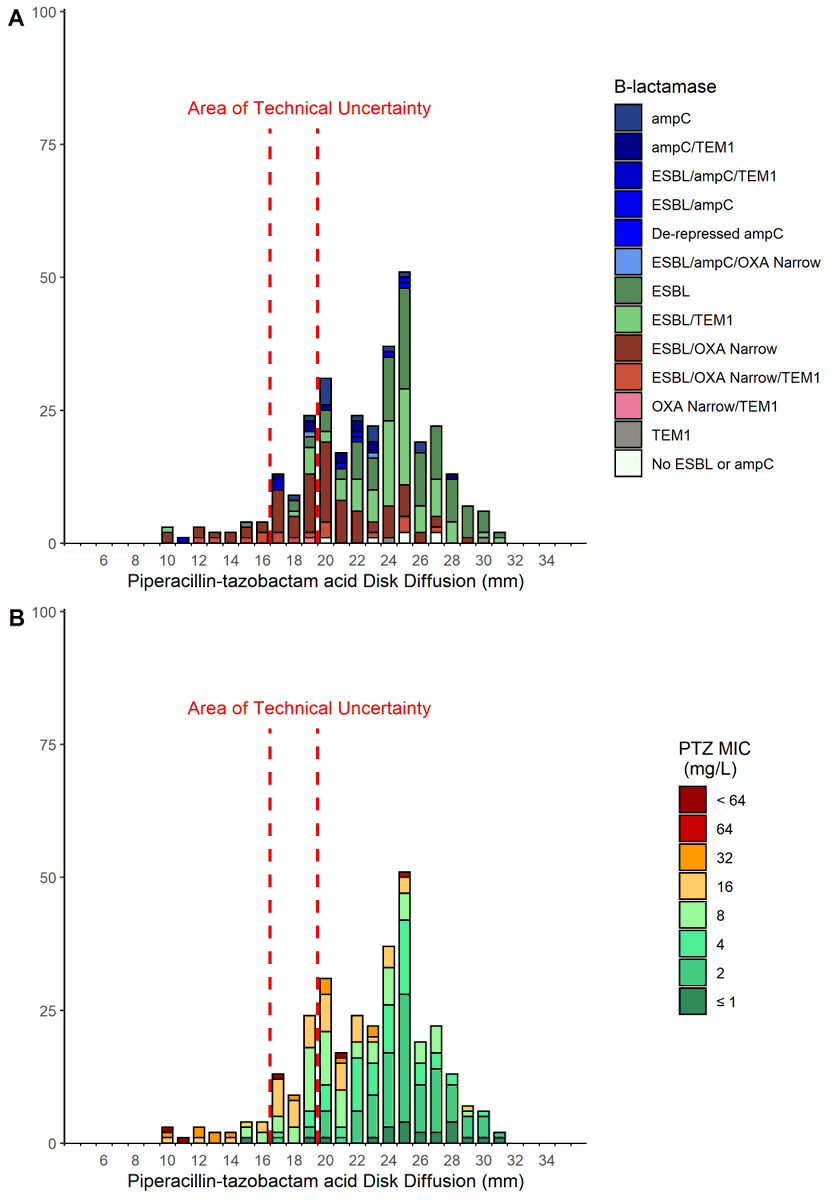
@DrToddLee@padstamundo@draghafur@davidantibiotic@MerinoTrial Interesting thought! Here is the PTZ zone diameter distribution stratified by MIC for isolates with VITEK MIC <16mg/L. I can do the same plot stratified by BL gene present, but almost all the 16mg/L and 32mg/L have OXA1 present.
@DrToddLee@padstamundo@draghafur@davidantibiotic@MerinoTrial pip/taz disk alone is probably enough and ignore the vitek, though the new Etest is probably better. Alternative: If susc by PTZ disk, CDDST confirms ESBL and amox/clav disk is susc, then sens and spec of 91.6% and 64.5% to exclude oxa strains
@DrToddLee@padstamundo@draghafur@davidantibiotic@MerinoTrial The main issue relates to the co-presence of OXA1 genes with ESBLs and the inability to differentiate the two using any phenotypic test. Reducing the susceptible breakpoint to <= 8mg/L as proposed by EUCAST does solve some issues, but still splits the OXA1/ESBL population.
Association between minimum inhibitory concentration, beta-lactamase genes and mortality for patients treated with piperacillin/tazobactam or meropenem from the MERINO study https://t.co/L8dBdmKU2z
Nice work @Hendonet@padstamundo@davidantibiotic
This paper from @Hendonet @UQMedicine helps further our understanding of the @MerinoTrial - bottom line, MIC matters but so does the way you test and the #AMR genes that define the phenotype
Exciting webinar from @UQ_News & @CHUNimes on new advances in #antimicrobial susceptibility testing and reporting...stellar panel of Profs Turnidge, Lavigne & Kahlmeter. Thanks to @CRE_REDUCE @Hendonet @padstamundo hosted at #UQCCR
Out in CID - Association between minimum inhibitory concentration, beta-lactamase genes and mortality for patients treated with piperacillin/tazobactam or meropenem from the MERINO study @merinotrial@padstamundo https://t.co/yqX3cfcXr6
Join Jason Roberts, Andrew Henderson, Jean-Philippe Lavigne, Gunnar Kahlmeter & John Turnidge for a webinar on antimicrobial susceptibility testing & hear from experts on the European Committee on AST (EUCAST). Please register here https://t.co/I1Spr6Io0b
@DrToddLee@padstamundo@davidantibiotic@Hugh_Murray_ @syctong @Josh_S_Davis We also only looked at vitek S strains, but I think that is the question that clinicians are most interested in: if the vitek calls it susceptible, can the lab exclude penicillinase in order to confidently treat the patient with benzylpenicillin.
@DrToddLee@padstamundo@davidantibiotic@Hugh_Murray_ @syctong @Josh_S_Davis We are sequencing all blaZ detected strains. There seemed to be two phenotypic distinct populations - disk size < 26 indicating an expressed penicillinase enzyme (perhaps slowly induced) and those with size > 26 in the WT distribution that might only express a basal amount.
@DrToddLee@padstamundo@davidantibiotic@Hugh_Murray_ @syctong @Josh_S_Davis Prevalence of penicillin susceptible by vitek in our region is about 12-14% depending on specimen site. Nitrocefin and disk testing seemed to perform equally for different vitek MICs but numbers start to get low when you stratify by this.
@DrToddLee@padstamundo@davidantibiotic@Hugh_Murray_ @syctong @Josh_S_Davis All good points and lots of questions!
First thing - I have never seen a published case of penicillin failure for PSSA due to mis-identification of penicillin resistance. Several other drug-bug combos have as many issues with false susceptibility (if not more)