Congratulations to @max_herman on his graduation! We’re incredibly proud of all he has accomplished during his Autoimmune Neurology fellowship and can’t wait to see what’s next as he returns to Emory. @Mayo_AING
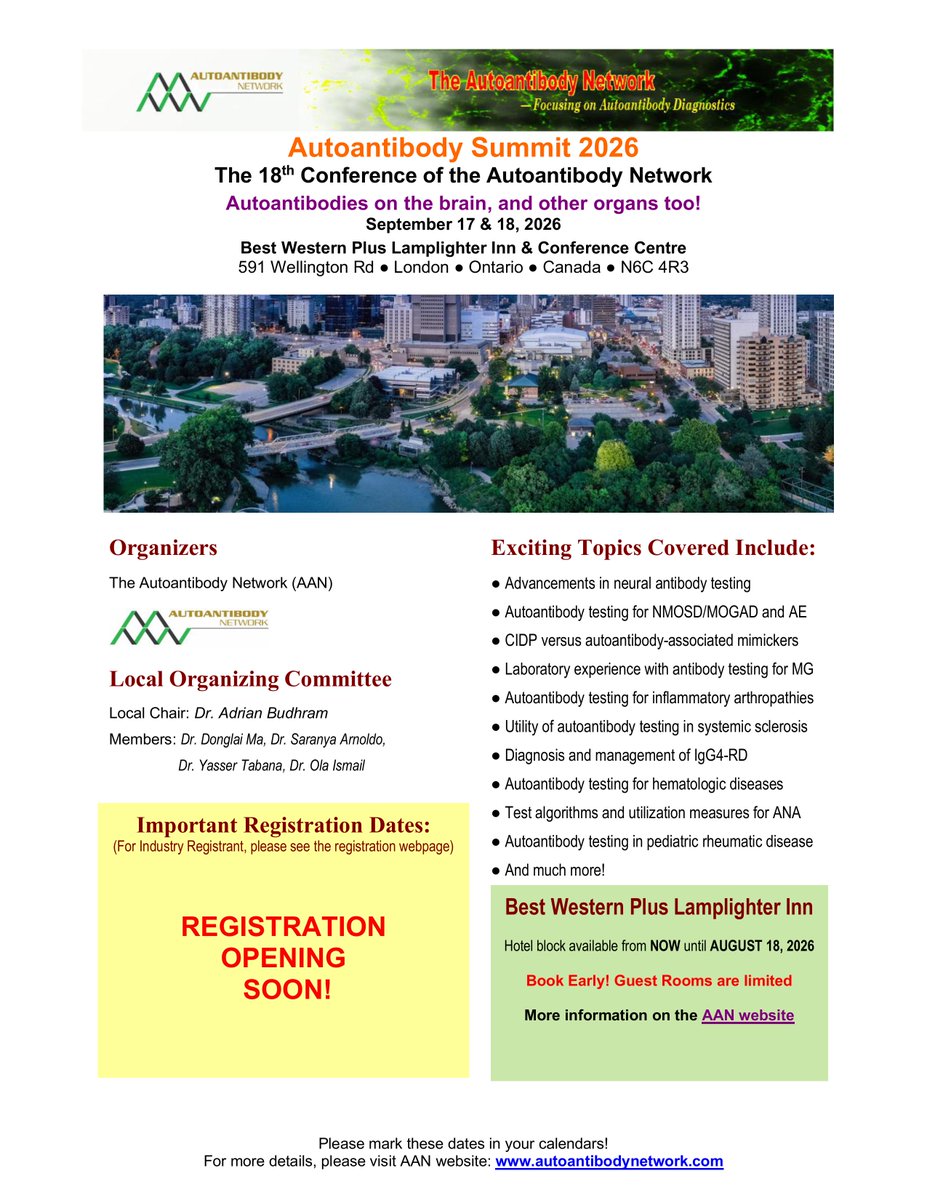
SAVE THE DATE: The 18th Autoantibody Summit is in London, ON Sept 17-18 2026 and focuses on #Neuroimmunology! Will cover #AE, #NMOSD, #MOGAD, #MG, and other autoimmune dx. Link to program below. Registration opens later this month; hope to see you there!
https://t.co/qJxQeYgRLH
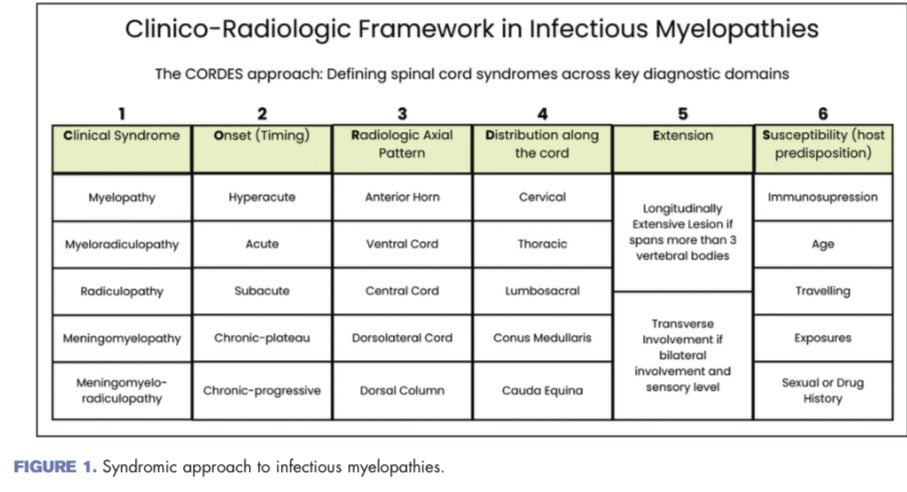
Infectious myelopathies are likely under-recognized.
As neurologists, we should keep them in the differential diagnosis of every myelopathy, as missing them can mean missing a treatable cause!
Here, we share our neurological-perspective review, now in Current Opinion!
#Neurology
Hope you like the waterfall analogy 😜…..
Our latest review framing The ‘cascade’ of events which lead to antibodies causing CNS diseases.
https://t.co/V9OgpqMhLO
Great work by all including
@FederMontini@elinor_wing@max_herman@mdsebaslopez@EoinFlanagan14
IVIg for CIDP: Start with the loading dose (2 g/kg), then give 1 g/kg every 3 weeks. Schedule a follow-up visit in 9-12 weeks. Treatment response should be assessed using the INCAT score (at least 1 point improvement) and/or the MRC sum score (>2 points). If there is no response, reconsider the diagnosis, as it is unlikely to be CIDP. Do not use symptom improvement or “halted progression” as proof of response. Refer to a @gbscidp center of excellence if there is no response or if there are doubts about the diagnosis.
Last call 🚨 Today is the hotel deadline for NCC Orlando 2026.
Mayo Clinic’s 12th Annual Neuro and Intensive Care course is coming to Orlando, May 6–9 at the JW Marriott Orlando with live and livestream options.
If you’re planning to join us in person, now’s the time:
https://t.co/8HN0EIElPx
#NeuroICU #Stroke #CME
@RabihTawkMD@mayoclinicnccfl@mayoclinicnccmn@MayoClinic
Among patients with multiple sclerosis treated long-term with ocrelizumab, interstitial lung disease developed after a mean of 10.5 years, mainly as organizing pneumonia with variable outcomes.
https://t.co/Dzwhp6Jc9T
Happy to share @andreuvilaseca7 et al collaboration with @ESotirchos on the TRUE-MOGAD Score to discriminate true & false positive MOG-IgG
➡️ We have created an online calculator for ease of use:
https://t.co/zjc0YR5JHh
The article link is below:
👇 https://t.co/KbgdKpupVR
@RafidMustafa@MayoClinic So glad I could be part of it, thanks for organizing such an awesome conference.
Excellent meeting and amazing location. Count me in for next year!
🚨 How does a breast tumor cause sudden-onset psychosis and seizures?
A new @Nature paper maps how ectopic NMDA receptors in cancer unmask pre-existing germline B-cells, triggering anti-NMDAR encephalitis.
It answers the WHY
Cancer immunity becomes neurotoxicity🧵
I am biased because I see these patients in a neuroimmunology clinic, where many progressive myelopathies are labeled as “transverse myelitis,” and delayed diagnosis is unfortunately common among them.
Typically a man >50 with slowly progressive myelopathy over months. Radicular pain is a frequent initial symptom, often presenting as chronic, insidious low back pain. Prior spine surgery is not uncommon. Symptoms may worsen with steroids or show only transient improvement. Stepwise decline with exertion/Valsalva,early gait impairment and neurogenic bladder/bowel dysfunction.
Important pitfalls: absence of obvious flow voids on MRI does not exclude the diagnosis. CSF is often abnormal (elevated RBCs protein common), but pleocytosis is uncommon.
A single spinal angiogram may be negative, some patients require repeat, highly selective angiography, and occasionally surgical exploration to localize and treat the fistula.
Any unexplained thoracic myelopathy extending to the conus should prompt a thorough evaluation for a spinal dural AV fistula.
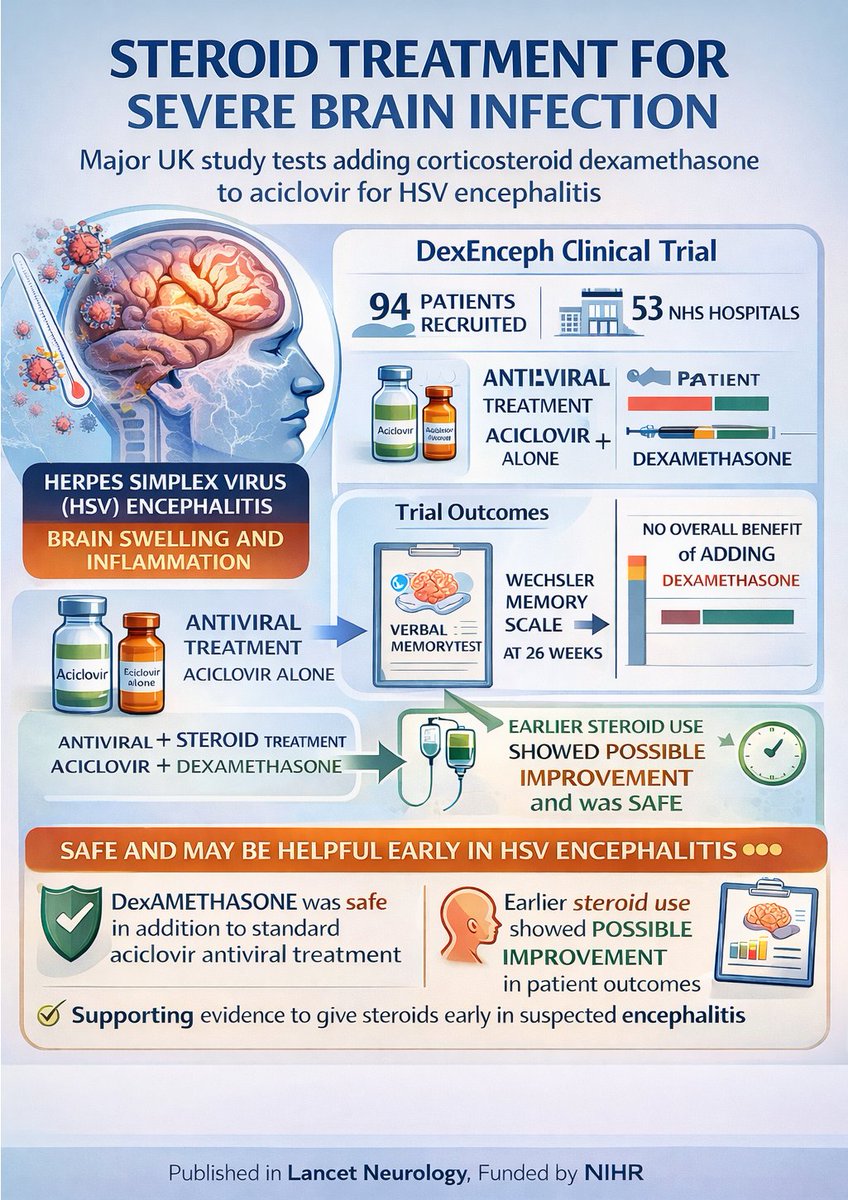
I am very pleased to share our DexEnceph trial is now published in @TheLancet Neurology.
The study shows that if you suspect a patient has encephalitis which might be autoimmune or could be HSV, it's safe to give steroids https://t.co/quCnka8jQE
@encephalitis@ThePandemicInst
This is an excellent review on this topic !
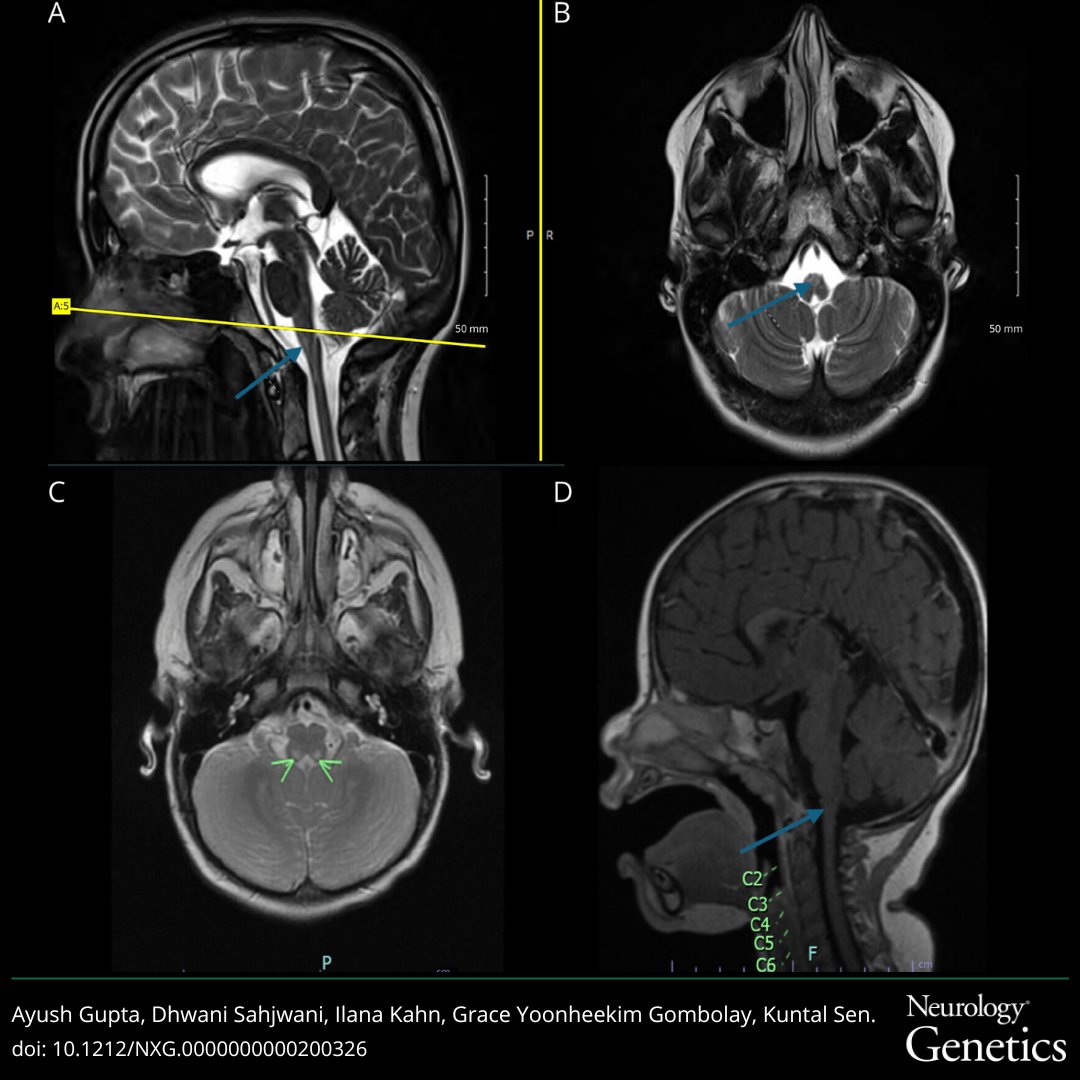
Persistent diagnostic uncertainty in suspected neuroinflammation should trigger genetic testing. You can’t diagnose what you don’t test.
Applying the Supporting Features for MOGAD Diagnosis to Patients With Multiple Sclerosis | Neurology Neuroimmunology & Neuroinflammation https://t.co/eqj2ot5yEf @PietroZara6@MGastaldi85@SaraMariottoMD@RosaCortese5@CartaSra and Giacomo Greco 🇮🇹💣
Who is a spectacularly good #antibody - #protein#biochemist?
and
wants to work on:
1. #Neuroimmune diseases 🧫 🧬
2. A translational environment @Mayo Clinic 🏥 🧑⚕️
3. In Florida ☀️🏝️🏖️
4. With an amazing lab team 👏🏼
If it’s you, please click here ⬇️
https://t.co/TIBLDJ7nB7
In our recent study, the "Insular Knife Cut" Sign had 99.3% specificity for HSV encephalitis and was often detectable early after symptoms onset on brain MRI. An ominous sign not to miss in patients with suspected encephalitis of new onset!!! https://t.co/l6jrmxHeHV
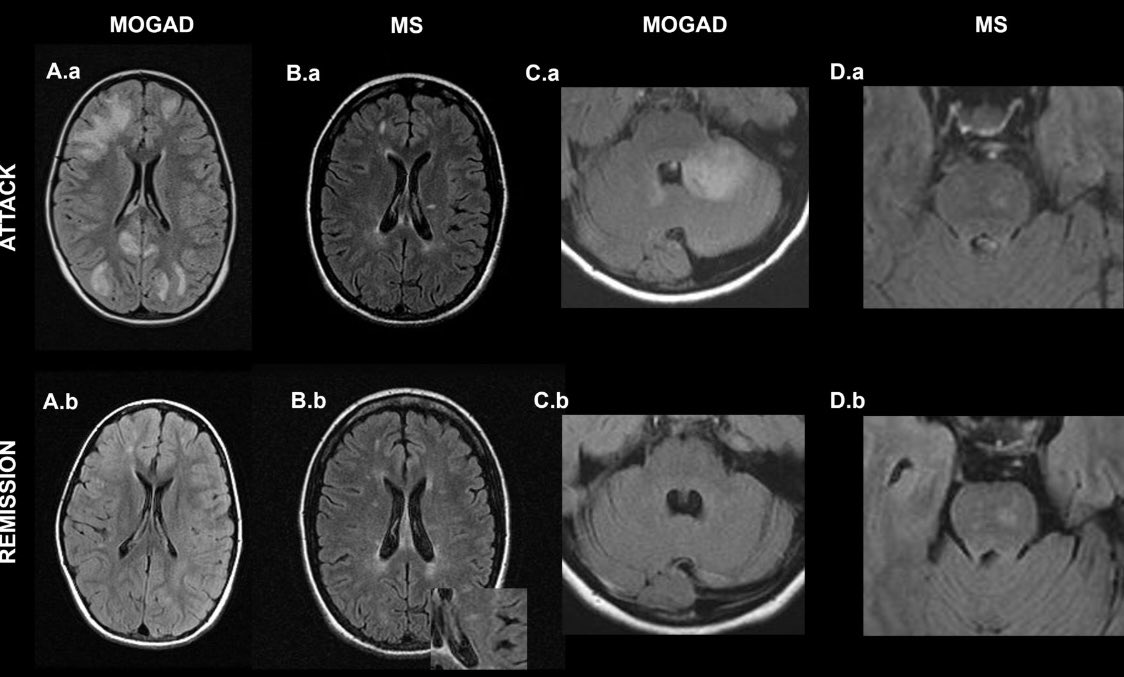
Happy to share Syc-Mazurek et al study of attack & remission MRI in #MOGAD vs #MS ➡️ Resolution of 1 lesion predicts #MOGAD and disappearance of ≥2 lesions separates #MOGAD completely from #MS ➡️ MRI 1 yr post #MOGAD brain/spine attack may aid diagnosis👇https://t.co/n7zDVSKNSY
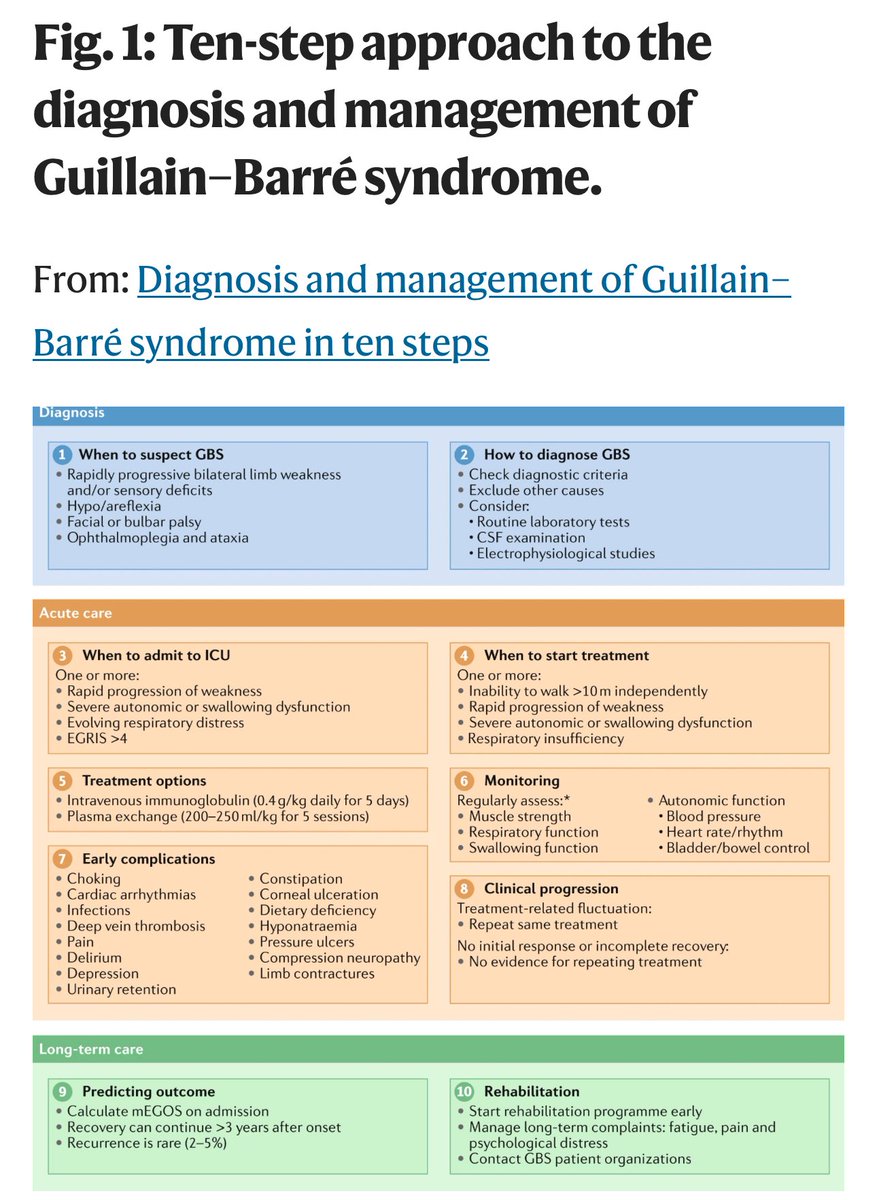
Dear Neurology Residents Starting in the ED Next Month,
You will frequently encounter “?GBS” or “GBS rule out” consults. Please remember to carry your reflex hammer, save this post for future reference, and read the open-access review that I share ⬇️. 🤓
Since you won’t have much time for history taking, make sure to ask about important details such as falls, the use of gait aids, the ability to climb stairs, difficulty walking, using zippers, and washing their hair. These activities can help you gather an accurate timeline. I also suggest asking when they last felt like their usual selves, as this can help pinpoint when the symptoms began, along with their prior level of disability, which is crucial. Don't forget to ask about potential triggers, including recent vaccinations, infections, surgery, and trauma.
The following physical examination features make GBS very unlikely and may assist you in “ruling it out”:
- A sensory level
- Unilateral weakness
- Markedly asymmetric weakness (excluding cranial nerves)
- Weakness confined to either the upper or lower limbs
- Normal (or preserved) ankle reflexes
- Fever or skin rash
- Normal gait
GBS is the most common cause of ascending weakness and paresthesias. So, if history suggests it, the patient is unable to walk, the weakness is symmetric, and the reflexes are reduced/absent, please admit the patient and start IVIg overnight. Time is nerve! 😅
Happy to share @albertaboseif et al multicenter study showing 4% of #MOGAD with meningitis ➡️ Frequent misdiagnosis as infection ➡️ Updates in criteria could incorporate this phenotype ➡️ Path had meningeal T & B cells, microglia & cortical myelin loss👇 https://t.co/7gn8z4HzhH