🆕 NUEVO en "García Fernández te pone al día"
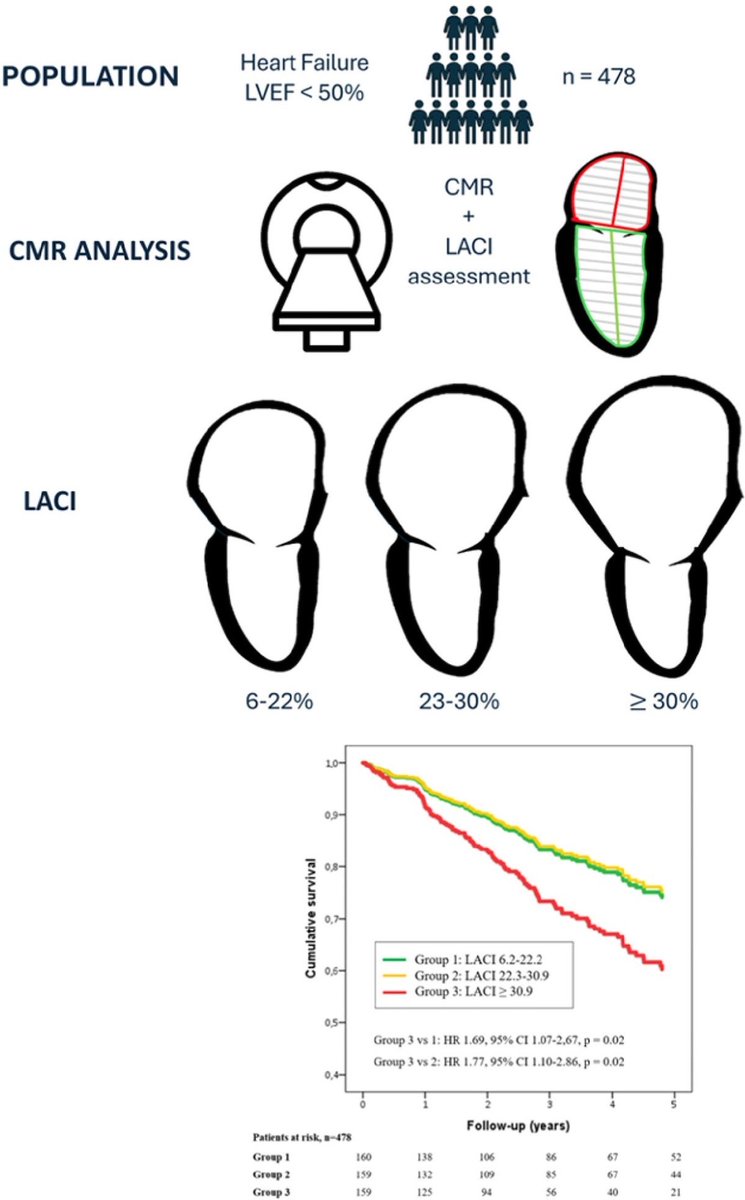
La función auricular analizada por acortamiento longitudinal, mejora la estratificación del riesgo en la posible miocarditis
👓 https://t.co/0XDpe1rO8v ◀️
El trabajo se plantea si la función auricular, medida por resonancia cardíaca mediante el acortamiento longitudinal de la aurícula, aporta valor pronóstico en pacientes con sospecha de miocarditis
#CardioNugget™
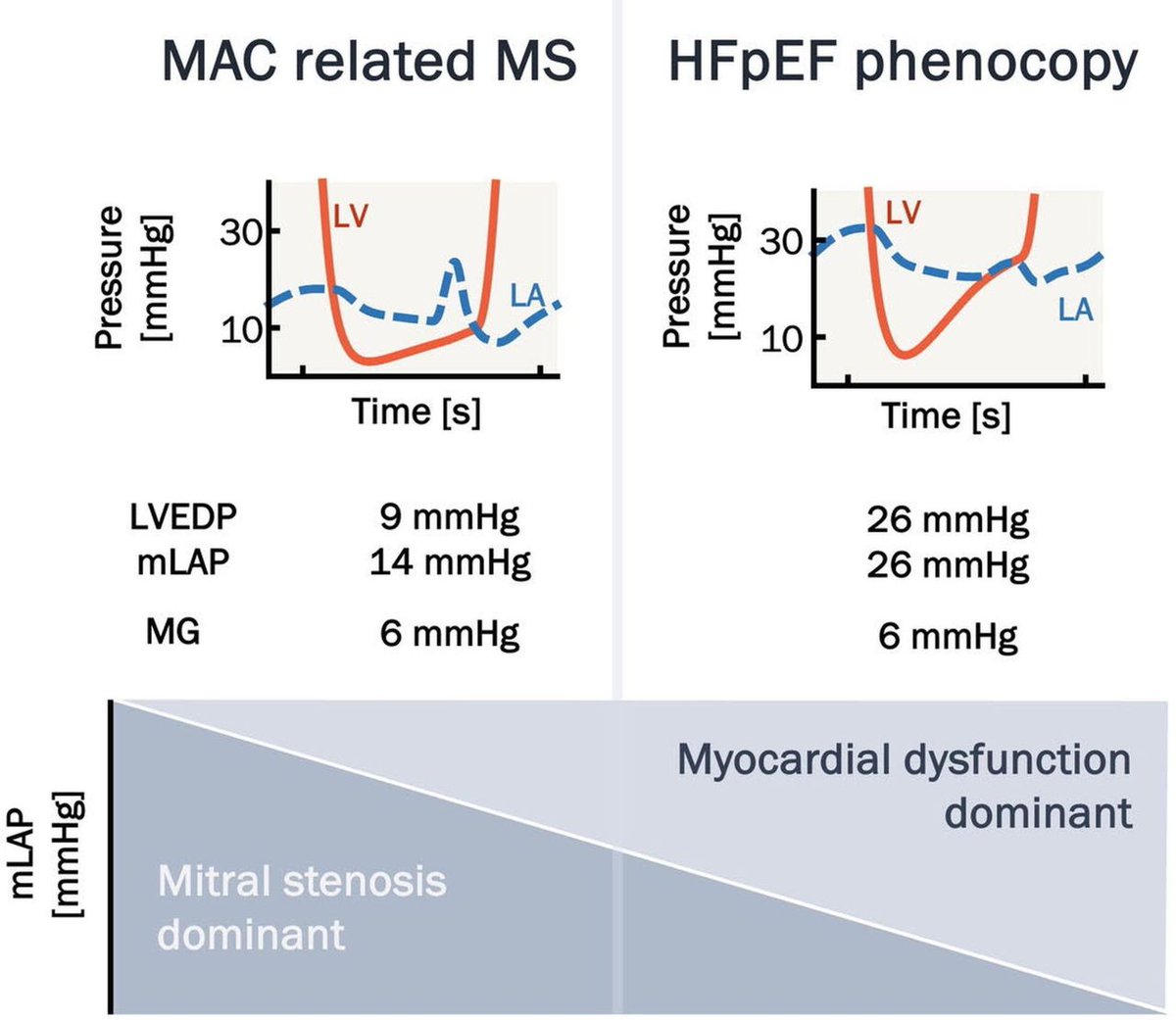
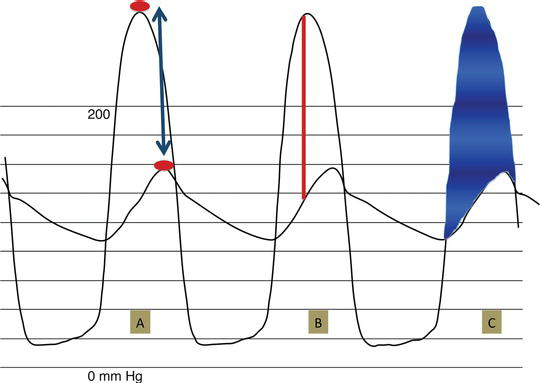
Cath gradients in AS are not all the same:
Peak-to-peak gradient
Peak LV systolic pressure − peak aortic systolic pressure
The peaks occur at different times → not a true instantaneous gradient
BUT clinically, the peak-to-peak gradient often approximates the mean transaortic gradient.
Peak instantaneous gradient
Closest equivalent to Doppler peak gradient
Mean gradient
The shaded area
Average of all instantaneous LV–Ao gradients during systole
Clinical pearl:
-Echo/cath mean gradients are most clinically useful
-Peak-to-peak gradient should not be used interchangeably with Doppler peak gradient
#CardioNuggets #MedEd #CardioMed #CardioMed #EchoFirst #AorticStenosis #MeanGradient
🚦FFR-Positive, Ischemia-Negative: The Elephant in the Room
For years, we have been told that after an abnormal CCTA, functional testing helps identify the lesions that “really matter.”
This large individual patient-data meta-analysis challenges that assumption.
Among patients with ≥50% stenosis on CCTA:
✅ Functional imaging identified anatomically severe CAD reasonably well (81% sensitivity).
❌ But for lesions with FFR ≤0.80, sensitivity dropped to only 64% overall.
In other words:
A substantial proportion of FFR-positive lesions do NOT produce detectable ischemia on stress imaging.
This raises an uncomfortable question:
If a lesion is FFR-positive but does not generate measurable ischemia, what exactly are we measuring?
A pressure gradient?
A biological disease process?
Or a surrogate endpoint that only partially overlaps with clinically relevant myocardial ischemia?
The study also showed that the most advanced imaging techniques (PET and high-field CMR) were more sensitive, while more traditional approaches were more specific. Yet even the best modalities failed to identify all FFR-positive lesions.
The broader implication
Perhaps the problem is not that functional imaging is insufficient.
Perhaps the problem is the expectation that:
FFR-positive = ischemic = clinically relevant
These concepts are related.
They are not synonymous.
As cardiac imaging continues to evolve, the future may lie less in choosing between anatomy and physiology and more in integrating:
👉 plaque burden
👉 plaque phenotype
👉 myocardial consequences
👉 symptoms
👉 physiology
into a unified disease model.
Because coronary artery disease is more complex than a pressure wire value.
#CardiacCT #CCTA #FFR #PET #CMR #CoronaryArteryDisease #PrecisionMedicine #PreventiveCardiology #CardiovascularImaging
Answer Revealed! 🫀 — May 26 CMR Case
This patient has Libman-Sacks endocarditis from systemic lupus erythematosus. There are both non-ischemic and ischemic myocardial injury present.
👉 Read the full case here: https://t.co/7ukkaGliTd
#WhyCMR#SCMRCases
Eco🫀: Índice de Acoplamiento AuriculoVentricular izquierdo [LACI].
📊 El LACI es un parámetro ecocardiográfico que integra la relación funcional entre la aurícula izquierda y el ventrículo izquierdo en un solo índice. A diferencia de parámetros aislados como el LAVI o el E/e’, el LACI evalúa simultáneamente ambos compartimentos y su interacción mecánica durante la diástole.
🧮Fórmula = (Vol. TeleDiastólico de AI / Vol. TeleDiastólico del VI) x 100
����️Fisiopatológicamente, en la IC-FEVI preservada, el VI desarrolla alteración de la relajación y aumento de rigidez miocárdica. Esto incrementa las presiones de llenado, generando dilatación progresiva de la aurícula izquierda mientras el volumen ventricular permanece relativamente conservado. El resultado es un aumento del LACI, reflejando un desacoplamiento auriculoventricular. 🫀💢
🔷️En un estudio publicado en Scientific Reports 2025, los valores de LACI fueron significativamente mayores en IC-FEVIp (~59%) comparado con IC-FEVIr (~41%) y controles sanos (~13%). Un punto de corte >33% identificó IC-FEVIp con una S: 97% y E: 87%. 🧐🎯
🔷️Además de su utilidad diagnóstica en IC-FEVIp, el LACI se ha relacionado con riesgo de FA, severidad de disfunción diastólica, hospitalización por ICA y eventos CV adversos post-IAM, posicionándose como un biomarcador emergente de interacción auriculoventricular. 🔎❤️🩹
📄🆓️⤵️
DOI: 10.1161/JAHA.125.041392
https://t.co/TCbNlcenCf
https://t.co/ZvUEDdQlly
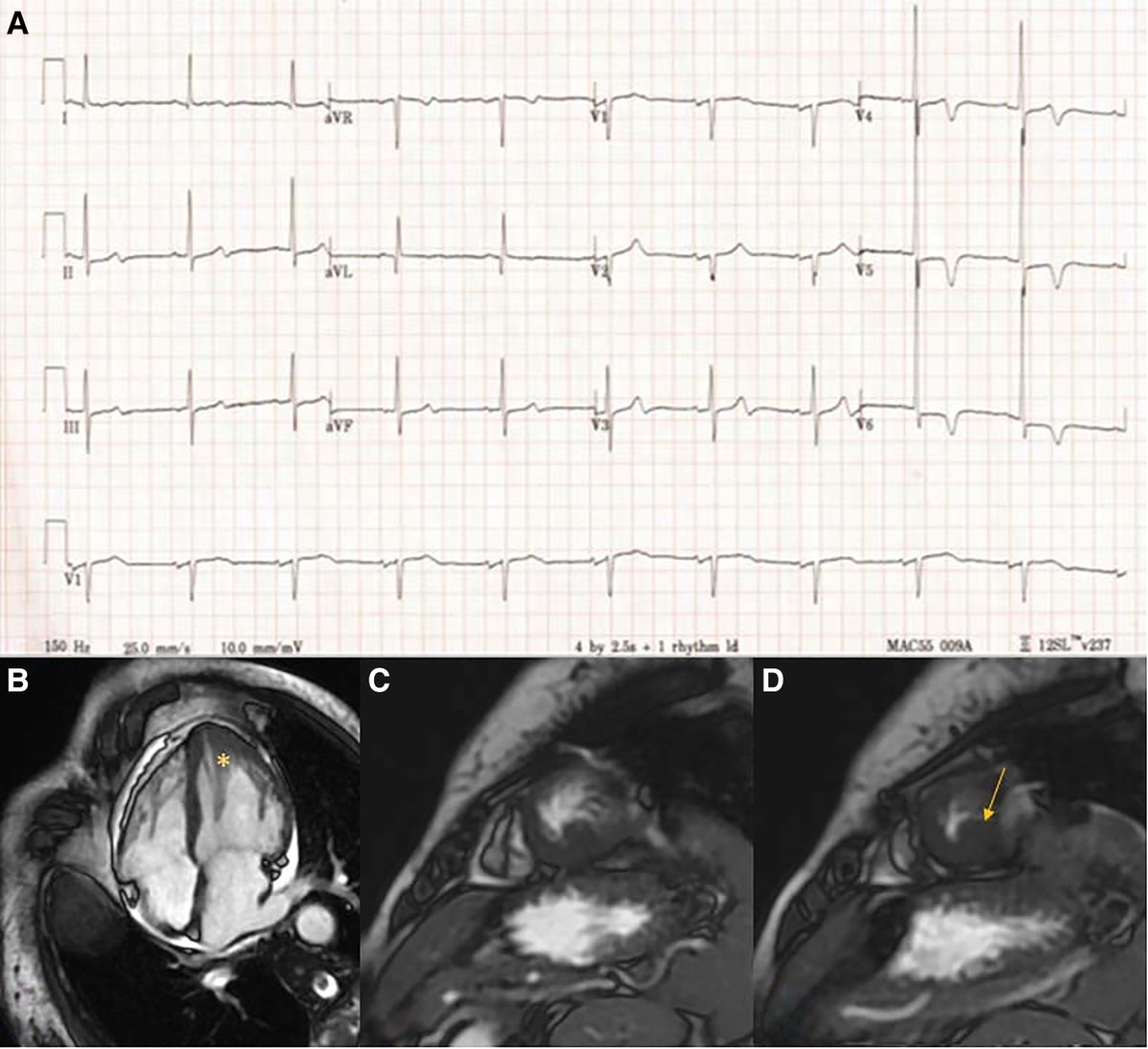
New CMR Case Drop! 🫀
A 32-year-old female with rheumatoid arthritis presented with fatigue and dyspnea 5 weeks after starting a biologic (eosinophilic count was 80% the differential).
🔍 What led to improvement on the follow-up CMR?
👇 Drop your answer below!
Answer Revealed! 🫀 — May 5 CMR Case
This is an example of a sinus of Valsalva rupture into the right atrium, creating a left-to-right shunt as well as aortic insufficiency.
👉 Read the full case here: https://t.co/BlelcP4LT1
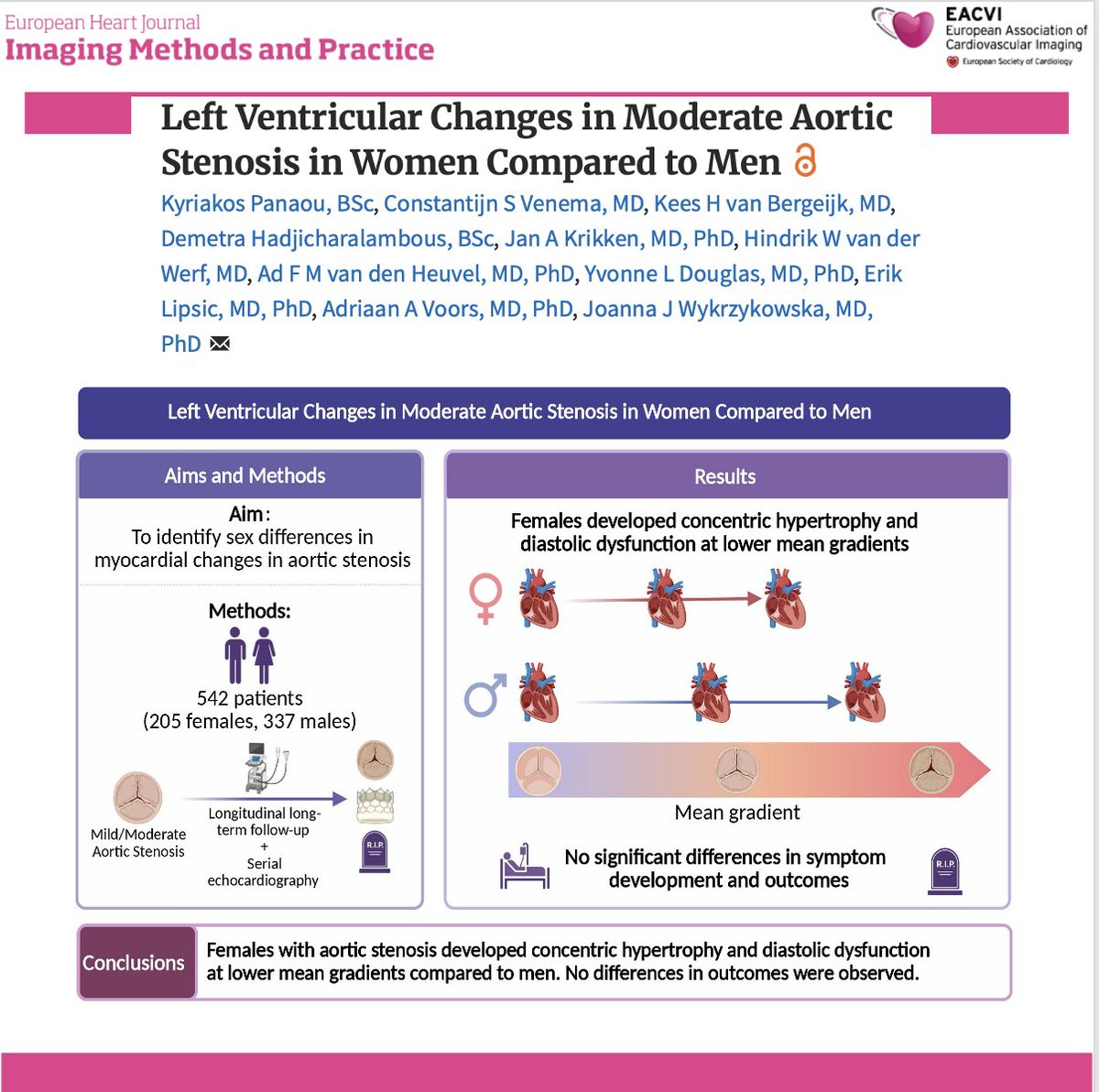
📄 Sex differences in moderate aortic stenosis: new longitudinal insights
🔗 https://t.co/ZuPlMei8wf
🫀 A longitudinal study of >500 patients with moderate aortic stenosis highlights important sex-specific differences in left ventricular remodeling.
✨ Key findings:
🔹 Women develop concentric hypertrophy and diastolic dysfunction at lower transvalvular gradients
🔹 They exhibit more pronounced diastolic dysfunction throughout follow-up
🔹 Dyspnoea is more common at presentation
🔹 Despite this, no differences in outcomes were observed:
➡️ symptom onset timing
➡️ aortic valve replacement
➡️ mortality
📊 These findings suggest greater sensitivity of the female myocardium to pressure overload, even at earlier stages of disease
💡 Clinical take-home message:
👉 Sex-specific differences emerge early (moderate AS stage)
👉 This may support:
closer surveillance in women
more tailored management strategies
rethinking timing of intervention
🚺 Aortic stenosis is not the same disease in women and men:
the pathophysiology differs—even when outcomes appear similar.
#Cardiology #AorticStenosis #Echocardiography #SexDifferences #WomenInCardiology #HeartValveDisease #CardiacRemodeling #HFpEF #TAVR #PrecisionMedicine 🫀📊
You can have a relatively preserved LV… and still be high arrhythmic risk
📊 In this cohort:
• NDLVC patients had:
→ smaller LV volumes
→ better NYHA class
→ similar LGE burden
BUT
• 17% developed sustained VA
• 10% HF hospitalization
1-s2.0-S000291492500760X-main
➡️ Not benign. Not low-risk.
🧠 What really drives risk? (not what you expect)
❌ Not LVEF
❌ Not LGE (presence alone)
✅ Instead:
• PVC burden >1000/24h → massive risk (OR ~20)
• RVEF ≤45% → strong predictor
• QTc prolongation → independent signal
1-s2.0-S000291492500760X-main
🔥 Translation:
👉 The disease is electrical + right ventricular,
not just structural LV
⚠️ This is the uncomfortable part:
We are still using
👉 LVEF thresholds
👉 DCM-based models
…for a disease where they don’t work well
🧬 Think arrhythmogenic spectrum
NDLVC overlaps with:
• arrhythmogenic cardiomyopathy
• early DCM
• LV-dominant disease
➡️ It’s not a stage.
➡️ It’s a phenotype with its own biology
🎯 Clinical take-home
When you see a “non-dilated” LV:
Don’t relax.
Look at:
▪️ PVC burden
▪️ RV function
▪️ QTc
👉 That’s where the risk is hiding
💬 Are we under-treating these patients because the LV looks “too good”?
#Cardiology #CMR #Arrhythmia
#NDLVC #DCM #HeartFailure
#EPeeps #CardioTwitter 🫀
https://t.co/0FNJf9NzvP
Major bleeding after left atrial appendage occlusion was most frequent in the first 6 months, and associated with older age, diabetes, prior bleeding, kidney disease, and increased risk of stroke and mortality.
https://t.co/9mfkKI8HyO
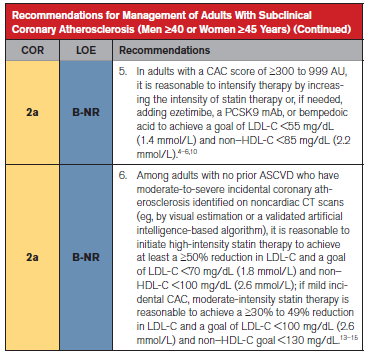
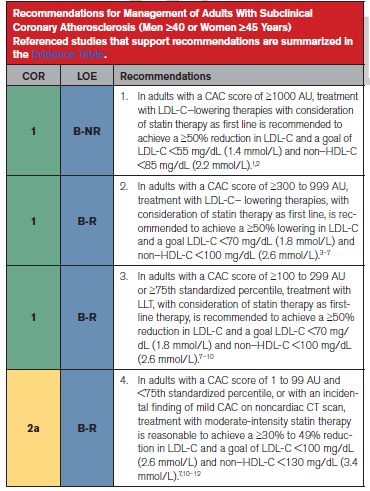
9/ 🫀 El calcio coronario gana protagonismo
El score de calcio se convierte en una herramienta clave para decidir tratamiento.
Escenarios:
🔴 ≥1000 AU
➡️ Reducir LDL ≥50%
🎯 Objetivo: <55 mg/dL
🟠 300–999 AU
➡️ Reducir LDL ≥50%
🎯 Objetivo: <70 mg/dL
⬇️ Intensificación razonable hasta <55 mg/dL
🟡 100–299 AU (o ≥ percentil 75)
➡️ Reducir LDL ≥50%
🎯 Objetivo: <70 mg/dL
🟢 1–99 AU (y < percentil 75)
💊 Estatinas de intensidad moderada
🎯 Objetivo: LDL <100 mg/dL
🫀An Expert Overview of Durability of M-TEER via #JACCIntervention
✅️ M-TEER durability up to 5 y remains understudied.
✅️ M-TEER failure 📈 af 3 y | primary MR > than secondary MR.
✅️ MR recurrence rates are relatively high after redo M-TEER.
https://t.co/rLTrlgIk4J
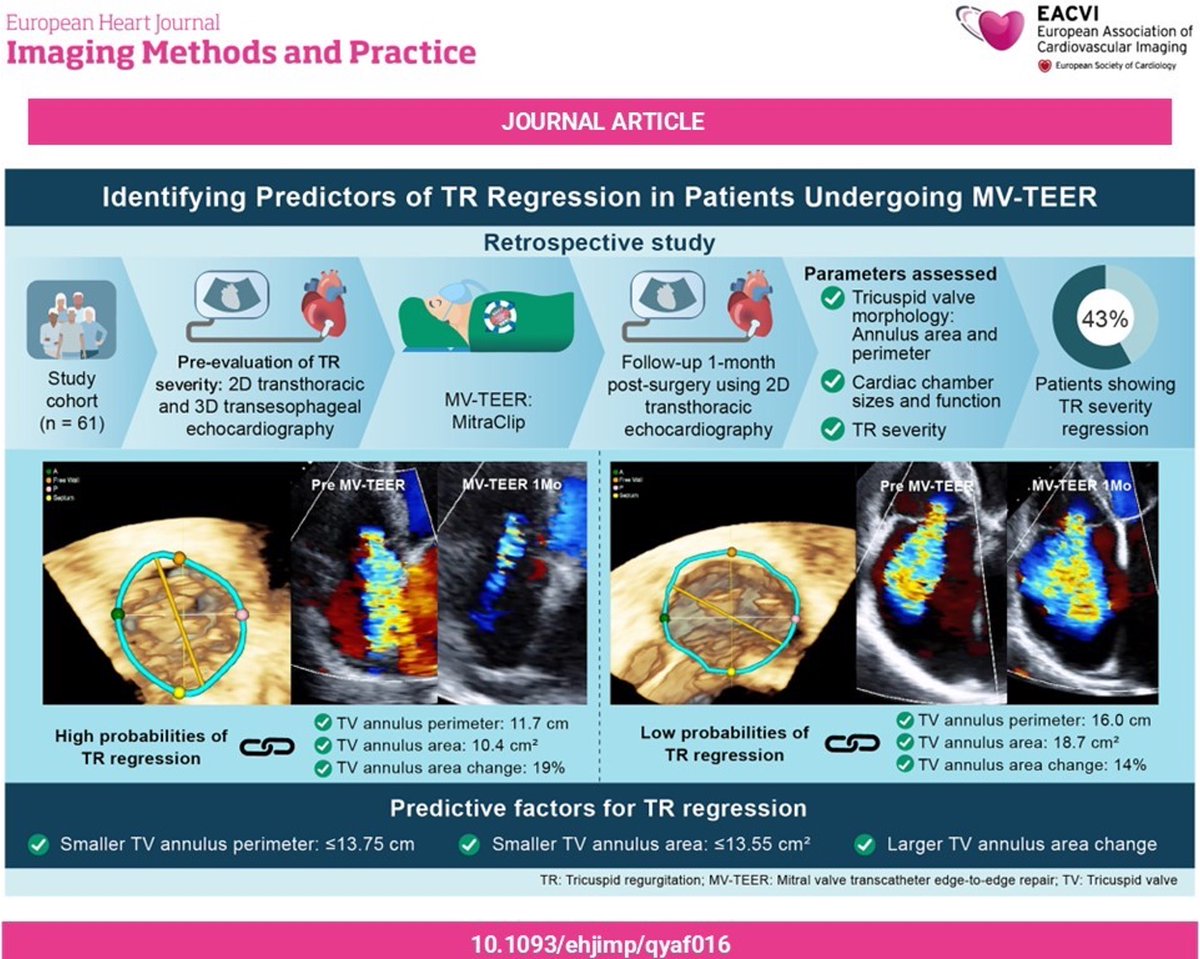
#EHJIMP 🫀 TR regression after M-TEER 💡
Tricuspid valve annulus perimeter was the strongest predictor of TR regression in this study including 61 patients who underwent pre+post 3D #echofirst. Annulus area and area change also predicted TR⬇️.
Read more: https://t.co/edhekXmcKk
Valor pronóstico del índice de acoplamiento auriculo-ventricular izquierdo en la insuficiencia cardíaca
👓 https://t.co/nVVwGHLm9S ◀️
Si en una CMR de IC con FEVI <50% encontramos una AI muy aumentada para un VI no tan dilatado, el IAAV ayuda a poner número a esa impresión clínica y a considerarlo una bandera roja de riesgo (junto a LGE, función, congestión y comorbilidad), más que un dato aislado de tamaño
En "García Fernández te pone al día"








![javier20ch's tweet photo. Eco🫀: Índice de Acoplamiento AuriculoVentricular izquierdo [LACI].
📊 El LACI es un parámetro ecocardiográfico que integra la relación funcional entre la aurícula izquierda y el ventrículo izquierdo en un solo índice. A diferencia de parámetros aislados como el LAVI o el E/e’, el LACI evalúa simultáneamente ambos compartimentos y su interacción mecánica durante la diástole.
🧮Fórmula = (Vol. TeleDiastólico de AI / Vol. TeleDiastólico del VI) x 100
����️Fisiopatológicamente, en la IC-FEVI preservada, el VI desarrolla alteración de la relajación y aumento de rigidez miocárdica. Esto incrementa las presiones de llenado, generando dilatación progresiva de la aurícula izquierda mientras el volumen ventricular permanece relativamente conservado. El resultado es un aumento del LACI, reflejando un desacoplamiento auriculoventricular. 🫀💢
🔷️En un estudio publicado en Scientific Reports 2025, los valores de LACI fueron significativamente mayores en IC-FEVIp (~59%) comparado con IC-FEVIr (~41%) y controles sanos (~13%). Un punto de corte >33% identificó IC-FEVIp con una S: 97% y E: 87%. 🧐🎯
🔷️Además de su utilidad diagnóstica en IC-FEVIp, el LACI se ha relacionado con riesgo de FA, severidad de disfunción diastólica, hospitalización por ICA y eventos CV adversos post-IAM, posicionándose como un biomarcador emergente de interacción auriculoventricular. 🔎❤️🩹
📄🆓️⤵️
DOI: 10.1161/JAHA.125.041392
https://t.co/TCbNlcenCf
https://t.co/ZvUEDdQlly](https://pbs.twimg.com/media/HJSEol4XYAAvb-z.jpg)

















![javier20ch's tweet photo. Eco🫀: Índice de Acoplamiento AuriculoVentricular izquierdo [LACI].
📊 El LACI es un parámetro ecocardiográfico que integra la relación funcional entre la aurícula izquierda y el ventrículo izquierdo en un solo índice. A diferencia de parámetros aislados como el LAVI o el E/e’, el LACI evalúa simultáneamente ambos compartimentos y su interacción mecánica durante la diástole.
🧮Fórmula = (Vol. TeleDiastólico de AI / Vol. TeleDiastólico del VI) x 100
����️Fisiopatológicamente, en la IC-FEVI preservada, el VI desarrolla alteración de la relajación y aumento de rigidez miocárdica. Esto incrementa las presiones de llenado, generando dilatación progresiva de la aurícula izquierda mientras el volumen ventricular permanece relativamente conservado. El resultado es un aumento del LACI, reflejando un desacoplamiento auriculoventricular. 🫀💢
🔷️En un estudio publicado en Scientific Reports 2025, los valores de LACI fueron significativamente mayores en IC-FEVIp (~59%) comparado con IC-FEVIr (~41%) y controles sanos (~13%). Un punto de corte >33% identificó IC-FEVIp con una S: 97% y E: 87%. 🧐🎯
🔷️Además de su utilidad diagnóstica en IC-FEVIp, el LACI se ha relacionado con riesgo de FA, severidad de disfunción diastólica, hospitalización por ICA y eventos CV adversos post-IAM, posicionándose como un biomarcador emergente de interacción auriculoventricular. 🔎❤️🩹
📄🆓️⤵️
DOI: 10.1161/JAHA.125.041392
https://t.co/TCbNlcenCf
https://t.co/ZvUEDdQlly](https://pbs.twimg.com/media/HJSEonpXgAA_aRd.jpg)