➡️HOT FROM THE PRESS
Multidisciplinary expert panel report on fluid stewardship: perspectives and practice
FULLTEXT https://t.co/xEJBo6KDol
#FOAMcc#FOAMed@AzOudenaarde@Medaman_AtoQ
💧Potassium, Magnesium and Electrolytes in the Critically Ill
Small Ions, Big Consequences
This chapter reviews the key roles of potassium, magnesium, calcium and phosphate in neuromuscular excitability, cardiac conduction and cellular metabolism. It highlights how even modest deviations in K⁺ or Mg²⁺ can precipitate arrhythmias, particularly in the presence of sepsis, diuretics, or renal dysfunction.
Correction Strategies and Pitfalls
Using data from observational and interventional studies, the authors discuss IV vs oral replacement, safe rates of correction, and the interplay between magnesium and potassium repletion. Practical tables list typical replacement regimens and monitoring intervals, stressing that fluid and electrolyte therapy should be prescribed with the same caution as any other drug.
📘 See Rational Use of IV Fluids in Critically Ill Patients - chapters on electrolyte management for full tables and dosing guidance.
🔵 At IFAD 2026, electrolyte sessions will be integrated with fluid strategy, acid–base and renal protection.
👉Registration: https://t.co/wATwBWBg5M
#Potassium #Magnesium #Arrhythmia #ICU
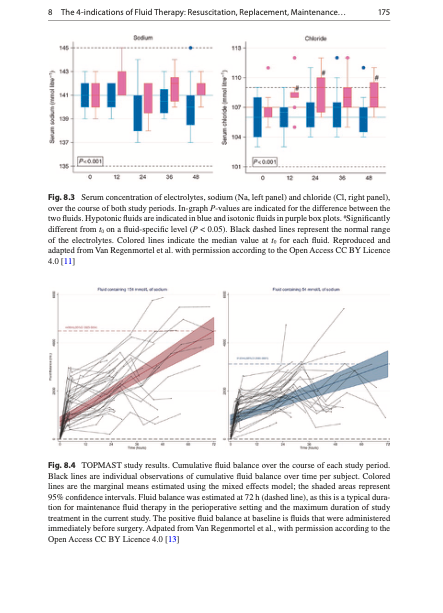
💧Composition of Intravenous Fluids
What’s in the Bag Matters
This chapter systematically compares commonly used crystalloids and colloids—their sodium, chloride, buffer content, osmolality and strong ion difference. It explains why 0.9% saline is not “physiologic”, how buffered solutions differ (lactate, acetate, gluconate), and which colloids have fallen out of favor because of renal or coagulation concerns.
Choosing Fluids Intelligently
Tables summarize the composition of each solution and map them to typical indications and cautions. Clinicians are encouraged to match fluid composition to the patient’s acid–base status, electrolyte profile, and phase of illness rather than choosing based on habit or availability alone.
🔵 IFAD 2026 will address how to redesign hospital formularies and order sets around stewardship principles.
👉Registration: https://t.co/wATwBWBg5M
#Crystalloids #Colloids #IVFluids #FluidStewardship
🫁🔰Ventilación guiada por fisiología,Cuando el ventilador y el paciente no están de acuerdo.
✅️Este consenso Delphi redefine la asincronía paciente-ventilador como un fenómeno fisiopatológico complejo y no solamente como una “anomalía de curvas”🫁. La ventilación mecánica moderna debe evolucionar desde parámetros estáticos hacia una monitorización dinámica de la interacción neuro-mecánica paciente-ventilador.
☝🏻🤓El verdadero objetivo no es únicamente oxigenar o ventilar, sino lograr una sincronía fisiológica protectora, minimizando tanto el daño pulmonar como el daño diafragmático y neurológico asociado a la ventilación mecánica.
🫁La asincronía paciente-ventilador. Mediante una metodología Delphi con expertos internacionales en cuidados críticos, ventilación mecánica, fisiología respiratoria y monitoreo avanzado, el trabajo busca estandarizar conceptos, terminología y estrategias diagnósticas relacionadas con la interacción paciente-ventilador.
➡️Las asincronías ocurren cuando existe una discrepancia entre el esfuerzo neural del paciente y la respuesta mecánica del ventilador. 🔰📝Estas alteraciones pueden incrementar el trabajo respiratorio, provocar lesión pulmonar inducida por ventilación (VILI), lesión diafragmática, sedación excesiva, delirium, fracaso en el destete y mayor mortalidad.
📝El consenso Delphi propone una clasificación fisiopatológica clara basada en:Asincronías de disparo (trigger),Asincronías de flujo, Asincronías de ciclado,Asincronías complejas o múltiples.
🫁Muchas asincronías pasan desapercibidas cuando solo se observan parámetros básicos del ventilador, resaltando la importancia de interpretar las curvas de presión, flujo y volumen en tiempo real.
➡️Se debe integrar: Monitoreo esofágico,actividad eléctrica diafragmática,ultrasonido diafragmático,presión muscular inspiratoria.
☕ Perlas cafeteras académicas
☕🫁 1. La asincronía no es un “detalle técnico”La asincronía persistente puede generar: Aumento del consumo de oxígeno,fatiga diafragmática,auto-PEEP,volutraumay fracaso del weaning.
☕📈 2. Las curvas del ventilador son “el ECG del pulmón”
🔰Interpretar curvas ventilatorias.
📝Las más importantes: presión-tiempo,flujo-tiempo,volumen-tiempo.
☕⚡ 3. El doble trigger es altamente lesivo⚠️
➡️Ocurre cuando el esfuerzo neural del paciente excede el tiempo inspiratorio programado.
Puede producir:🔹️breath stacking.
y ocurre típicamente durante:
●Doble trigger (doble disparo),
●tiempo inspiratorio insuficiente,
●drive respiratorio elevado,
●asincronía paciente-ventilador.
📝El paciente continúa intentando inspirar mientras el ventilador ya terminó el ciclo inspiratorio, desencadenando una segunda respiración consecutiva.
🔹️Aumento crítico del volumen tidal,
🔹️Incremento del stress y strain pulmonar.
☕🫀 4. La sedación excesiva también genera asincronía
⚠️No toda asincronía se corrige sedando más.‼️
🔹️La depresión del drive respiratorio puede favorecer los disparos inefectivos,hipoventilación,atrofia diafragmática.
☕🌊 5. El flujo inspiratorio insuficiente es una causa frecuente olvidada😵💫
➡️Cuando el ventilador no satisface la demanda inspiratoria aumenta el trabajo respiratorio, aparece “air hunger”(hambre de aire) y el paciente lucha contra el ventilador.🥴
☕🧠 6. La asincronía puede preceder al delirium y al síndrome post-cuidados intensivos.post-UCI
🔰La sensación de “no poder respirar” durante ventilación mecánica es un factor psicológico importante asociado ansiedad extrema.síndrome post-cuidados intensivos.
☕📉 7. Los disparos inefectivos suelen asociarse a auto-PEEP
Especialmente en:EPOC,asma,
SDRA obstructivo,ventilación con tiempos espiratorios cortos.
🔍 Clasificación simplificada de asincronías
☝🏻🤓🫁
🔹️Trigger ➡️Trigger inefectivo➡️ Fatiga respiratoria
🔹️Flujo➡️ Flujo insuficiente ➡️Air hunger
🔹️Ciclado➡️ Doble trigger➡️ Volutrauma
🔹️Espiratoria ➡️Ciclado tardío ➡️Auto-PEEP
🔹️Reverse triggering ➡️Lesión pulmonar y diafragmática.
👇🏽👇🏽👇🏽👇🏽
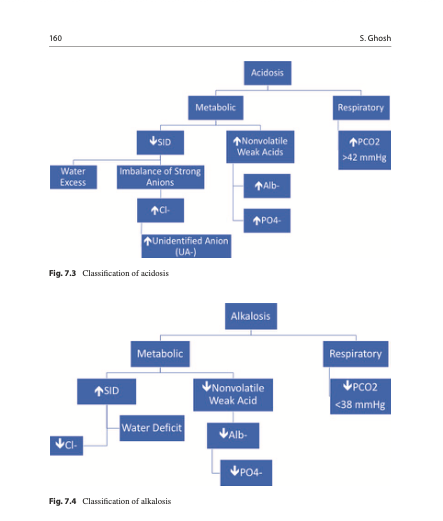
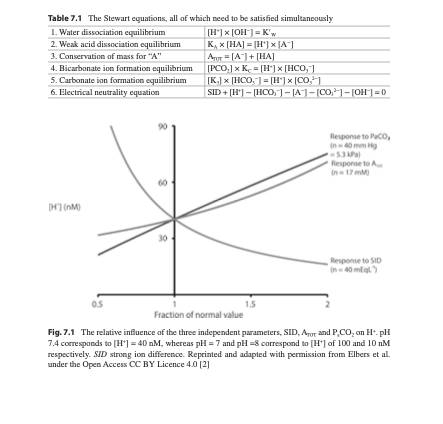
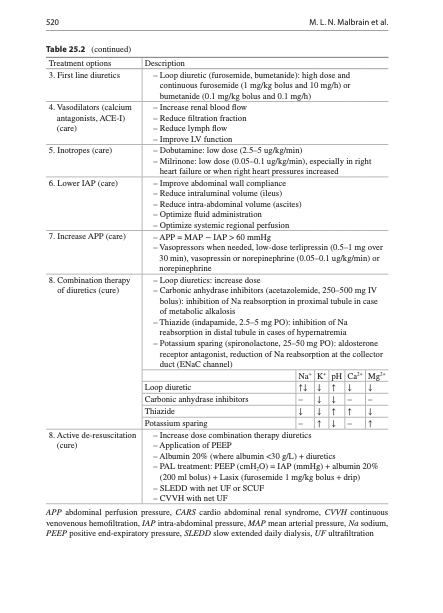
💧 Acid–Base Effects of IV Fluids – Stewart Approach
Beyond bicarbonate: Strong Ion Difference
This chapter introduces the Stewart approach, where pH is determined by strong ion difference, PaCO₂ and weak acids rather than bicarbonate alone. It shows how chloride‑rich fluids reduce the strong ion difference and drive hyperchloremic metabolic acidosis, whereas balanced solutions better preserve acid–base equilibrium.
Clinical Application at the Bedside
Through worked examples, the authors demonstrate how to interpret ABGs after large volumes of saline vs balanced crystalloids. Recognizing fluid‑induced acid–base changes helps clinicians adjust both fluid choice and ventilatory strategy, especially in patients with sepsis, kidney injury or major surgery.
📘 Detailed figures and case discussions in the acid–base chapter: https://t.co/7pvDxZGh4I
🔵 At IFAD 2026, a dedicated session will apply the Stewart approach to real ICU blood gases and fluid decisions.
👉Registration: https://t.co/wATwBWAIge
#AcidBase #StewartApproach #Chloride #ICU
💧Indications for Intravenous Fluids – Getting the Basics Right
Four Indications Only
his chapter distills fluid use into four indications: resuscitation, maintenance, replacement and carrier for drugs/nutrition. It argues that many problems arise when these indications are blurred—for example, resuscitation fluids drifting into unreviewed “maintenance” or carriers being ignored in daily fluid balance.
From Intuition to Prescription
Algorithms and tables link common clinical scenarios (hypovolaemic shock, perioperative fasting, diarrhoea, fever, diuretics) to specific indications and fluid choices. The emphasis is on writing clear fluid orders—type, volume, rate, target—and building daily review into routine rounds.
📘 Full classification and algorithms: https://t.co/7pvDxZGOUg
🔵 IFAD 2026 will show how to embed this four‑indication framework into order sets, electronic records and ward practice.
👉Registration: https://t.co/wATwBWBg5M
#IVFluids #Indications #FluidStewardship #HospitalMedicine
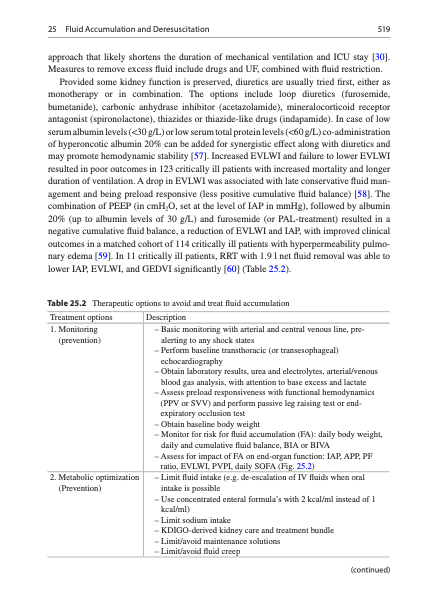
💧Monitoring Fluid Balance – Seeing the Full Picture
Why Daily Weights and Balances Matter
This chapter highlights the limitations of “ins and outs” alone and advocates combining meticulous input/output charting with daily weights and bedside assessment of edema, lung water and organ function. Even modest daily positive balances, when unnoticed, can accumulate to significant tissue edema and ventilator dependence.
From Numbers to Decisions
he authors propose thresholds (e.g. >5% weight gain from baseline) and patterns that should trigger a reassessment of fluids, diuretics or ultrafiltration. They also discuss technical tools—bio‑impedance analysis, transpulmonary thermodilution, ultrasound‑based congestion scores—that refine volume assessment beyond physical exam alone.
📘 All measurement methods and cut‑offs: https://t.co/7pvDxZGOUg
🔵 IFAD 2026 will feature practical sessions on integrating congestion scores and advanced monitoring into ICU rounding.
👉Registration: https://t.co/wATwBWBg5M
#FluidBalance #VolumeStatus #Congestion #ICU
💧 Fluid Management in Sepsis and Septic Shock
Early, but Not Excessive
This core chapter revisits sepsis resuscitation in the era of stewardship, showing how initial fluids remain essential to reverse life‑threatening hypoperfusion, but fixed large bolus protocols can lead to harmful volume overload when applied indiscriminately. It integrates the ROSE concept, emphasizing short, targeted resuscitation followed by optimization and, where needed, timely evacuation.
Dynamic Assessment and Early Vasopressors
The authors advocate dynamic tests of fluid responsiveness (passive leg raising, stroke volume variation, echocardiographic indices) and early vasopressor support rather than repeated blind boluses. Evidence linking positive fluid balance with mortality in sepsis is summarized, underlining the need for explicit stop rules and deresuscitation plans once shock has resolved.
📘 Full sepsis algorithms and case vignettes in Chapter 14.
🔵 IFAD 2026 in Antwerp will devote multiple sessions to sepsis fluid management, including hands‑on hemodynamics and stewardship.
👉Registration: https://t.co/wATwBWAIge
#Sepsis #SepticShock #FluidResuscitation #ICU #ROSE #FluidStewardship
💧 Fluid Resuscitation in Trauma
From High‑Volume to Damage‑Control Resuscitation
The trauma chapter tracks the shift from aggressive crystalloid loading to damage‑control resuscitation with early haemorrhage control, permissive hypotension (in selected patients), and balanced blood product transfusion. Excessive crystalloids dilute coagulation factors, worsen acidosis and hypothermia, and contribute to abdominal and limb compartment syndromes.
Tailoring Fluids to Mechanism and Phase
The authors differentiate blunt vs penetrating trauma, isolated TBI vs multi‑trauma, and early controlled vs ongoing bleeding, with different targets for blood pressure and fluid type. They stress continuous reassessment, early recognition of abdominal compartment syndrome (with intra‑abdominal pressure monitoring), and the role of point‑of‑care coagulation testing to guide additional products rather than “just more fluids”.
📘 Full trauma chapter in Rational Use of Intravenous Fluids in Critically Ill Patients.
👉 https://t.co/7pvDxZGh4I
🔵 Trauma resuscitation and abdominal hypertension will be key topics at IFAD 2026.
👉Registration: https://t.co/wATwBWAIge
#Trauma #DamageControlResuscitation #MassiveTransfusion #AbdominalCompartmentSyndrome
💧 Fluid Management in Neurocritical Care
Avoiding Secondary Brain Injury
This chapter focuses on maintaining cerebral perfusion while avoiding fluid‑induced brain swelling and electrolyte disturbances. Hypotonic solutions and free water are explicitly discouraged in patients with TBI or subarachnoid haemorrhage because they lower plasma osmolality and promote cerebral edema; hypertonic saline and carefully titrated isotonic crystalloids are preferred.
Integrating ICP, CPP and Electrolytes
Evidence from randomized trials and consensus statements is synthesized to show how hypervolaemic or hyperdynamic therapy can worsen outcome if used indiscriminately. The authors stress frequent monitoring of ICP, CPP, serum sodium and osmolality, and aligning fluid choices with overall neuroprotective strategies including ventilation, sedation and osmotherapy.
📘 Full neurocritical care chapter in Rational Use of Intravenous Fluids in Critically Ill Patients:
👉 https://t.co/7pvDxZGh4I
#NeuroICU #TBI #SAH #HypertonicSaline #FluidTherapy
Join the Fluid Academy during iWIN in Catania.
📅 26 June 2026
📍 Palazzo della Cultura, Catania (IT)
💻 Hybrid: onsite + virtual
Session 4 focuses on fluids, VExUS and hemodynamic monitoring for daily ICU and perioperative practice.
💙 Secure Your Seat: https://t.co/LmvjhYkMYg
#IFAD #IFADmini #IFADmicro #IFADnano
💧 Fluid Management in Heart Failure and Cardiogenic Shock
Preload vs Congestion
This chapter explains that in acute and chronic heart failure, the challenge is not simply “giving or withholding fluids” but balancing preload to support cardiac output against the risk of venous congestion and pulmonary edema. Conventional preload markers (CVP, PAOP) are often misleading in dilated, stiff or ischemic ventricles, so the authors emphasize integrated assessment using echo, blood pressure, urine output and clinical signs of congestion.
Cardiogenic Shock Strategy
In cardiogenic shock, small, carefully tested fluid challenges may be justified early, but ongoing hypotension is usually better addressed with inotropes, vasopressors and mechanical support rather than repetitive fluid boluses. The chapter highlights how positive fluid balance worsens outcomes in decompensated heart failure and advocates early decongestive therapy and, when needed, ultrafiltration as part of a broader deresuscitation plan.
📘 Full chapter in Rational Use of Intravenous Fluids in Critically Ill Patients:
👉 https://t.co/7pvDxZGOUg
🔵 Discussed in depth at IFAD 2026 in Antwerp.
👉Registration: https://t.co/wATwBWBg5M
#HeartFailure #CardiogenicShock #FluidManagement #VEXUS #ICU
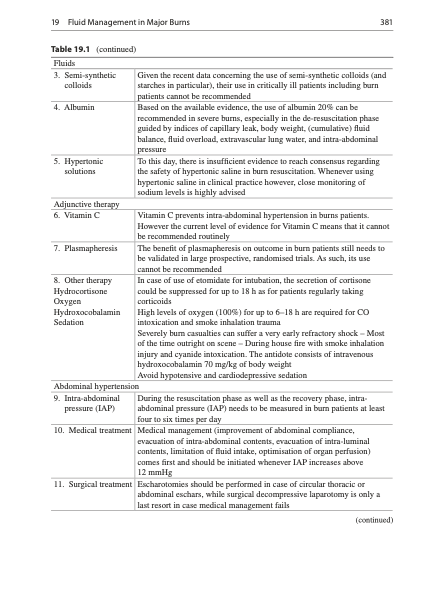
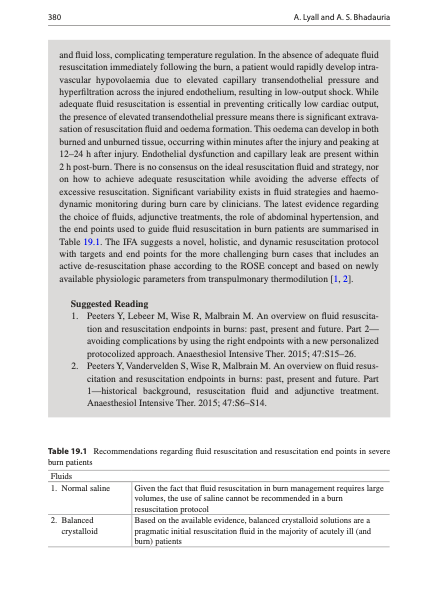
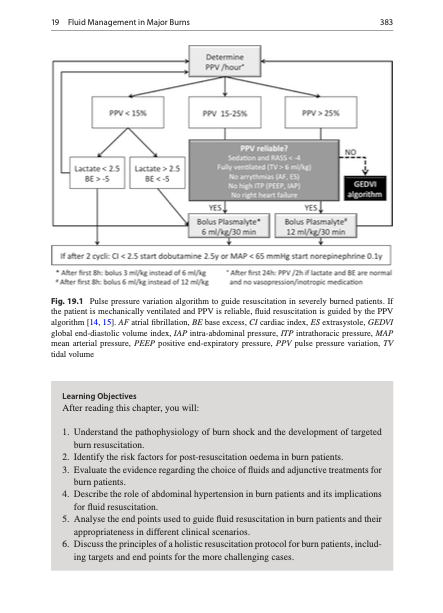
💧 Fluid Management in Major Burns
Parkland and Beyond
Using historical and contemporary data, this chapter describes initial resuscitation with Ringer’s lactate or Plasma‑Lyte based on TBSA burned (e.g. Parkland formula: 4 mL/kg/%TBSA in 24 h, half in first 8 h), while warning against uncritical adherence to formulas without bedside reassessment.
Avoiding Fluid Creep and Complications
Tables summarize complications of over‑resuscitation—worsening edema, airway obstruction, ARDS, abdominal compartment syndrome—and the limited but growing evidence on colloid use later in the course to reduce total crystalloid volume. The chapter concludes that endpoints such as urine output, lactate, mental status and abdominal perfusion pressure are more important than hitting a calculated volume exactly.
📘 Full “Fluid Management in Major Burns” chapter in Rational Use of Intravenous Fluids in Critically Ill Patients:
👉 https://t.co/7pvDxZGh4I
🔵 ROSE‑based strategies will be presented at IFAD 2026.
👉Registration: https://t.co/wATwBWAIge
#Burns #ParklandFormula #ARDS #AbdominalCompartmentSyndrome #ICU
Join us tomorrow in Catania (or online) for IFADmini – a full-day, high-yield journey through fluid management and hemodynamics.
📅 Tomorrow – 26 June 2026
📍 PALAZZO DELLA CULTURA, CATANIA (IT)
💻 Hybrid format – onsite & virtual
🔗 Register now: https://t.co/LmvjhYkMYg
IFADmini offers a concise curriculum from cardiovascular physiology and preload responsiveness to sepsis, cardiogenic shock, ECMO and AI-guided fluid therapy, with constant focus on practical bedside decisions for ICU, anesthesia, perioperative and acute care teams.
Registration for IFAD 2026 is now open.
Our Executive Board is ready to welcome you to a highly interactive, clinically focused meeting where education meets practice.
🌊 Registration follows a wave-based pricing system.
Once a ticket wave is sold out, the next pricing tier automatically applies.
⚠️Secure your spot early and be part of a different kind of learning experience in Antwerp.
➡️ https://t.co/7XkKFbtjVK
Free webinar 👩💻👨💻
Breaking The Habit: Individualised IV fluid prescribing and stewardship, delivered by Turning the Tide in collaboration with the International Fluid Academy (IFA), and sponsored by Baxter.
🎙️ Speaker spotlight: Dr Justin Kirk-Bayley
Dr Justin Kirk-Bayley will be one of the featured speakers in our upcoming webinar on IV fluid prescribing and stewardship.
He is a Consultant Intensivist and Anaesthetist at Royal Surrey NHS Foundation Trust and a recognised expert in lung ultrasound and IV fluid management. He is also a council member of the Intensive Care Society and leads their work in lung ultrasound.
Dr Kirk-Bayley is actively involved in education through a UK charity focused on improving IV fluid practices and regularly presents at conferences and webinars.
Join his talk: What’s in a bag? Right drug, right patient, right time
📅 Date: Monday 6 July 2026
🕔 Time: 17:00 CET / 16:00 UK & Portugal
Register here:
https://t.co/7dTvJYAX62
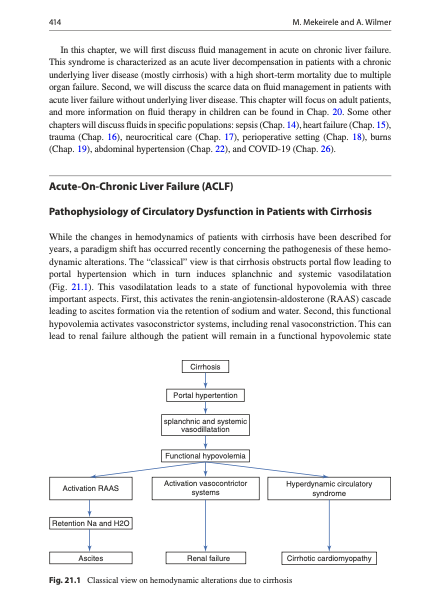
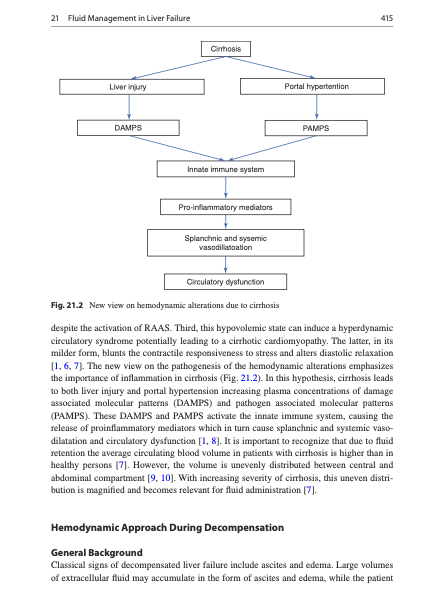
💧 Fluid Management in Liver Failure and Ascites
Circulatory Dysfunction and Effective Hypovolaemia
The liver failure chapter explains that despite edema and ascites, many patients with cirrhosis are effectively underfilled due to splanchnic vasodilation and low effective arterial blood volume. This creates a delicate balance: excessive fluids exacerbate ascites and hyponatraemia, while under‑resuscitation risks renal hypoperfusion and hepatorenal syndrome.
Albumin, Paracentesis and Vasoactive Drugs
The authors review indications and dosing for albumin following large‑volume paracentesis, in spontaneous bacterial peritonitis and in prevention/treatment of hepatorenal syndrome, drawing on key clinical trials. Practical tables link specific clinical situations (e.g. tense ascites, SBP, HRS) to albumin and vasoconstrictor strategies while reinforcing sodium restriction and diuretic stewardship.
📘 Full liver failure chapter in Rational Use of Intravenous Fluids in Critically Ill Patients:
👉 https://t.co/7pvDxZGh4I
🔵 IFAD 2026 will address albumin use and fluid management in decompensated cirrhosis and liver ICU.
👉Registration: https://t.co/wATwBWAIge
#LiverFailure #Ascites #Albumin #HepatorenalSyndrome #ICU
Fluids save lives.
But excess fluids can harm.
Fluid Accumulation Syndrome (FAS) is not just “edema”—it is a reflection of disease severity, capillary leak, and impaired physiology.
In critical illness, disruption of the endothelial glycocalyx and increased vascular permeability lead to fluid shifting into the interstitium—triggering a cascade of organ dysfunction:
🧠 Brain: edema, delirium, ↑ ICP
🫁 Lungs: pulmonary edema, impaired oxygenation
❤️ Heart: myocardial edema, ↓ contractility
🧂 Kidneys: venous congestion, AKI
🦠 Gut: “motor of MOF” → ileus, bacterial translocation
📉 The consequence?
A positive fluid balance is consistently associated with worse outcomes and increased mortality.
💡 Key message:
Fluid therapy requires the same precision as any drug—right indication, right dose, right timing, and early de-escalation.
👉 Learn more in the Fluid Champion Course: https://t.co/yzkzSKOwM2
👉 Join us at IFAD 2026 to translate physiology into practice: https://t.co/7XkKFbtRLi
#FluidAccumulation #CapillaryLeak #Glycocalyx #OrganDysfunction #Sepsis #CriticalCareMedicine #FluidBalance #DeResuscitation #Hemodynamics #IFAD2026
We still prescribe IV fluids as if they are harmless.
But fluids are drugs.
With dose.
With timing.
With side effects.
And yet:
• Fluid creep remains underrecognized
• Maintenance fluids are often misused
• De-resuscitation is delayed
It’s time to move from habit-based to physiology-driven fluid management.
What is the most common fluid mistake you see in your daily practice?
👇 Share your experience.
➡️ explore how your peers approach fluid therapy: https://t.co/g0h3yRlvAM
Only 5 Early Bird tickets remain for IFAD 2026!
As we approach the 15th edition of the International Fluid Academy Days (3–5 December, Antwerp), we are pleased to see strong interest in a format that prioritizes interactive, case-based learning and bedside applicability in fluid stewardship and critical care.
IFAD 2026 is designed as “A Different Kind of Meeting”—moving beyond traditional congress structures toward:
☑️ Small-group, expert-led discussions
☑️ Clinically grounded decision-making
☑️ Integration of physiology into daily practice
☑️ Multidisciplinary exchange across ICU, anesthesia, emergency, and ward settings
Participation is intentionally limited to maintain a high level of interaction and educational value.
With only a few Early Bird registrations still available, we welcome colleagues who are interested in advancing a more physiology-driven, individualized approach to fluid management.
More information on programme and registration:
➡️ https://t.co/Eum08P5us1