of the Autonomic Nervous System (ANS)
3.1 Cause of Fixation (Initial Damage)
• The initial defect is triggered by chronic psychophysical stress or physical trauma (e.g., of the upper cervical spine).
• Mechanism: These triggers cause persistent irritation of brainstem regions that regulate unconscious breathing.
• Consequence: Flexible, deep diaphragmatic breathing is inhibited. The respiratory system becomes fixed in an inefficient, shallow thoracic breathing pattern.
3.2 Establishment of Dysautonomia
• Shallow, rapid breathing physiologically corresponds to an acute alarm state (“fight-or-flight” breathing).
• Sympathetic dominance: Autonomic regulation shifts permanently toward sympathetic overactivity.
• Vagal inhibition: The parasympathetic branch is actively suppressed, leading to dysregulation of heart rate, circulation, and restorative functions.
• Consequence: A manifest dysautonomia develops, characterized by POTS-like patterns with unstable heart rate and blood pressure regulation.
⸻
4. The Mediator (Factor 2): Functional Oxygen Deficiency
This section describes the transition from autonomic misregulation to cellular energy crises despite normal arterial oxygen saturation (SpO₂).
4.1 CO₂ Imbalance and O₂ Release (Bohr Effect)
• Chronically inefficient, shallow, or mildly hyperventilatory breathing patterns cause CO₂ loss (hypocapnia).
• Hypocapnia induces mild respiratory alkalosis.
• Bohr effect: In an alkaline environment, hemoglobin increases its oxygen-binding affinity, thereby reducing oxygen release to tissues (muscles, brain).
• Result: Functional cellular oxygen deficiency occurs despite normal SpO₂ levels.
4.2 Impaired Perfusion (Circulatory Mismatch)
• CO₂ deficiency causes vasoconstriction, particularly in cerebral vessels.
• Cerebral blood flow (CBF) drops significantly during orthostatic or cognitive load.
• Consequence: The so-called brain fog arises as a direct result of reduced cerebral perfusion.
⸻
5. The End Effect (Factor 3): Cellular Consequences
At the cellular level, functional oxygen deficiency leads to profound energetic dysregulation.
5.1 Forced Anaerobic Metabolism
• Muscle and nerve cells receive insufficient O₂ for mitochondrial aerobic ATP production.
• Even minor exertion forces a shift to anaerobic metabolism.
• Lactate evidence: Disproportionate lactate accumulation and delayed clearance are key pathological markers.
5.2 Secondary Mitochondrial Dysfunction and PEM
• Sustained anaerobic emergency operation structurally and functionally overloads mitochondria.
• ATP production drops significantly, leading to deep exhaustion.
• Post-Exertional Malaise (PEM): arises from the system’s inability to energetically compensate even minimal exertion.
• Recovery is delayed because ATP deficiency blocks restoration processes.
5.3 Chronic Inflammatory Reaction
• Energy stress and ATP deficit induce release of proinflammatory cytokines.
• Activated microglia cause secondary neuroinflammation.
• Consequences: Pain, malaise, amplification of cognitive impairment (“brain fog���), and perpetuation of dysregulation.
⸻
6. The Therapeutic Pathway Back: Resolution of the Cascade
6.1 Primary Therapeutic Conclusion
If Factor 1 (breathing fixation and ANS misprogramming) represents the starting point, then therapeutic intervention must begin there.
The goal is to restore autonomous breathing function, normalize CO₂ levels, and reactivate diaphragmatic breathing.
6.2 Reversal of the Pathophysiological Chain
• Application of targeted breathing therapies, e.g., biofeedback or CO₂ tolerance training.
• Restoration of normocapnia → dilation of cerebral vessels → increased CBF → improved cognitive function.
• Normalization of O₂ release → reduction of functional oxygen deficiency.
• Reduction of anaerobic pressure → decreased lactate production → mitochondrial relief.
• Stabilization of ATP production → reduced PEM sensitivity.
• Attenuation of inflammatory responses → reduction of neuroinflammatory processes.
• The overall system gradually exits the chronic alarm mode.
⸻
7. Conclusion
The presented model chain describes a plausible, systemically coherent dynamic of complex functional disorders.
The blockade of scientific engagement with such mechanisms represents less an epistemic problem and more a structural-cultural problem within medicine.
The fear of erroneous causal explanations prevents the necessary investigation of potentially relevant interconnections.
Knowledge is not protected by such caution — it is prevented.
#MECFS #LongCovid #PostViralSyndrome #ChronicFatigueSyndrome #Dysautonomia #POTS #Neuroinflammation #Mitochondria #BreathingDysfunction #AutonomicNervousSystem #VagusNerve #OxygenDysregulation #CO2Balance #BohrEffect #BrainFog #SystemicMedicine #MedicalResearch #ScientificBias #ParadigmShift #MedicalEpistemology #ComplexSystems #Pathophysiology #Biofeedback #FunctionalMedicine #IntegrativeMedicine #SomaticIntelligence #ScienceCulture #MedicalBlindSpot #KnowledgeBarrier #ResearchReform
The Systemic Blind Spot of Medicine
1. Methodological Caution and Its Consequences
When research restricts itself to stating:
• “This is not proven”
• “This cannot be the cause”
• “This is just coincidence”
• “This is insufficient for causality”
this leads to the following consequences:
• Lack of initiation of new research projects
• Disregard of therapeutic successes
• Blocking of potential paths of discovery
• Loss of opportunities for affected individuals
This excessive caution represents a systemic blind spot in medicine.
The statement “We must not claim that it is causal” is often misunderstood as “Therefore, it is not relevant.”
As a result, severe structural effects arise:
• Research no longer focuses on the phenomenon.
• Funding is not provided.
• Physicians disregard the subject.
• Patients are not taken seriously.
• Successes fall out of the scientific spotlight.
⸻
2. Causes of Scientific Blockades
Scientific culture often reacts with restraint out of fear of:
• Oversimplified explanatory models
• Unsubstantiated promises of cures
• Stigmatization of patient groups
• Heterogeneity of clinical populations
• Misinterpretation by the media
• Possible assignment of blame
These fears lead to:
• Excessive caution
• Neutralization of innovative hypotheses
• Research-related passivity
This dynamic does not stem from malicious intent but represents a structural problem within science itself.
It hinders processes of knowledge formation and blocks the analysis of potential healing pathways.
The consequence:
Caution itself becomes the barrier.
The fear of false knowledge prevents the emergence of new knowledge.
⸻
Cause of ME/CFS – Systemic Pathophysiology
Complex diseases typically arise from dynamic systems, not from single isolated factors.
The Functional Cascade
Autonomic breathing dysfunction → Functional oxygen deficiency → Cellular malfunction → Chronic symptomatology
This model describes a logically coherent and systemically consistent chain of dysfunction, progressing from a clearly defined primary disturbance through several physiological mediators to cellular damage and chronicity.
⸻
3. The Trigger (Factor 1): Reprogramming of the Autonomic Nervous System (ANS)
3.1 Cause of Fixation (Initial Damage)
• The initial defect is triggered by chronic psychophysical stress or physical trauma (e.g., of the upper cervical spine).
• Mechanism: These triggers cause persistent irritation of brainstem regions that regulate unconscious breathing.
• Consequence: Flexible, deep diaphragmatic breathing is inhibited. The respiratory system becomes fixed in an inefficient, shallow thoracic breathing pattern.
3.2 Establishment of Dysautonomia
• Shallow, rapid breathing physiologically corresponds to an acute alarm state (“fight-or-flight” breathing).
• Sympathetic dominance: Autonomic regulation shifts permanently toward sympathetic overactivity.
• Vagal inhibition: The parasympathetic branch is actively suppressed, leading to dysregulation of heart rate, circulation, and restorative functions.
• Consequence: A manifest dysautonomia develops, characterized by POTS-like patterns with unstable heart rate and blood pressure regulation.
⸻
4. The Mediator (Factor 2): Functional Oxygen Deficiency
This section describes the transition from autonomic misregulation to cellular energy crises despite normal arterial oxygen saturation (SpO₂).
4.1 CO₂ Imbalance and O₂ Release (Bohr Effect)
• Chronically inefficient, shallow, or mildly hyperventilatory breathing patterns cause CO₂ loss (hypocapnia).
• Hypocapnia induces mild respiratory alkalosis.
• Bohr effect: In an alkaline environment, hemoglobin increases its oxygen-binding affinity, thereby reducing oxygen release to tissues (muscles, brain).
• Result: Functional cellular oxygen deficiency occurs despite normal SpO₂ levels.
4.2 Impaired Perfusion (Circulatory Mismatch)
• CO₂ deficiency causes vasoconstriction, particularly in cerebral vessels.
• Cerebral blood flow (CBF) drops significantly during orthostatic or cognitive load.
• Consequence: The so-called brain fog arises as a direct result of reduced cerebral perfusion.
⸻
5. The End Effect (Factor 3): Cellular Consequences
At the cellular level, functional oxygen deficiency leads to profound energetic dysregulation.
5.1 Forced Anaerobic Metabolism
• Muscle and nerve cells receive insufficient O₂ for mitochondrial aerobic ATP production.
• Even minor exertion forces a shift to anaerobic metabolism.
• Lactate evidence: Disproportionate lactate accumulation and delayed clearance are key pathological markers.
5.2 Secondary Mitochondrial Dysfunction and PEM
• Sustained anaerobic emergency operation structurally and functionally overloads mitochondria.
• ATP production drops significantly, leading to deep exhaustion.
• Post-Exertional Malaise (PEM): arises from the system’s inability to energetically compensate even minimal exertion.
• Recovery is delayed because ATP deficiency blocks restoration processes.
5.3 Chronic Inflammatory Reaction
• Energy stress and ATP deficit induce release of proinflammatory cytokines.
• Activated microglia cause secondary neuroinflammation.
• Consequences: Pain, malaise, amplification of cognitive impairment (“brain fog”), and perpetuation of dysregulation.
⸻
6. The Therapeutic Pathway Back: Resolution of the Cascade
6.1 Primary Therapeutic Conclusion
If Factor 1 (breathing fixation and ANS misprogramming) represents the starting point, then therapeutic intervention must begin there.
The goal is to restore autonomous breathing function, normalize CO₂ levels, and reactivate diaphragmatic breathing.
6.2 Reversal of the Pathophysiological Chain
• Application of targeted breathing therapies, e.g., biofeedback or CO₂ tolerance training.
• Restoration of normocapnia → dilation of cerebral vessels → increased CBF → improved cognitive function.
• Normalization of O₂ release → reduction of functional oxygen deficiency.
• Reduction of anaerobic pressure → decreased lactate production → mitochondrial relief.
• Stabilization of ATP production → reduced PEM sensitivity.
• Attenuation of inflammatory responses → reduction of neuroinflammatory processes.
• The overall system gradually exits the chronic alarm mode.
⸻
7. Conclusion
The presented model chain describes a plausible, systemically coherent dynamic of complex functional disorders.
The blockade of scientific engagement with such mechanisms represents less an epistemic problem and more a structural-cultural problem within medicine.
The fear of erroneous causal explanations prevents the necessary investigation of potentially relevant interconnections.
Knowledge is not protected by such caution — it is prevented.
#MECFS #LongCovid #PostViralSyndrome #ChronicFatigueSyndrome #Dysautonomia #POTS #Neuroinflammation #Mitochondria #BreathingDysfunction #AutonomicNervousSystem #VagusNerve #OxygenDysregulation #CO2Balance #BohrEffect #BrainFog #SystemicMedicine #MedicalResearch #ScientificBias #ParadigmShift #MedicalEpistemology #ComplexSystems #Pathophysiology #Biofeedback #FunctionalMedicine #IntegrativeMedicine #SomaticIntelligence #ScienceCulture #MedicalBlindSpot #KnowledgeBarrier #ResearchReform
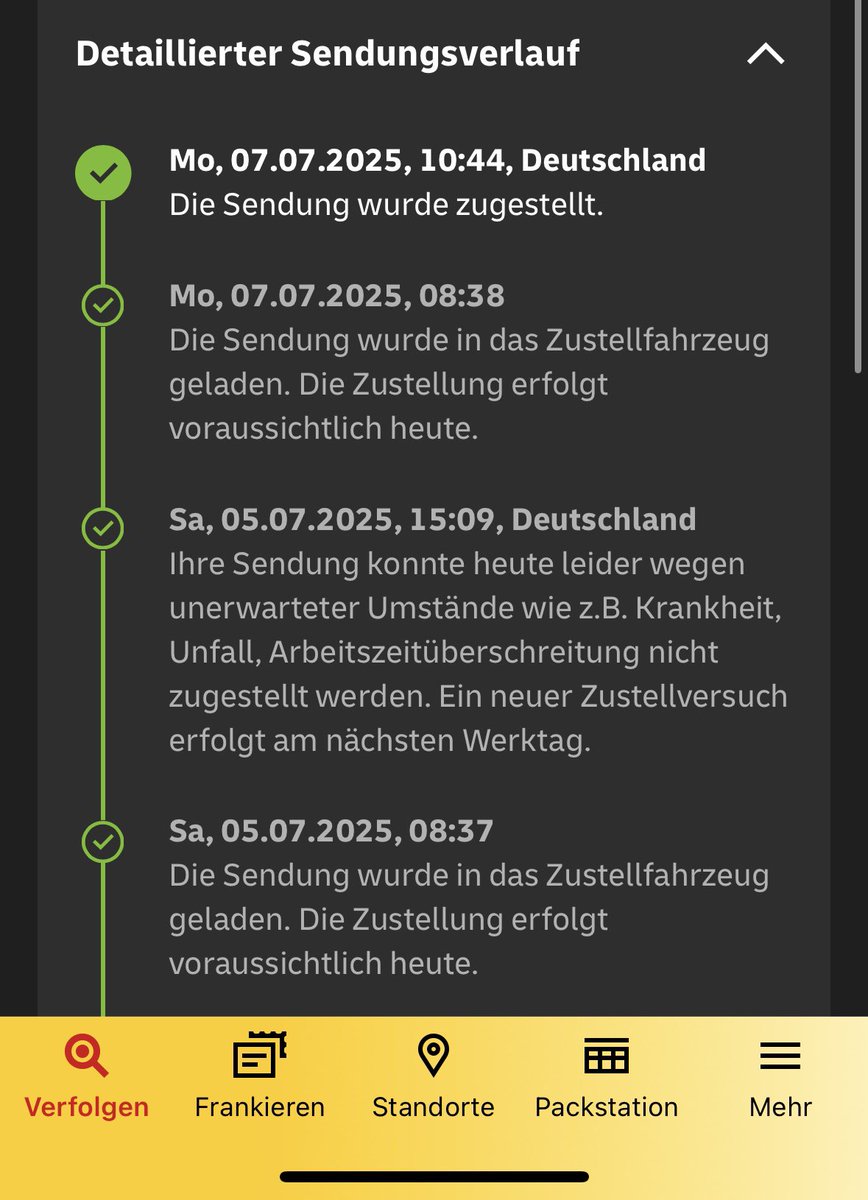
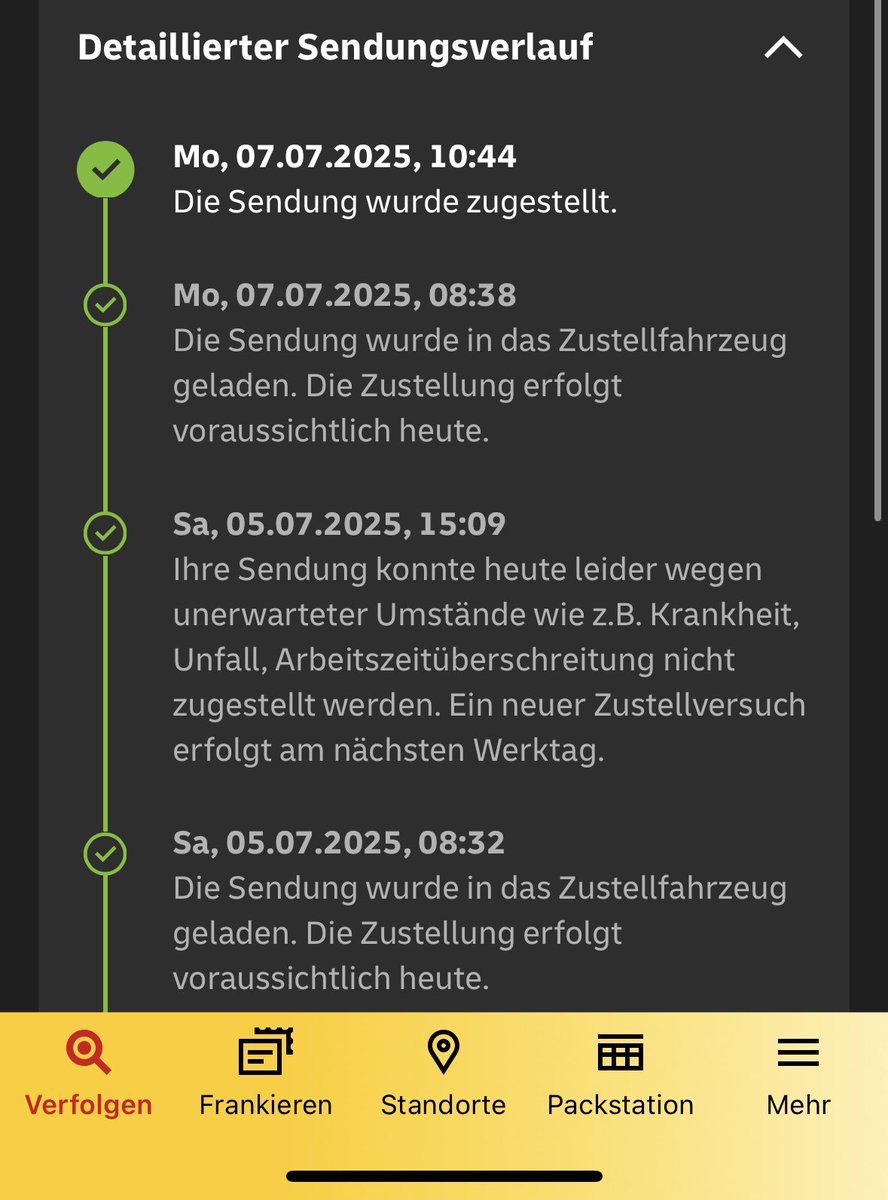
@DHLPaket Ich beobachte seit Monaten in Osterholz-Scharmbeck, dass die Live-Verfolgung meiner Pakete immer nach wenigen Minuten deaktiviert wird – obwohl sie später doch ankommen. In Bremen war das nie so. Ist das ein bekanntes Problem im Depot OHZ?