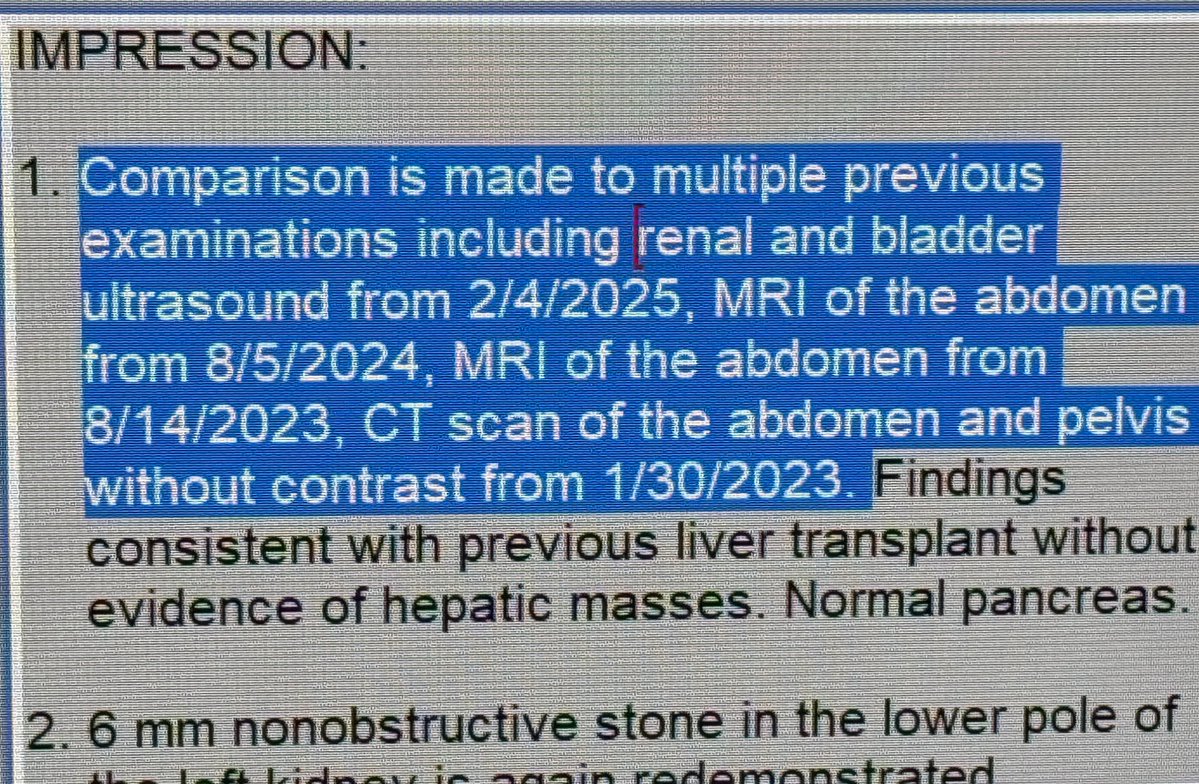
The use of the word “redemonstrated” in a radiology report is associated with higher odds that the imaging study or its prior comparison study was inappropriate/unindicated/low-value/redundant.
I'm heading to SIR this April in Toronto! Looking forward to advancing my knowledge for patients suffering from PAD and carotid disease.
https://t.co/kGlw6t8GXk
#SIR26TOR
Healthcare will make you feel like you're taking crazy pills:
Precertification obtained for standard of care procedure.
Patient has 45 min outpatient procedure. Hospital bills patients insurance $304,713.97 --> roughly $6,700 per MINUTE of procedure time. Itemization is opaque and makes it impossible to understand cost.
Insurance arbitrarily reimburses $16,318.46 for the hospital portion but decides NOT TO PAY THE PHYSICIAN PORTION. No reason given, no mechanism to appeal.
@mcuban@MattHawkinsMD@RichDuszak@SandeepBaglaMD
On a population basis, there are very few interventional radiologists. This effect is only magnified in rural areas like upstate NY! We need more IR doctors.
https://t.co/mJ4dhrECfd
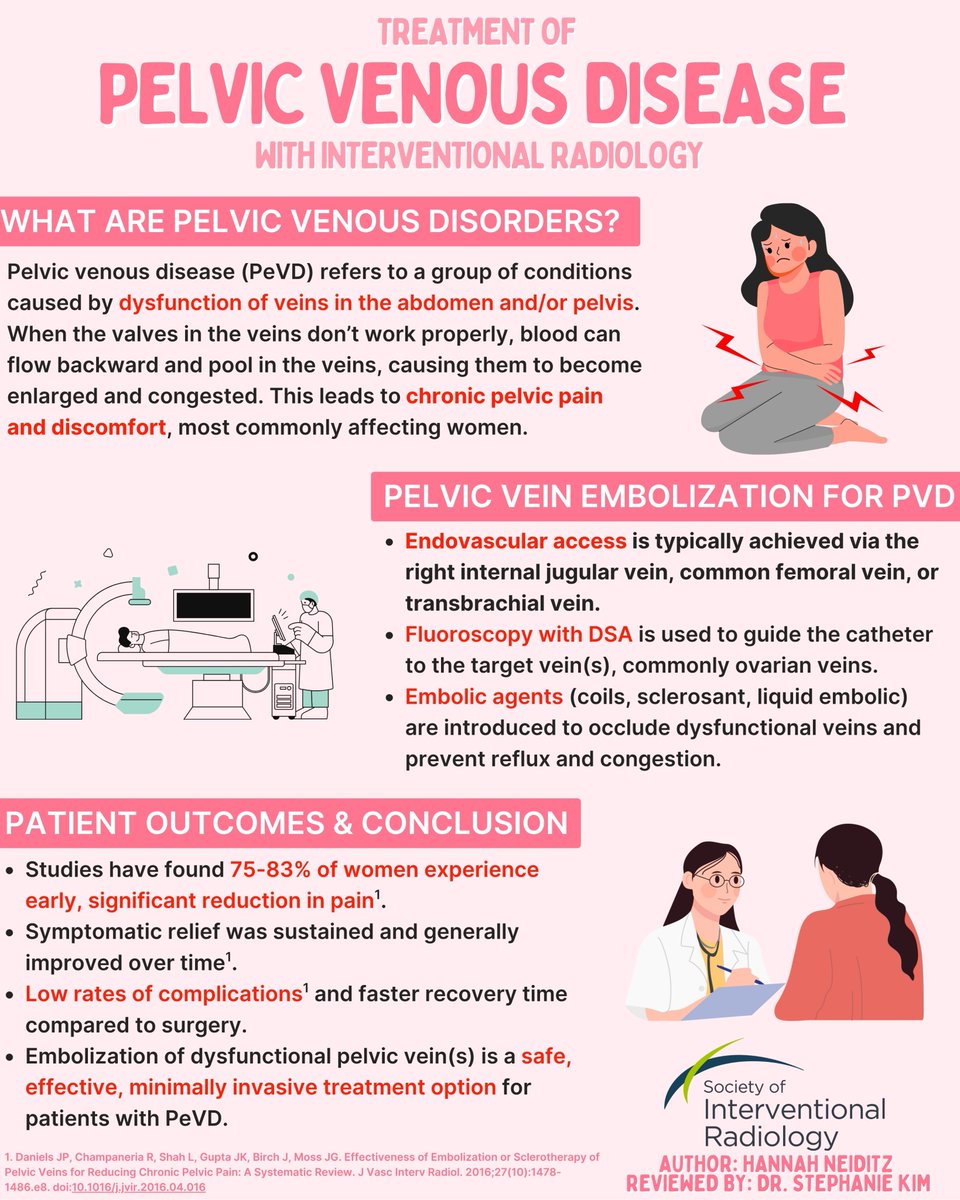
Pelvic Venous Disease affects millions of women worldwide and can lead to debilitating pain. IR can provide an effective minimally-invasive treatment option with faster recovery times compared to surgery. #PelvicVenousDisease#InterventionalRadiology#WomensHealth
Millions suffer from hemorrhoids—IR has a solution. Learn how Hemorrhoidal Artery Embolization treats bleeding hemorrhoids and restores quality of life. #SIR#SIRRFS#InterventionalRadiology#HAE
EMBOLIZE Trial randomized controlled trial in CPP (chronic pelvic pain) is happening. Send any potential subjects to assess! @SIRspecialists@VIVAPhysicians
How can a doctor make money as a clinician without having any ownership of facilities or ancillary services?
Professional fees - where doctors get paid a centrally set rate for seeing patients and doing procedures.
Call coverage - where doctors get paid for taking ER and inpatient consults.
That’s about it. Now what about hospitals?
Facility fees - the facility, be it an ambulatory surgery center or hospital, gets paid substantially more for procedures than the physician does.
Ancillary revenue - labs, imaging, and therapies all generate revenue for hospitals.
340B, tax exemption, GME, local and state subsidies - these are all extra revenue streams for large hospitals that are unavailable to doctors.
Now if doctors want to own, they can buy into surgery centers and ancillary services, but then they must navigate stark and certificate of need laws. They can drop Medicare to open their own hospital, cutting themselves off from other revenue streams.
It’s easy to see how physicians are being locked out of capital and revenue streams. This is by design.