Clinical Scientist (HSST) @PublicHealthW - Microbiology. Focusing on #AMR and WGS 🧬 Own opinion only. Fictional cases for education #AMStewardship#MedEd
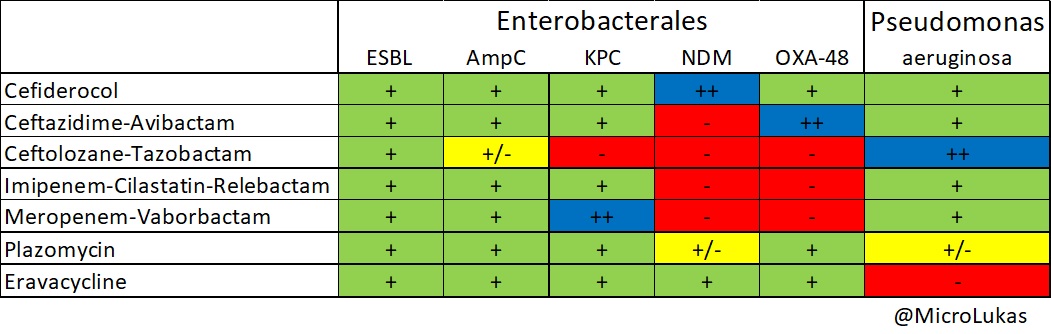
A potentially useful table for anyone interested in understanding the recommended usage of some of the newer antibacterials, e.g. latest beta-lactam/inhibitor combinations.
#AMR#AMS
Q: Which Staphylococcus aureus toxin is responsible for toxic shock syndrome?
A. Exfoliative toxin
B. TSST-1
C. Staphylococcal enterotoxin A
D. Haemolysin
It combines cefepime’s activity against penicillin-binding protein 3 (PBP3) with zidebactam’s selective inhibition of penicillin-binding protein 2 (PBP2).
Mycobacterium leprae ✅
Extremely slow 🦥
Estimated doubling time: ~12-14 days
Cannot be cultured in standard artificial media
Requires intracellular growth in host tissues (e.g., Schwann cells)
Yersinia pestis ❌
Intermediate-fast grower
Doubling time: ~1-2 hours
Grows well on standard media (e.g., blood agar, MacConkey)
Slower than Clostridium perfringens but still a relatively rapid pathogen compared with most bacteria
A neonate presents with meningitis at your hospital.
CSF grows a bacteria with a propensity for abscess formation.
You recommend contrast-enhanced MRI as a result.
Which organism have you seen?
The answer here is Citrobacter koseri.
Why? Because it has a well-known propensity for causing brain abscesses in neonates - far more than most other neonatal meningitis pathogens.
But why isn't the answer K. aerogenes....🧐👇
A neonate presents with meningitis at your hospital.
CSF grows a bacteria with a propensity for abscess formation.
You recommend contrast-enhanced MRI as a result.
Which organism have you seen?
Importantly, manifestations often emerge in the second week of illness.
New focal neurology or seizures in neonatal meningitis should prompt imaging for abscess formation.