I had the honor of speaking at the H&N companion club @IAP_AUS this morning. My colleague @PathCKim captured the moment I realised I couldn’t see the tiny presenter screen 😳 lucky there was a huge screen behind me 🤣 #pathology#gettingold
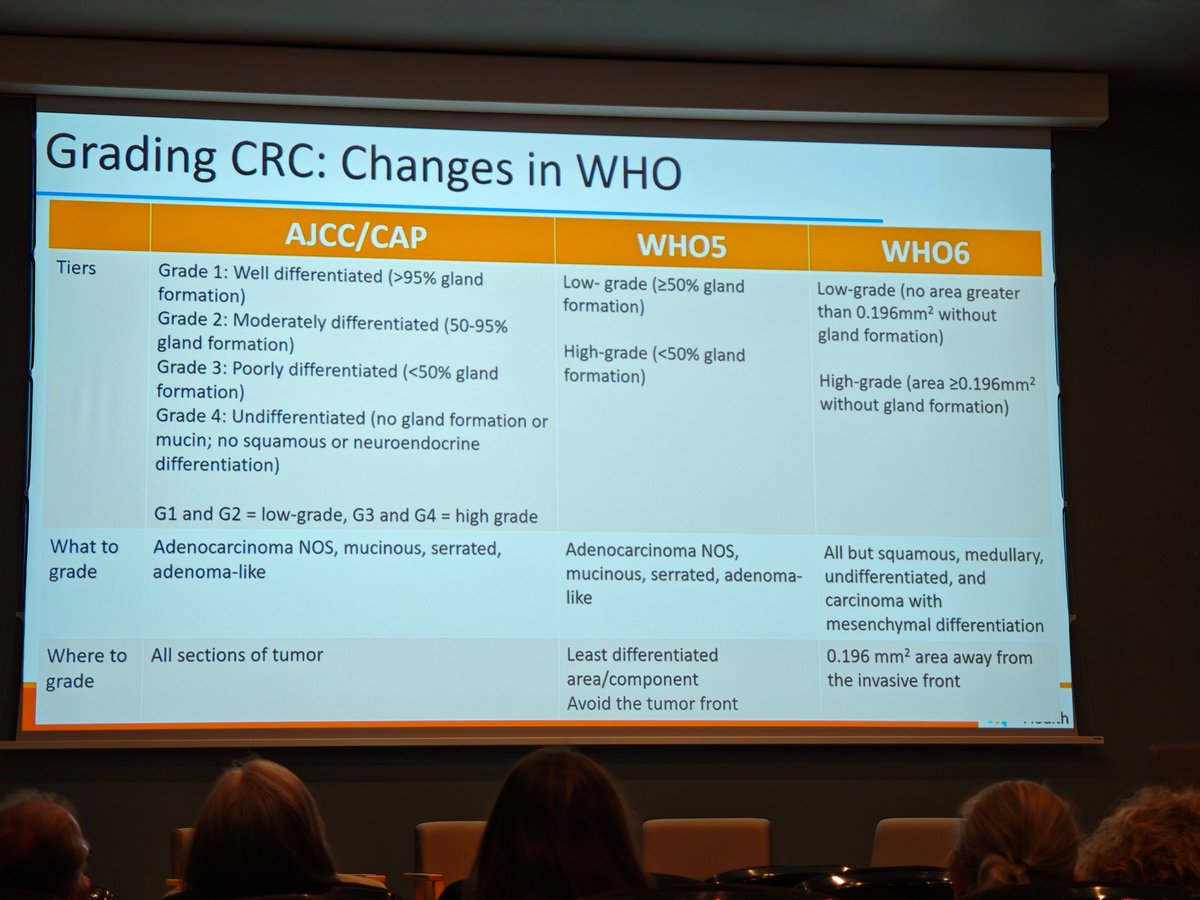
Novelties regarding CRC subtypes and grading in the new 6th edition WHO 📘
Can't help but wonder if anybody is really going to be using this 0.196 mm2 rule.
Dr. Rish Pai, #HMAR_DIGESTIVE26#GIpath#PathTwitter
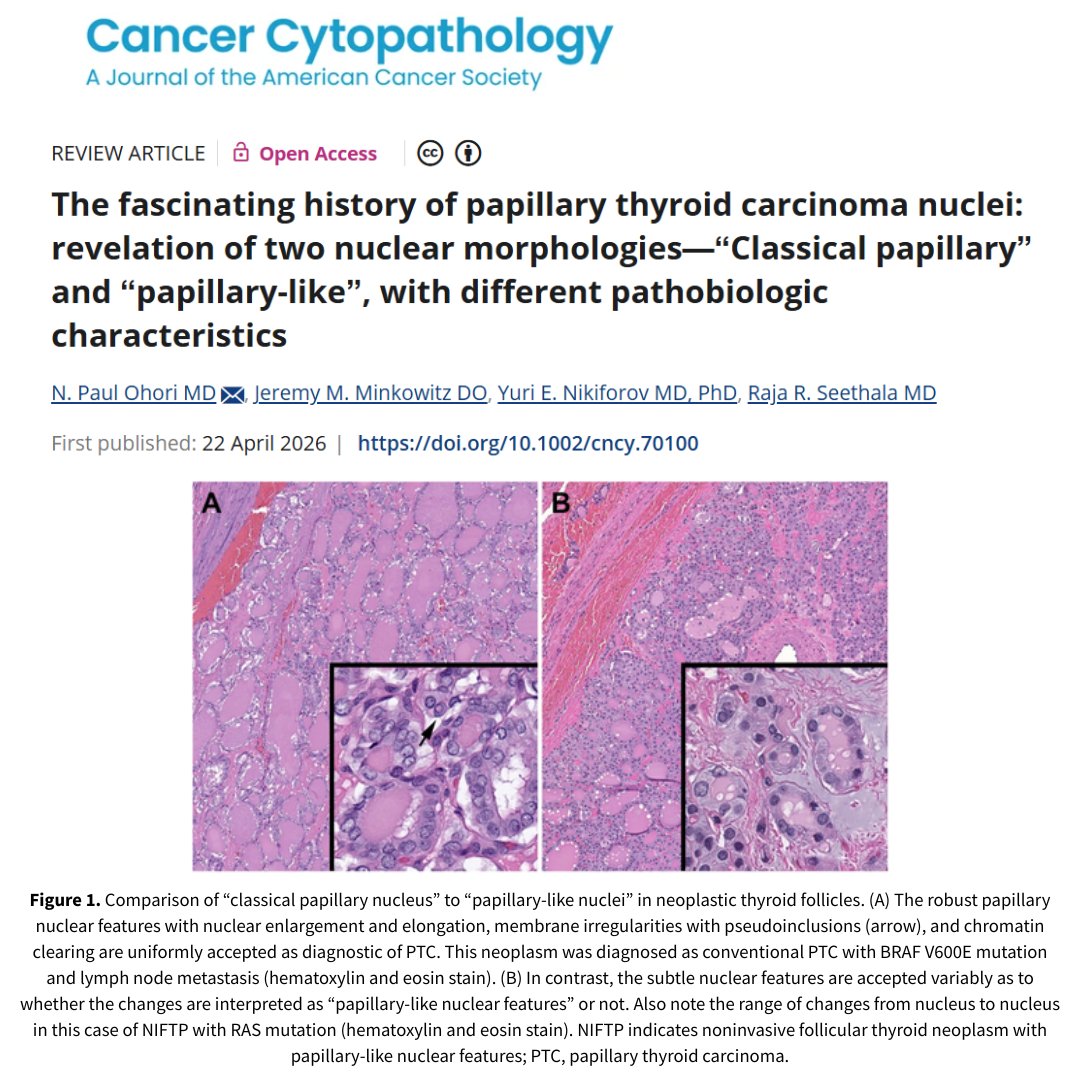
New #OpenAccess review by N. Paul Ohori MD of @UPMCPathology et al details the fascinating history of PTC nuclei & summarizes the major events representing the paradigm shifts, classification system changes, and controversies: https://t.co/wtOPRCUr9M #CytoPath#ENTPath
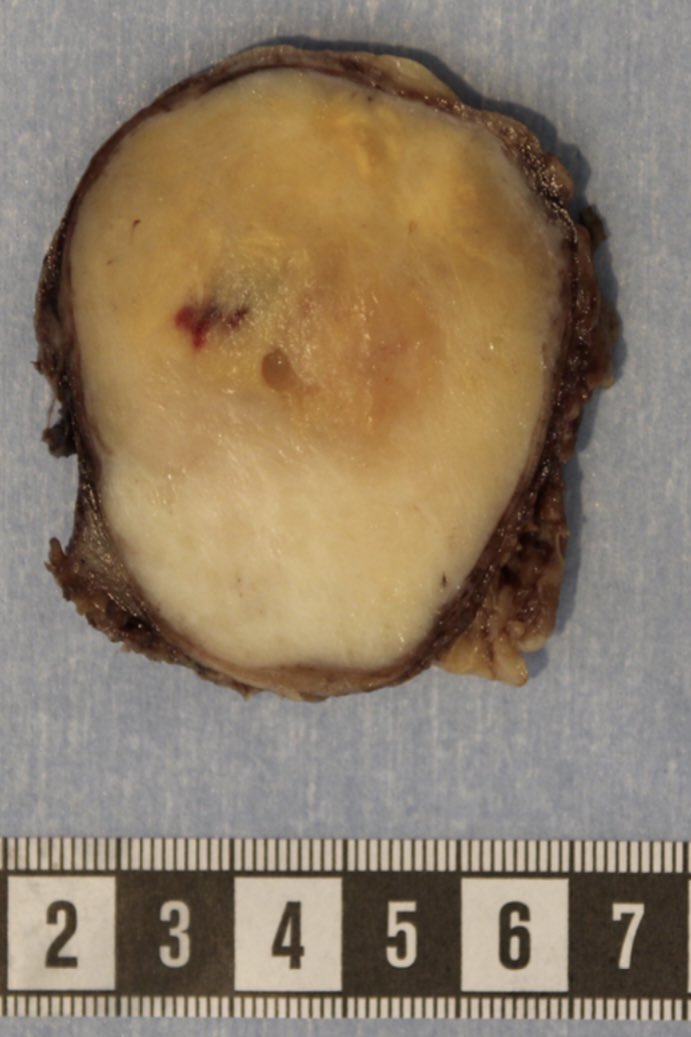
🌸 WTR April Case
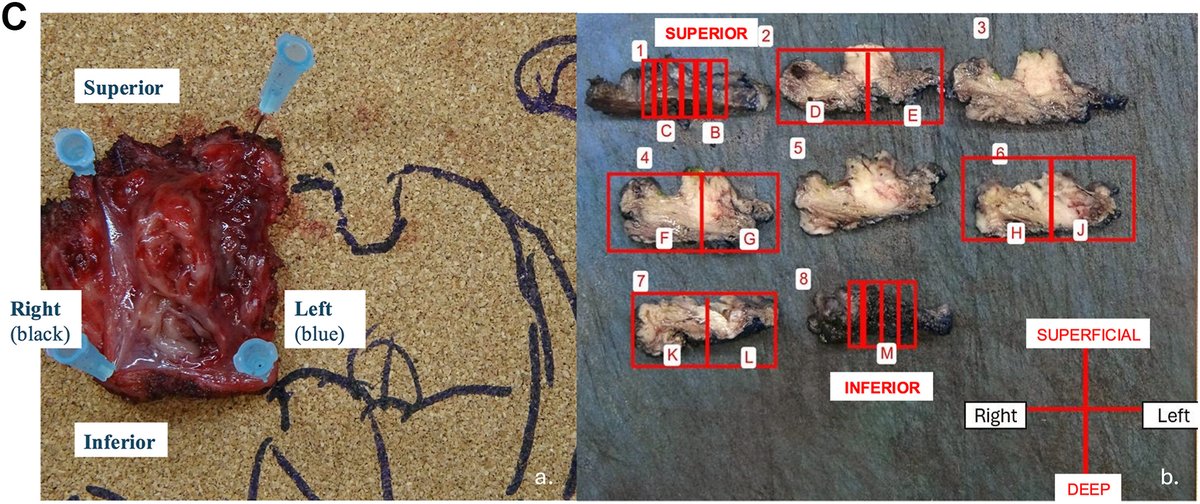
🔬 Case 3: Follicular Thyroid Carcinoma
Encapsulated tumor with capsular invasion, showing macrofollicular architecture with abundant colloid.
👉 https://t.co/zcQxublvXQ
#WorldTumorRegistry#Thyroid#DigitalPathology
Incredibly grateful to be at Asan Medical Center for an observership under Prof. Seung-Mo Hong. Looking forward to three weeks of meaningful learning in #GI/#HPB pathology and #digitalpathology at such a world-class institution!
Extremely rare case of a thyroid FNA in a patient with a history of Alk+ lung adenocarcinoma. An earlier FNA of the adrenal gland showed a mixed small cell-adenocarcinoma with both components staining with TTF-1. The thyroid FNA was predominantly small cell carcinoma with a minute component of adenocarcinoma (red circle) c/w patient's known lung primary.
Nucleolar prominence and relatively abundant cytoplasm clearly favor an oncocytic neoplasm in this thyroid FNA over a medullary carcinoma. Both tumors can have cytoplasmic granularity and isolated plasmacytoid cells. The material at 6 o'clock is colloid and should not be confused with amyloid. Follow-up; "Oncocytic Carcinoma".
A new study compares focus quality across three whole-slide scanners for thyroid cytology! An automated Laplacian variance score helped detect out-of-focus areas, especially in 3-D cell clusters, and may support scanner choice and quality control.
https://t.co/xy7vFW2iOP
A quantitative analysis in Endocrine Pathology reveals that Laplacian variance effectively measures focus quality in digital cytopathology. The study found over 70% of scanned tiles were in-focus, indicating diagnostic usability across scanners.
https://t.co/IbTeHuWwaz
Hello #PathTwitter If you cannot register for this, please do me a favour and like and retweet.
The Australasian Gastrointestinal Pathology society 'AGPS' are hosting the biggest GIT pathology conference ever held in Australasia from 30 October to 1 November 2025.
It's being held right next to Sydney Harbour and is a once in a lifetime opportunity to see the harbur city, discuss GIT pathology, and socialize.
The target audience is general surgical pathologists who report some (or a lot) of GIT pathology, but there will also be plenty for specialty GIT pathologists.
Faculty are flying in from all around the world.
Information and registration at:
https://t.co/vkpt9zd1Uv
Although this thyroid FNA of a papillary carcinoma appears more "columnarish" than "tallish", the resection showed a "Papillary Thyroid Carcinoma, Tall Cell Subtype". I usually do not subtype PTCs on FNA but in aggressive subtypes would mention the finding in a note.
Just a gorgeous "Follicular Neoplasm" on thyroid FNA. As I often say, more important than the microfollicular pattern is the monotony of the follicles. Also seen here are some "flaming" cells (fire flames are by no means specific for Graves' disease).
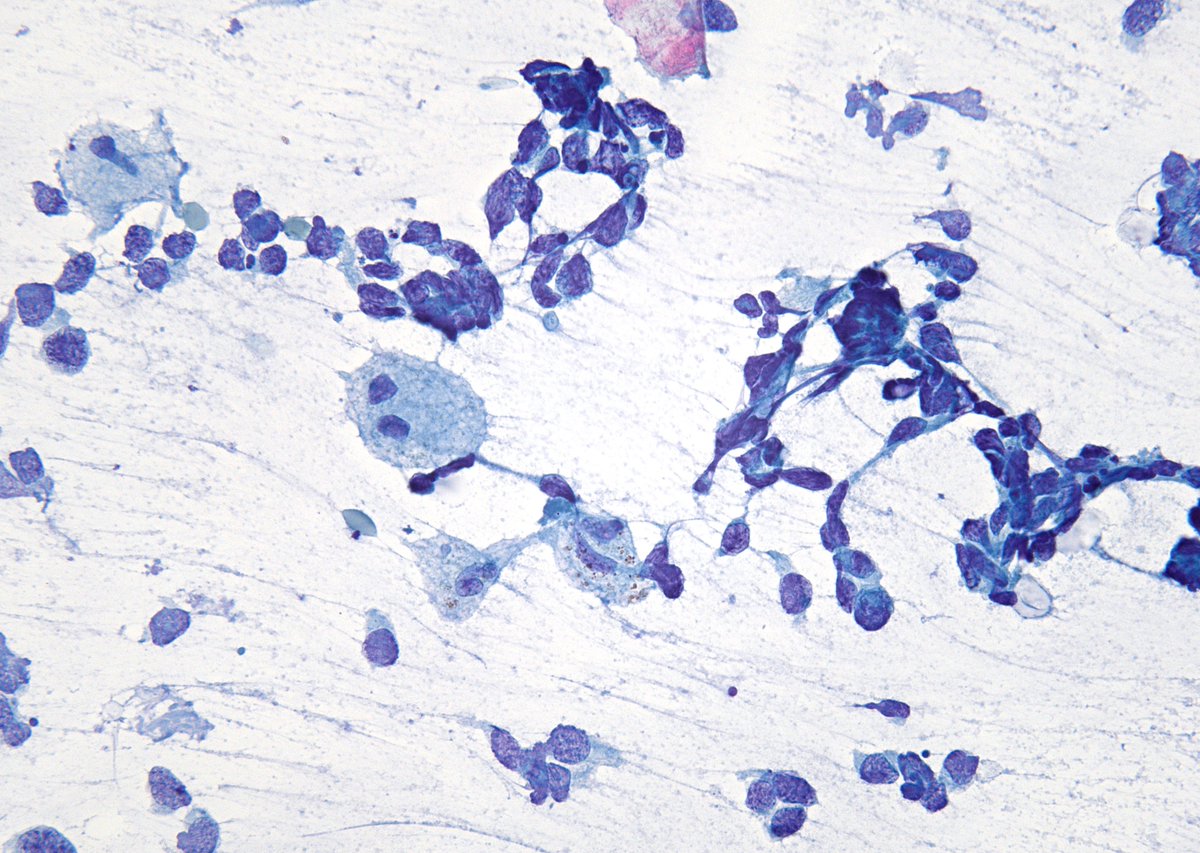
THYROID with metastatic lung "Small Cell Carcinoma". Macrophages provide a good size reference. DD - Medullary CA uncommonly may have a "small cell" phenotype as well as mets from other neuroendocrine tumors (I've seen at least two cases of Merkel cell CA mets to thyroid). (FNA)