🧬 Obexelimab: A New Way to Control B Cells
Unlike rituximab, which removes B cells, obexelimab functionally silences them by co-engaging CD19 and the inhibitory receptor FcγRIIB (CD32B).
🔹 Inhibits B-cell activation
🔹 Reduces plasmablast formation
🔹 Decreases antibody production
🔹 Suppresses inflammatory cytokines
🔹 Minimal B-cell depletion
Obexelimab turns B cells “OFF” rather than wiping them out, potentially preserving immune function while controlling autoimmune disease.
#RheumattDoc #MedTwitter #RheumTwitter #Medicine #rheumatology @docakx@IhabFathiSulima@CelestinoGutirr@DurgaPrasannaM1
The #EULAR recommendations for the management of Polymyalgia Rheumatica and Large Vessel Vasculitis were presented today at #EULAR2026 at London by the task force lead Dr Chetan Mukhtyar. It was a privilege to represent India on this international task force! I hope these recommendations lead to the better management of patients with PMT, GCA and Takayasu Arteritis. Watch out for the publication of these recommendations in the future!
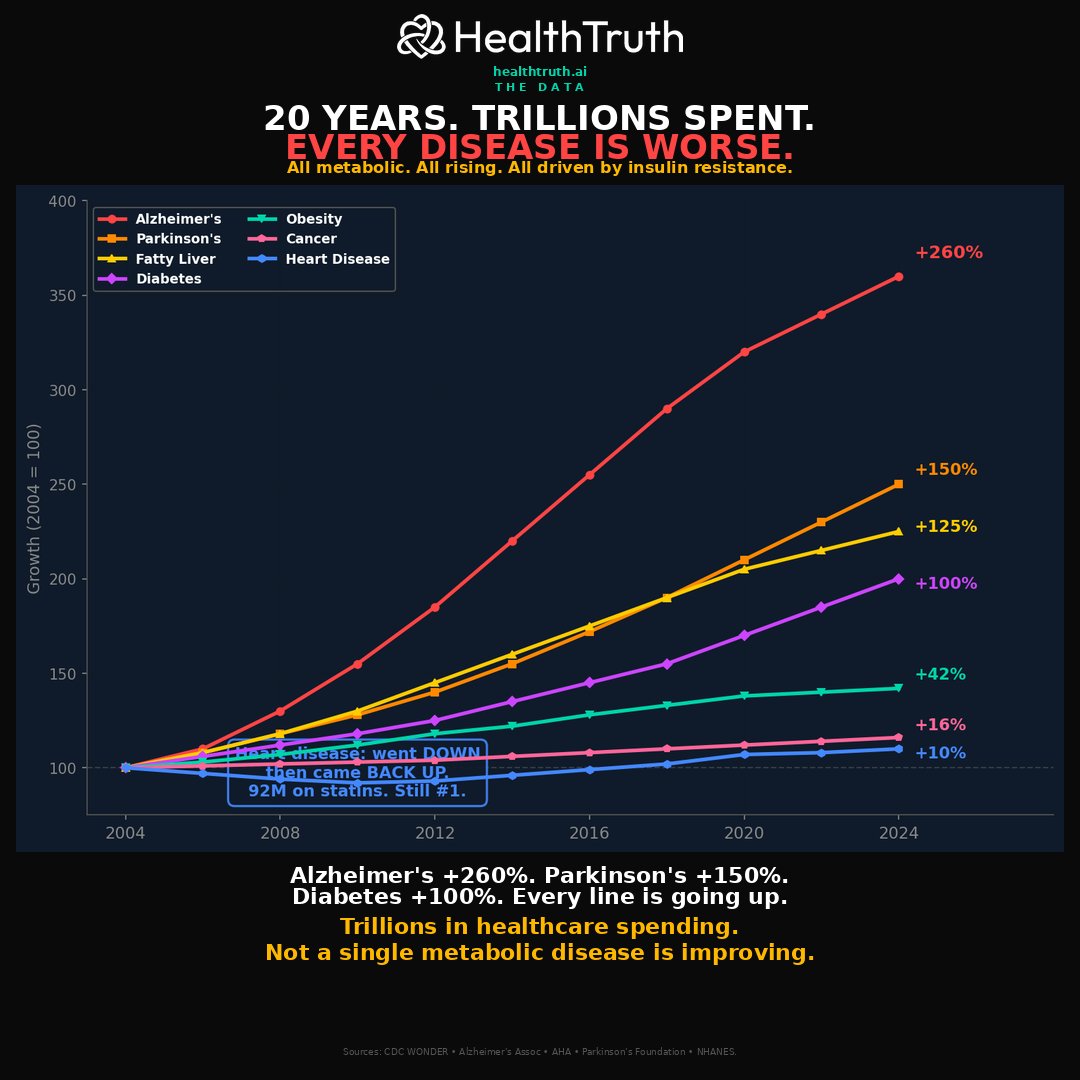
I want you to look at this chart and tell me what you see.
20 years. Seven diseases. Every single line is going up.
Alzheimer's up 260%. Parkinson's up 150%. Fatty liver up 125%. Diabetes doubled. Obesity up 42%. Cancer up 16%. Heart disease went down then came right back up.
Trillions of dollars. The most expensive healthcare system in human history. And not a single metabolic disease is improving.
Something is causing all of them. The same something. And nobody is stopping it.
🧵
شركات الأدوية الكبيرة ما تبيك تعرف عن د. جيسون فنق.
بينما السكري النوع الثاني ومقاومة الإنسولين ينقصون من عمرك سنين...
هو أثبت إنك تقدر ترجعهم لوضعهم الطبيعي بشكل طبيعي وبدون أدوية.
هذي أهم 7 بروتوكولات عنده لعكس مقاومة الإنسولين (احفظها عندك):🧵
🧵 “Doctor, why is my BP still 190/110 despite 4 medicines?”
Because sometimes hypertension is NOT the disease.
It’s the symptom.
Clinical cases that reveal the hidden causes of SECONDARY HYPERTENSION 👇
Fever in lupus is always confusing.
Infection?
Or lupus flare?
And the treatment goes in opposite directions.
More steroids in infection can worsen the patient.
Delaying immunosuppression in severe flare can also be dangerous.
This study looked at something interesting:
DNI (Delta Neutrophil Index)
A parameter automatically generated in some CBC analyzers.
It reflects immature granulocytes in blood.
In simple words:
higher DNI means the marrow is pushing out young neutrophils, usually during infection.
The study showed:
• Infection group had higher DNI
• Lupus flare group had lower DNI
• DNI ≥2.8% strongly favored infection
• Higher DNI increased infection risk nearly 8-fold
Interesting part:
In multivariate analysis, DNI was the strongest independent predictor of infection.
Simple takeaway:
High DNI → think infection
Low C3/C4 → think lupus flare
Many clinicians never notice DNI in CBC reports.
Maybe we should start looking at it more carefully.🤭😊
Los científicos japoneses acaban de descubrir algo inquietante sobre las canas.
Literalmente, es tu cuerpo eligiendo la supervivencia antes que el cáncer.
Aquí tienes todo lo que necesitas saber (y cómo mantener tu cabello oscuro):
🔥 HLH in 2026: The “3 Fs” That Should Trigger Immediate Suspicion
Credits for sharing: Dr. Hind Salama 🌟
⸻
🚨 Suspect HLH When You See the 3 Fs
🔻 Falling blood counts
New or worsening cytopenias involving ≥2 lineages
🌡️ Persistent Fever
Unexplained fever despite broad-spectrum antimicrobials
🩸 Ferritin High
Often >3,000–10,000 µg/L
Extreme hyperferritinemia (>10,000 µg/L) is highly suggestive
⸻
🆕 HLH-2024 Diagnostic Criteria (5 of 7)
The updated criteria simplify diagnosis by removing NK-cell activity testing, which is not widely available.
Diagnosis can be made with:
1️⃣ Fever
2️⃣ Splenomegaly
3️⃣ Cytopenias affecting ≥2 lineages
4️⃣ Hypertriglyceridemia and/or hypofibrinogenemia
5️⃣ Ferritin ≥500 µg/L
6️⃣ Soluble CD25 (sIL-2R) ≥2,400 U/mL
7️⃣ Hemophagocytosis in bone marrow, CSF, or lymph node
📌 Diagnosis = 5 of 7 criteria
⸻
🩸 Cytopenia Thresholds
Hemoglobin <9 g/dL
Platelets <100 × 10⁹/L
ANC <1.0 × 10⁹/L
⸻
🧪 Metabolic Criteria
Triglycerides ≥3 mmol/L (≥265 mg/dL)
Fibrinogen <1.5 g/L
⸻
🔬 Why HLH-2024 Matters
✅ Removes NK-cell function testing
✅ Retains excellent diagnostic performance
✅ More practical for real-world adult hematology practice
⸻
📊 HScore Remains Useful in Adults
Interpretation:
<90 → low probability
90–169 → intermediate
≥169 → high probability of HLH
⸻
🧠 Clinical Pearls
💡 Hemophagocytosis is not required and may be absent early.
💡 Ferritin >10,000 µg/L strongly supports the diagnosis but is not specific.
💡 Start treatment when suspicion is high—do not wait for all tests.
💡 Always search for the trigger: infection, lymphoma, autoimmune disease, or cellular therapy.
⸻
❓ MCQ
Which parameter was removed from HLH-2024 criteria?
A. Ferritin
B. Soluble CD25
C. NK-cell activity
D. Splenomegaly
✅ Answer: C. NK-cell activity
⸻
🩺 OSCE Scenario
A 42-year-old patient with lymphoma has persistent fever, splenomegaly, Hb 7.8 g/dL, platelets 45 × 10⁹/L, ferritin 18,000 µg/L, fibrinogen 0.9 g/L, and sCD25 9,000 U/mL.
Perfect Answer
“This patient fulfills HLH-2024 criteria with fever, splenomegaly, bicytopenia, hypofibrinogenemia, elevated ferritin, and elevated soluble CD25. This is secondary HLH, likely lymphoma-associated, and treatment should begin urgently while addressing the underlying lymphoma.”
⸻
📌 Bottom Line
🔥 Think HLH = 3 Fs
Falling counts
Persistent Fever
Ferritin High
🩸 HLH-2024 uses 5 of 7 criteria.
⏳ Early recognition and treatment save lives.
⸻
Key Reference
Blood 2024: Diagnostic Guidelines for Familial Hemophagocytic Lymphohistiocytosis Revisited
#HLH #HemophagocyticLymphohistiocytosis #Ferritin #HScore #Lymphoma #EBV #Hematology #KFSHRC #SSBMT2026
A high CK is not the diagnosis.
It is only the entry ticket.
Inflammatory myopathy should be approached by pattern first, not by calling everything polymyositis.
First, look at the weakness.
Slow, asymmetric weakness with finger flexor and quadriceps involvement
Think inclusion body myositis.
Rapid proximal weakness with a CK volcano
Think immune mediated necrotizing myopathy, especially anti HMGCR or anti SRP.
Subacute proximal weakness with mechanic’s hands, Raynaud’s, arthritis or ILD
Think antisynthetase syndrome, especially anti Jo 1, PL 7 or PL 12.
Rash with or without weakness, sometimes even with normal CK
Think dermatomyositis, especially MDA5, TIF1 gamma, NXP2, Mi 2 or SAE.
Antibodies are powerful, but only when the phenotype agrees.
MRI tells you activity versus damage.
Biopsy still matters in seronegative cases, suspected IBM, poor steroid response or dystrophy mimics.
The real mistake is stopping at muscle.
Always ask about:
lung, skin, swallow, heart and cancer risk.
Myositis is not one disease.
It is a pattern recognition exam where the wrong lane can cost muscle, lung and time.
Pattern first.
Antibody next.
Biopsy when needed.
Screen beyond muscle.
Treat the subtype, not the CK.
#Neurotwitter #Medtwitter
Source: Allenbach Y, Benveniste O. Inflammatory Myopathies. NEJM, 2026.
🚨 81 scientific studies confirm that exercise is the most powerful cardiovascular drug ever discovered.
Most cardiologists never prescribe it.
But the data says otherwise.
I am a cardiologist.
I have seen patients reverse hypertension, cut their heart attack risk in half, and extend their lives by years.
Not with a pill. With a structured exercise prescription.
Here is what the science actually says.
💓 The cardiovascular data is staggering.
✅ HERITAGE FAMILY STUDY (aerobic training): VO2 max increased 17% in 20 weeks
✅ LOOK AHEAD TRIAL (lifestyle intervention): cardiovascular risk factors dropped significantly in patients who exercised consistently
✅ INTERHEART STUDY (physical activity): regular exercise reduced heart attack risk by 35%
✅ META-ANALYSIS OF 81 STUDIES (exercise as medicine): aerobic exercise reduced all-cause mortality by 31% and cardiovascular mortality by 35%
That matters because no single drug on the market matches that mortality reduction across a population.
🔬 What exercise actually does to your heart:
Lowers resting heart rate
Reduces systolic blood pressure by 5 to 8 mmHg
Increases stroke volume and cardiac output
Reduces LDL and triglycerides
Increases HDL
Improves endothelial function and arterial compliance
Reduces chronic inflammation
Lowers visceral adiposity
These are not soft endpoints. These are the exact mechanisms that kill you when they go wrong.
🩺 The exercise prescription the data supports:
150 to 300 minutes of moderate intensity aerobic exercise per week
2 to 3 sessions of resistance training per week
Zone 2 cardio as the foundation. Think brisk walking, cycling, swimming at a pace where you can still hold a conversation.
High intensity interval training added on top for VO2 max gains.
Consistency over 8 to 12 weeks before you measure results.
⚠️ What most people get wrong:
They treat exercise as optional.
They start too hard and quit in two weeks.
They skip resistance training entirely.
They never track their resting heart rate or blood pressure to see the data working.
❌ A 30-minute walk three times a week will not cut it if you are high risk.
❌ Weekend warrior patterns will not replace daily movement.
❌ Cardio alone without resistance training leaves you metabolically exposed.
"The tools with the strongest data are unsexy, free, and require your participation."
A patient who commits to 180 minutes of aerobic exercise and 2 resistance sessions per week can lower their blood pressure by 7 mmHg and reduce their cardiovascular event risk by up to 35% in 12 weeks.
That is the difference between managing disease and reversing it.
❤️ Bottom line:
Exercise is not a lifestyle suggestion. It is the most evidence-backed cardiovascular intervention in the history of medicine.
81 studies. Hundreds of thousands of patients. The data is not ambiguous.
Get your heart rate up 5 days a week. Lift weights twice a week. Track your resting heart rate. Give it 12 weeks.
The question is no longer whether exercise helps your heart. The question is why your doctor has not written you a prescription for it yet.
Are you treating exercise like medicine, or like an option?
#Cardiology #HeartHealth #HeartDisease #CardiovascularHealth #ExerciseIsMedicine #VO2Max #CardiacRehab #MetabolicHealth #PreventiveCardiology #LifestyleMedicine
Big Pharma doesn't want you to know about Dr. Jason Fung.
While Type 2 Diabetes and insulin resistance take years off your lifespan...
He's proved you can reverse them naturally without meds.
Here are his top 7 protocols to reverse insulin resistance (bookmark this):🧵
Listening to Lupus: A Rheumatologist’s Perspective 💜
Living with lupus is not just about medicines or hospital visits. It is about living every day with uncertainty.
In my practice in North India, I see young women—students, mothers, professionals—struggling with fatigue that others can’t see, pain that is often dismissed, and symptoms that come and go unpredictably. Many patients spend months, sometimes years, moving from one doctor to another before getting the right diagnosis.
Lupus affects more than the body. It affects confidence, careers, relationships, and mental well-being. Families also go through silent stress—trying to understand a disease that has no fixed pattern, supporting a loved one through flare-ups, and managing long-term treatment costs.
In our setting, the challenges are deeper and very specific to lupus. Awareness about Systemic Lupus Erythematosus (SLE) remains limited, so early symptoms—persistent fatigue, joint pains, skin rashes, hair fall—are often overlooked or misattributed. Many patients are initially treated for infections, anemia, or “general weakness,” leading to significant delays in diagnosis.
Social stigma adds another layer—especially for young women—impacting education, employment, and even marriage prospects. Access to specialized rheumatology care is still limited in many areas, and the need for long-term follow-up, regular investigations, and immunosuppressive therapy creates both emotional and financial strain for families.
As a result, patients often reach us late, sometimes only after major organ involvement like kidney disease or severe flares—when timely intervention could have changed the course of illness.
But there is hope.
With early diagnosis, regular follow-up, and the right treatment, patients with lupus can lead meaningful, productive lives. What they need most is awareness, understanding, and timely care.
As a rheumatologist, I believe our responsibility is not just to treat, but to listen, educate, and support—both patients and their families.
Let’s make lupus visible. 💜
#MakeLupusVisible #LupusAwareness #Rheumatology
Editorial
Collagen Turnover Biomarkers in Systemic Sclerosis: Can We Capture the Full Fibrotic Process From the Blood?
📖 https://t.co/vsvLz9fVUX
@UZH_ch@MurielElhai#Fibrosis#SystemicSclerosis