@HoustonShockHSS@BurkhoffMd@CSWorkingGroup@JumeanMarwan@NirUrielMD@Nikhil15
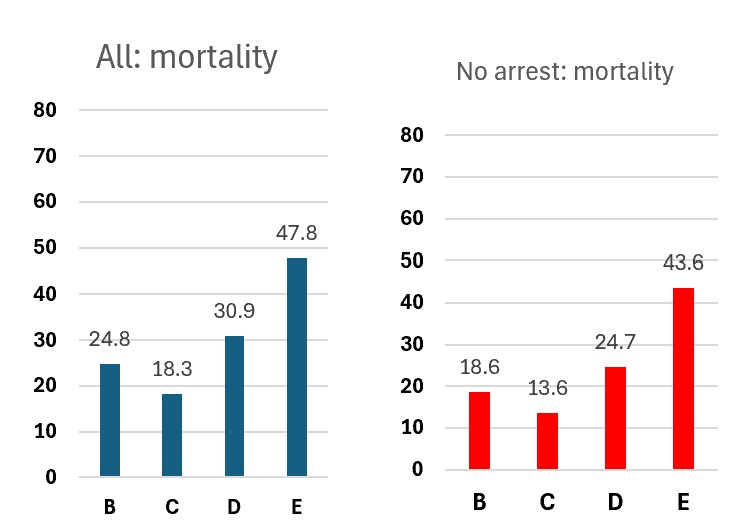
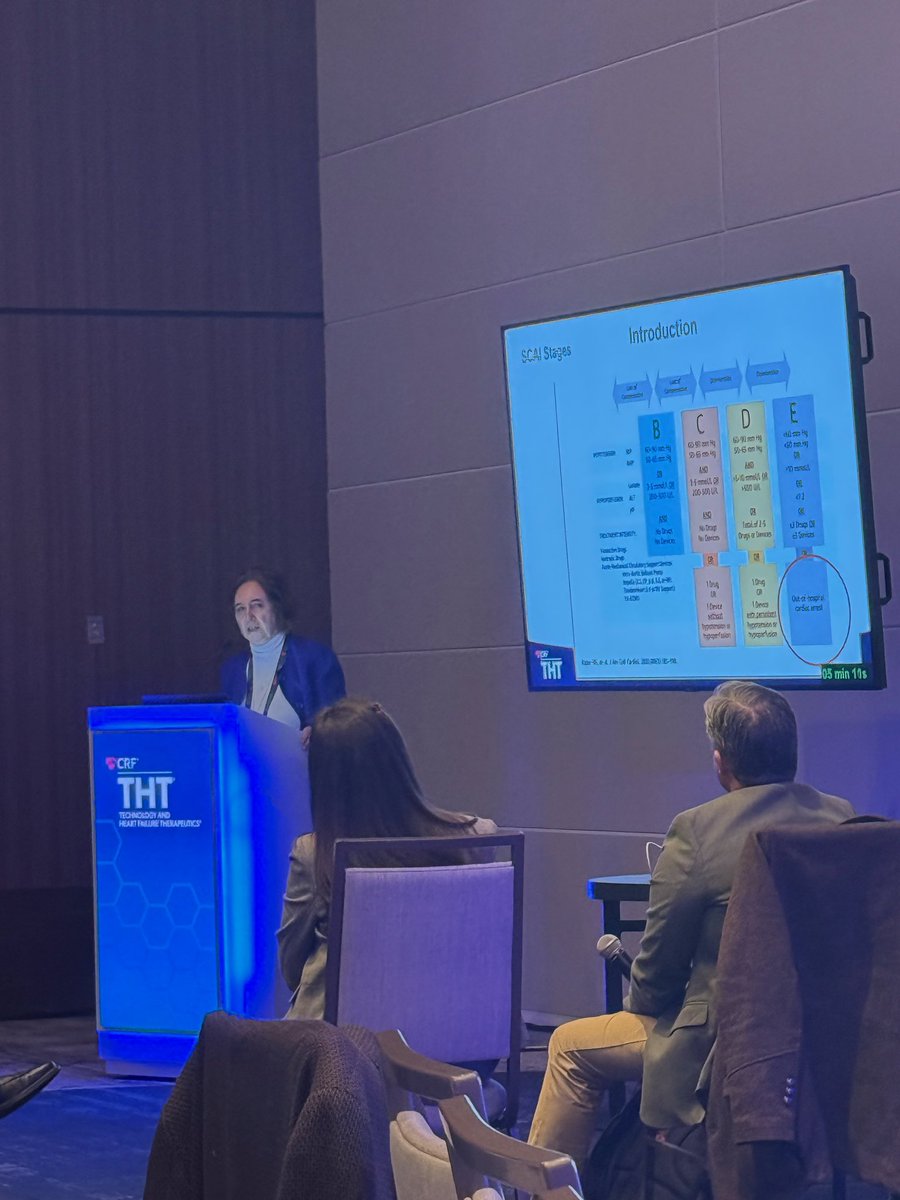
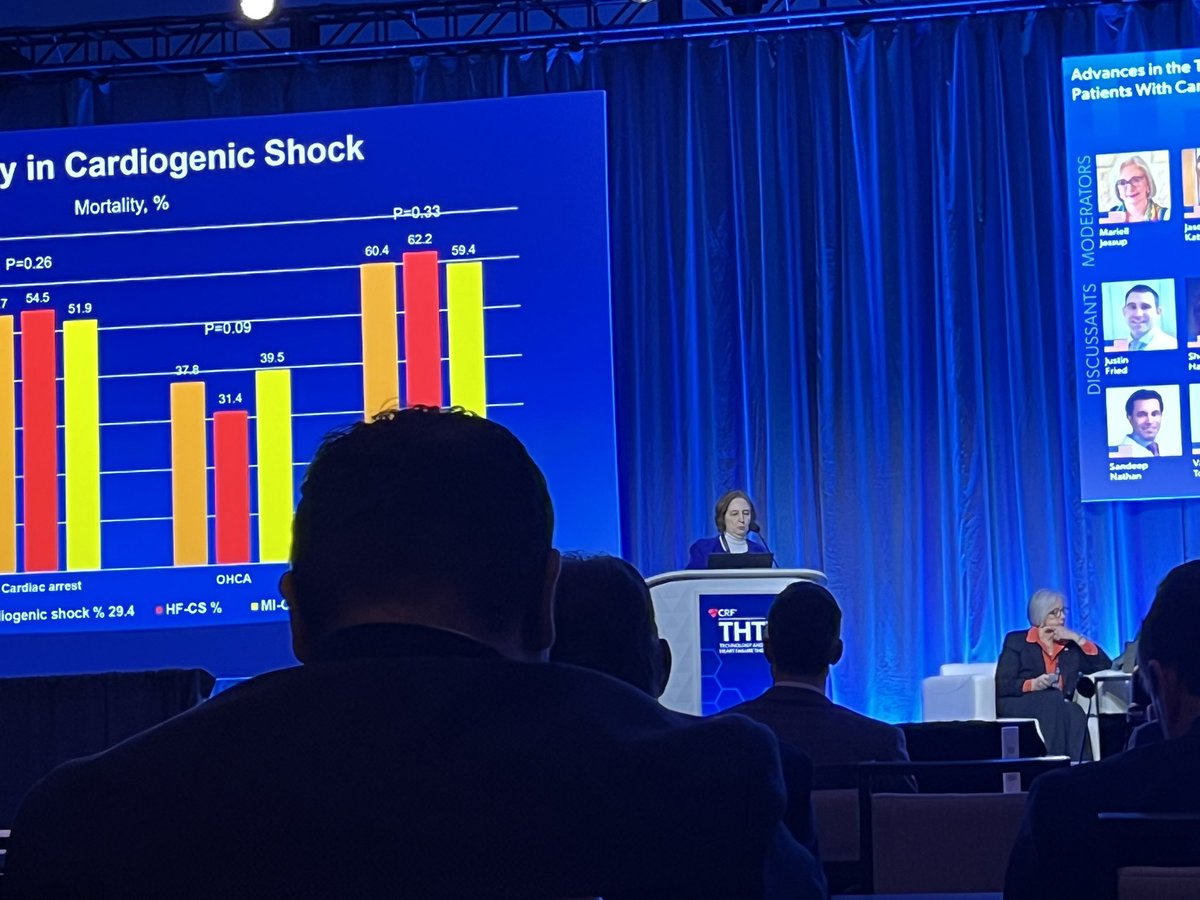
Who agrees with me that in cardiogenic shock each subsequent SCAI stage should carry higher mortality? If yes -why SCAI B is higher than C? I called it the SCAI B mortality pardox- just presented at THT. All hypotheses are welcome!
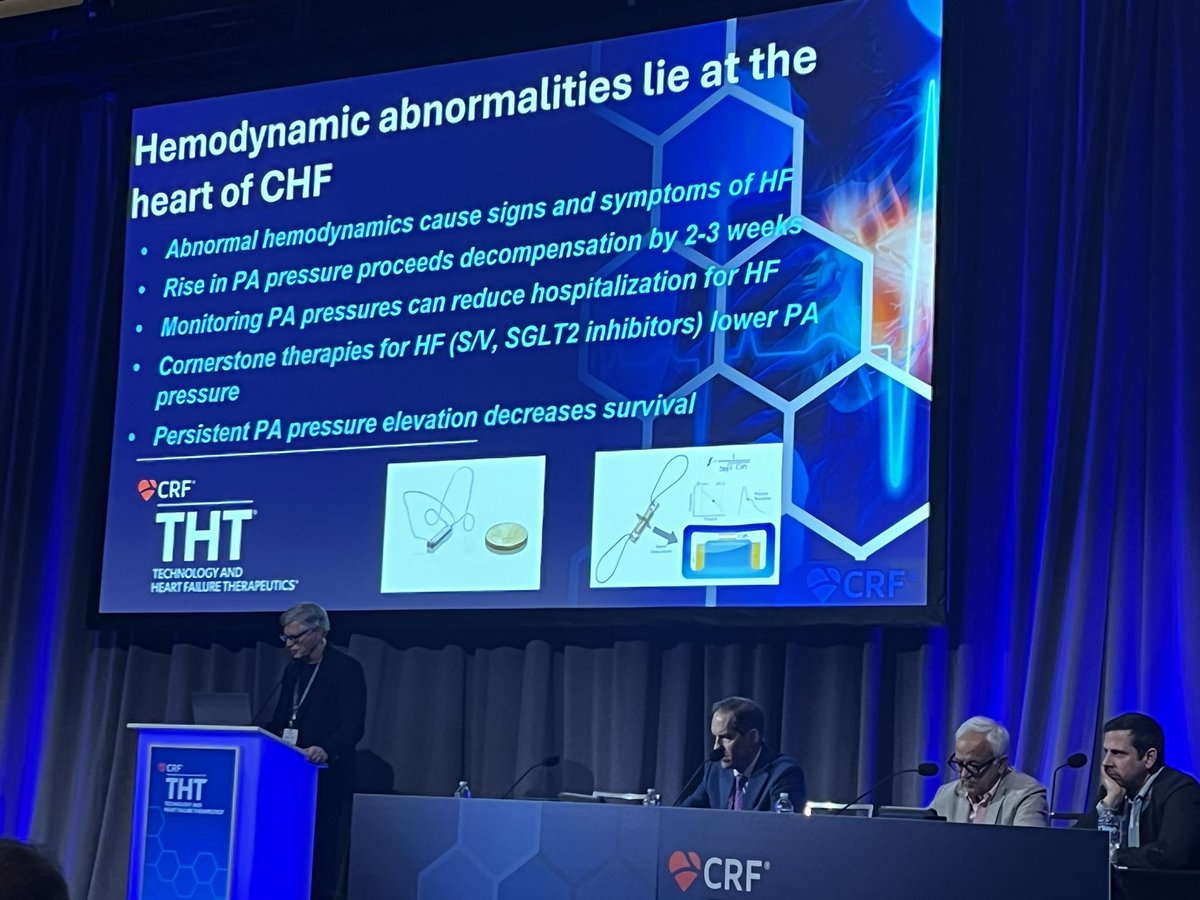
Infarct size is not reduced in patients with anterior #STEMI without shock if they receive a combination of a trans-valvular micro-axial flow pump plus delayed #PCI versus PCI alone, results from the STEMI-Door to Unload trial show. #ACC26 on #CRTonline https://t.co/vGJIQmYi9y
I think all points are well taken. To me, the primary reason - they are not treated, because as soon as they are on any vasopressor or device, they become stage C. The question is - should we use the SCAI classes as stages - and then mortality is expected to increase - or as phenotypes, and then mortality does not have to get progressively worse.
@HoustonShockHSS@BurkhoffMd@CSWorkingGroup@JumeanMarwan@NirUrielMD@Nikhil15
Who agrees with me that in cardiogenic shock each subsequent SCAI stage should carry higher mortality? If yes -why SCAI B is higher than C? I called it the SCAI B mortality pardox- just presented at THT. All hypotheses are welcome!
Not all ICDs in patients with LVAD are futile! We recorded immediate drop in pulmonary pressures and increase in CVP in an LVAD patient who went into ventricular fibrillation, with immediate recovery post defibrillation. Check out our case report! https://t.co/8kGvOuJYzh
The #CSWG was honored to recognize @BurkhoffMd with a Lifetime Achievement Award for his contributions to cardiovascular medicine, heart failure, cardiogenic shock, hemodynamics, and for his humility and mentorship. Thank you Marty Leon for the Keynote! @crfheart@hopkinsheart
Congratulations to our Heart Failure fellow Marcos Molina who mached to the Cardiology fellowship at Rutgers! And yes, we are looking for applicants to our non-ACGME accredited Advanced HF fellowship. If interested, please send you CV to [email protected]. We'll teach you how to care for patients with HF, cardiogenic shock, post-LVAD, and heart transplant. We are in New Brunswick, NJ.
Who agrees with me?
There is a dire shortage of doctors signing up to heart failure fellowships with >60% programs unfilled. I propose the following:
- allow the entry into HF training to general internists—including those who did not match to cardiology
- if they then proceed to cardiology fellowship, allow them to sit for HF Boards after they are Board certified in Cardiology
- If they remain internists with HF training, create an alternative certificate for them.
This would yield immediate benefits:
- all available fellowship slots would be filled with eager and capable trainees
- teaching faculty will be teaching again
- the market will be saturated with HF doctors
Read my whole piece https://t.co/vfzOnCz5vN
@HFSA@JACCJournals@nikhilna@NirUrielMD@Aheartdoc@AHAScience@EMDeFilippisMD@DmitryAbramovMD@EiranGorodeski