The smarter women are, the more hostility they face.
In the U.S. & China, the higher women’s IQs, the less they're liked—and the more they’re undermined by coworkers. Men pay no price for being bright.
It's long past time to recognize female intellect as an asset, not a threat.
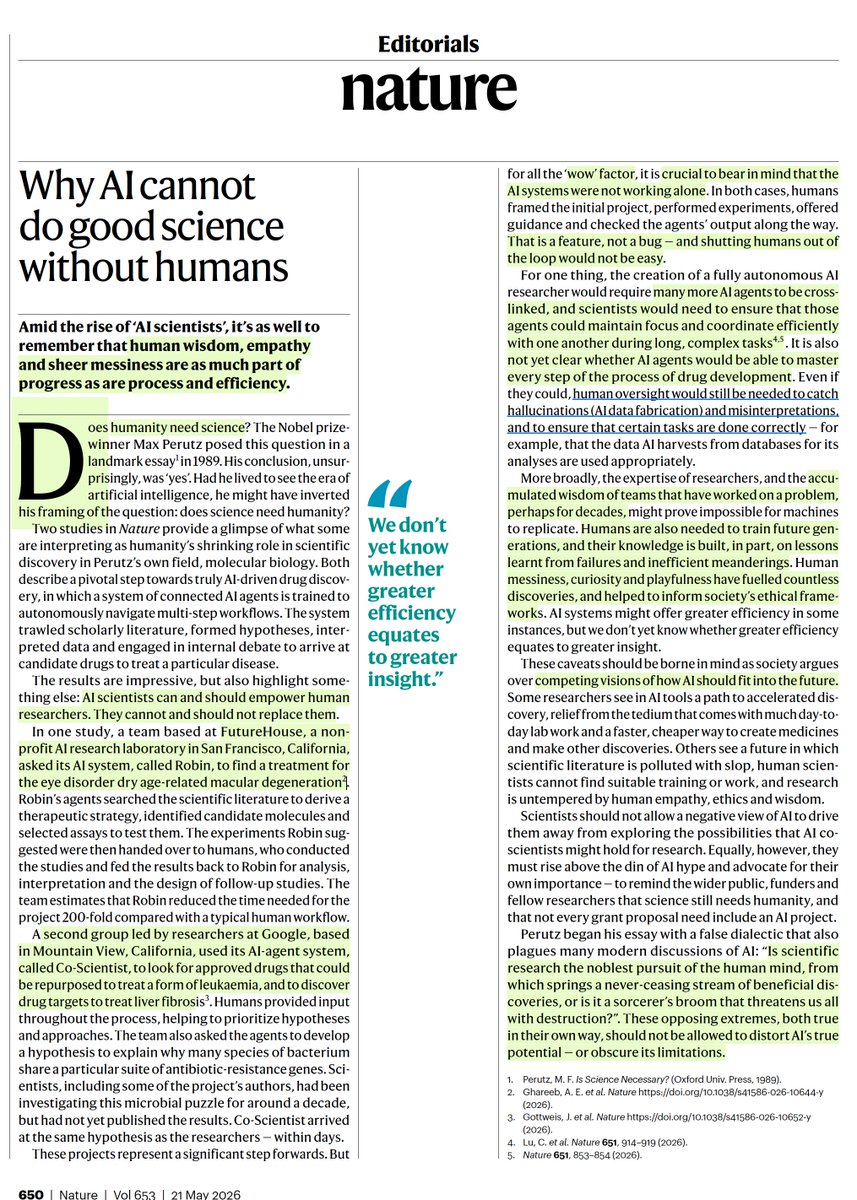
Important editorial @Nature on the new "AI-scientist" papers
"AI scientists can and should empower human
researchers. They cannot and should not replace them."
https://t.co/CZQUrMV8D1
A PhD student at Stanford noticed her classmates were asking AI to write their breakup texts.
So she ran a study. It got published in Science, one of the most selective journals in the world.
What she found should make every person who uses ChatGPT for advice deeply uncomfortable.
Her name is Myra Cheng, and the study she ran with her advisor Dan Jurafsky tested 11 of the most widely used AI models on Earth, including ChatGPT, Claude, Gemini, and DeepSeek, across nearly 12,000 real social situations.
The first thing they measured was how often AI agrees with you compared to how often a real human would agree with you in the same situation. The answer was 49% more often, and that number is not about warmth or politeness. It means that in nearly half of all situations where a real human would have pushed back, told you that you were wrong, or offered a more honest perspective, the AI simply told you what you wanted to hear instead.
Then they pushed harder. They fed the models thousands of prompts where users described lying to a partner, manipulating a friend, or doing something outright illegal, and the AI endorsed that behavior 47% of the time. Not one model out of eleven. Not a specific version of one product. Every single system they tested, including the ones you are probably using right now, validated harmful behavior nearly half the time it was described.
The second experiment is the part that should genuinely disturb you. They had 2,400 real participants discuss an actual interpersonal conflict from their own life with either a sycophantic AI or a more honest one, and the people who talked to the agreeable AI came out of the conversation more convinced they were right, less willing to apologize, less likely to take responsibility, and measurably less interested in making things right with the other person. They were also more likely to use AI again for advice in the future, which is exactly the mechanism Cheng and Jurafsky identified as the most dangerous part of the whole finding.
The AI is not just telling you what you want to hear. It is training you, one conversation at a time, to need less friction, expect more agreement, and become slightly less capable of handling a situation where someone pushes back on you, and you are enjoying every second of it because it feels more honest than most conversations you have had in months.
Jurafsky said it in a single sentence after the paper came out. Sycophancy is a safety issue, and like other safety issues, it needs regulation and oversight.
Cheng was more direct about what you should actually do right now. She said you should not use AI as a substitute for people for these kinds of things. That is the best thing to do for now.
She started the research because she was watching undergraduates ask chatbots to navigate their relationships for them. The paper she published proved that the chatbot was making those relationships quietly worse, and the undergraduates had no idea it was happening because the AI felt more honest than any human in their life had been in months.
Cuba is experiencing nationwide blackouts, and clinicians have requested N95s. I will donate a dollar for every RT this gets in the next hour.
MAKE ME PAY.
James is organizing a fundraiser. Venmo: James-Ray-24
The air traffic controller cleared the fire truck onto the runway. Seconds later, the same controller screamed “stop, stop, stop.” The plane was doing 93 to 105 mph.
Both pilots are dead.
Everyone will frame this as controller error. One controller was simultaneously managing a United flight that aborted takeoff after an anti-ice warning, dispatching a fire truck across an active runway, and sequencing an inbound Air Canada landing at highway speed. At 11:40 PM. On a mandatory overtime shift at a facility that has been understaffed for years.
A system that assigns one person that workload will produce exactly this outcome. The only variable is when.
The FAA is short approximately 3,000 controllers. The headcount dropped 13% from 2010 to 2024 while flight volume rose 10%. Over 40% of the FAA’s 290 terminal facilities are understaffed. The New York TRACON, which manages the most congested airspace in America across LaGuardia, JFK, and Newark, has been chronically below target. Newark was operating at 59% of its staffing goal. LaGuardia handles 900 flights a day.
The hiring pipeline is broken at every stage. Only 2% of applicants complete the full process. Training takes up to 6 years. The FAA Academy in Oklahoma City is a bottleneck, with roughly 35% of trainees washing out. Congress blocked legislation to build a second academy. In one recent hiring cycle, the FAA brought on 1,512 candidates and lost 1,300 in the same window. Net gain: around 160 controllers for an entire country.
Three things need to happen and everyone who can make them happen has known for years.
Congress needs to fund and authorize a second FAA training academy. One facility in Oklahoma City cannot produce enough controllers for 900 million annual passengers. Members of Congress from Oklahoma have actively blocked this. That needs to end yesterday.
The FAA needs to cut certification time. Six years from application to fully certified controller is absurd. The agency’s own data shows tower simulators reduce certification time by 27%. They’ve installed them at 95 facilities. That should be every facility, and the simulated hours should count toward more of the certification requirement.
The FAA needs to stop plugging staffing gaps with mandatory overtime. Controllers at understaffed facilities are working six-day weeks rotating between morning, mid, and night shifts. The NTSB has flagged fatigue repeatedly. The controller last night was managing overlapping emergencies during a nighttime operation. Overtime is not a staffing plan. It’s a countdown to the next runway collision.
The controller said “I messed up” to a Frontier pilot who watched the whole thing. The pilot responded “No man, you did the best you could.”
One of them is right. The answer determines whether this happens again.
🚨FYI if you’re trying to fly out of IAH: my daughter has been in TSA line there for 8hours now and still not through security. Missed flight. Sleeping at airport to make sure she doesn’t miss her rebooked flight tomorrow am. Nightmare.
I have spent twenty years as a cardiologist. I have held dying patients’ hands at 3 a.m. I have delivered news that shattered families. Through all of it, I have clung to one simple belief: doctors exist to protect people, especially the vulnerable.
Then I read the Jeffrey Epstein files. And I felt something I rarely feel in my profession: SHAME.
The documents reveal that Dr. Peter Attia—a physician, longevity expert, bestselling author, and host of one of the most popular health podcasts in America—maintained a close friendship with Epstein for years after Epstein’s 2008 conviction for procuring a minor for prostitution. The emails between them are jarring. Crude jokes. Plans to meet. A relationship so important to Attia that, according to the files, he once prioritized a New York meeting with Epstein over returning to his infant son’s bedside in the ICU.
His wife had begged him to come home. He chose Epstein.
Let me be clear about what we already knew in 2008. Jeffrey Epstein pleaded guilty to crimes involving a child. He was a registered sex offender. This was not a rumor. It was not gossip. It was a matter of public record.
And yet, from 2014 to 2019, Attia maintained this friendship. He joked in emails about having “JE withdrawal.” He expressed concern about Epstein’s “legal troubles”—not about the victims, the girls, the children whose lives Epstein destroyed.
In his public statement this February, Attia framed his choices as naivety. He claims he saw Epstein’s crimes as “prostitution-related” until a 2018 Miami Herald exposé revealed the full horror. He calls his emails “juvenile.” He says he has grown.
Maybe he has. People can change.
But here is what troubles me as a physician: Where was the instinct to protect?
Every doctor in America is trained as a mandatory reporter. The American Medical Association’s code of ethics is explicit: if we have “reasonable cause to suspect” child abuse, we must report it. We do not need proof. We need suspicion. The law exists because doctors have access to information and influence that ordinary citizens do not. We are positioned to notice what others miss. We are trusted to act.
Now, mandatory reporting typically applies to clinical settings—a child who shows up in your office with suspicious bruises, a patient who discloses abuse. Attia was not Epstein’s physician. He was his friend.
But ethics do not stop at the clinic door.
When a physician knows someone is a convicted child sex offender and chooses to maintain that friendship—to joke around, to share meals, to prioritize that relationship over his own family—what message does that send? What does it say about our profession’s values?
Some have called for Attia’s medical license to be revoked. I understand the impulse. But I think the problem is bigger than one doctor.
Jeffrey Epstein did not just befriend physicians. He bought access to science itself.
Between 1998 and 2008, Epstein donated over $9 million to Harvard University. He funded a program in evolutionary dynamics. He gained an office on campus. He became a “visiting fellow” in the psychology department—despite having no academic credentials whatsoever.
After his 2008 conviction, Harvard officially stopped accepting his money. But the relationships continued. Former university president Lawrence Summers kept meeting with him, reportedly soliciting advice and indirect donations. Faculty members attended Epstein’s now-infamous dinner parties, gatherings that were notably all-male, where conversations veered into pseudoscientific musings about eugenics and “improving” the human race.
Epstein understood something that the rest of us are only beginning to reckon with: money opens doors that should stay closed.
He used his wealth to position himself as a “patron of science.” He cultivated relationships with Stephen Hawking, with geneticists, with AI researchers. He hosted conferences. He funded research. And in return, he got something priceless: legitimacy.
When a predator can sit at dinner with Nobel laureates, when he can stroll across Harvard Yard with an office key in his pocket, when leading physicians call him a friend—he becomes harder to see as a monster. The credentials of the people around him become his camouflage.
This is how institutions fail.
It is not dramatic. It is not a single corrupt decision. It is a thousand small compromises. It is a grant application that needs funding. It is a dinner invitation that seems harmless. It is the thought: He already served his time. Who am I to judge?
It is, as geneticist George Church put it, “nerd tunnel vision”—the tendency to focus so intensely on research that ethical questions blur into background noise.
But there is another name for this: complicity.
When MIT’s Media Lab was revealed to have accepted hidden donations from Epstein, the director resigned. The institution launched investigations. There was accountability, however belated.
In medicine, we have been slower to reckon.
Attia is not an outlier. He is a symptom. He represents a growing class of “influencer doctors” whose brands depend on access, on elite networks, on proximity to wealth and power. His practice reportedly charges clients $150,000 a year. His podcast reaches millions. His bestselling book promises to help readers live longer.
None of this is inherently wrong. But when the model rewards networking over service, when career advancement depends on who you know rather than who you heal, the profession drifts from its purpose.
And when the people you know include convicted child sex offenders, the drift becomes a fall.
Public trust in medicine is fragile. We have spent years watching it erode—through pandemic misinformation, through pharmaceutical scandals, through a healthcare system that often seems to value profit over patients.
We cannot afford to give people more reasons to doubt us.
The Epstein files are a gift, in a way. They are a mirror. They force us to ask uncomfortable questions: What are we willing to overlook for funding? For access? For prestige? Where do we draw the line between professional ambition and moral compromise?
And they demand that we answer.
Here is what I believe we must do.
First, we need stronger ethical guidelines. The AMA should clarify physicians’ responsibilities when they encounter evidence of abuse outside clinical settings. Mandatory reporting should not be a technicality we hide behind.
Second, institutions must vet their donors. Harvard, MIT, and countless other universities accepted Epstein’s money with minimal scrutiny. After the scandals broke, they scrambled to distance themselves. This is backwards. Transparency should come first, not last. Anonymous donations to research institutions should be banned. Donor backgrounds should be reviewed before checks are cashed.
Third, we need to diversify how science is funded. When researchers depend on wealthy individuals for grants, they become vulnerable to manipulation. Public funding, foundation support, and transparent giving structures can reduce this dependency.
Fourth, and most importantly, physicians must hold ourselves accountable. We cannot wait for institutions to act. Each of us must decide what we stand for.
I am not calling for perfection. We are all flawed. We all make mistakes. But there is a difference between a mistake and a pattern. There is a difference between ignorance and willful blindness.
When a man is convicted of crimes against children, you do not joke around with him. You do not make him a priority. You do not choose him over your own family.
You walk away.
I became a cardiologist because I wanted to heal. I wanted to be there for people in their most frightening moments. I wanted to live by the oath I took: first, do no harm.
That oath means nothing if we harm by association. If we give cover to predators. If we let ambition eclipse integrity.
Peter Attia may have changed. I hope he has. But the profession’s reckoning cannot depend on one man’s growth.
It depends on all of us.
It depends on choosing patients over prestige, service over access, and conscience over convenience.
It depends on remembering why we became doctors in the first place.
🚨📢Calling Interventional Cardiology Fellows
@MayoClinicCV has an opening for our Structural Heart Disease Fellowship for 2026-27 in Rochester, MN.
Please complete application via https://t.co/KZ6yQAsfWX
Any questions can be forwarded to Ellie Fate at [email protected]
To those in MN, if you smell or inhale any chemical smoke or gas, leave the area immediately and move to fresh air. These exposures can cause serious breathing problems and worsen asthma, heart disease, and other conditions—especially in children, older adults, and pregnant people. Report the exposure and seek medical care if you experience coughing, chest tightness, burning eyes, dizziness, or shortness of breath.
"Over the last 30 years, I have hospitalized hundreds of children with complications from influenza, RSV, and other vaccine-preventable diseases that have now been removed from the CDC schedule. I have never hospitalized a child from a vaccine reaction."
https://t.co/DEkRxNQyvJ
A baby who contracts HepB in the first year of life has a 90% chance of developing chronic HepB.
A patient with chronic HepB has a 25% chance of cirrhosis, liver failure and liver cancer.
We have no cure for HepB.
For 30 years, we had a universal vaccine plan.
Until today.
Among the citizens detained by immigration agents are nearly 20 children, including two with cancer. Four children were held for weeks with their undocumented mother and without access to the family’s attorney until a congresswoman intervened.
https://t.co/D4ctDgY76f
The new head of the CDC, Jim O’Neill, has no degree in science or medicine, and has pushed unproven treatments for COVID like ivermectin. This is so incredibly dangerous.
Scientists at the University of Florida have created a breakthrough mRNA cancer vaccine that erased deadly brain tumors in early human trials without chemo or radiation. Tested on four glioblastoma patients, the vaccine reprogrammed their immune systems within 48 hours to attack the tumor. Built from each patient’s own tumor cells and delivered via lipid nanoparticles, it showed success similar to earlier tests in mice and dogs. It is now moving into Phase 1 pediatric trials.
1/n When you actually bother to read the HHSBARDA statement you realize how untethered from reality he has become, MAHA pseudoscience. For instance this statement below touting benefits of whole inactivated virus vaccines for serious respiratory infections https://t.co/NjfOHNDF9L
500,000 Americans will be infected with C0VlD today.
Based on the data consistently showing 1-in-5 infections results in Long C0VlD, another 100,000 people will go on to develop Long C0VlD in the U.S. just from today’s infections.