💊 Perioperative antiplatelet management is not “stop aspirin 7 days before surgery.”
It is a balance between surgical bleeding and catastrophic arterial thrombosis.
Recent PubMed indexed guidance is clear: in non cardiac surgery, the highest risk patient is not the one taking aspirin. It is the patient with a recent coronary stent, recent ACS, recent stroke, or high thrombotic burden in whom interruption of antiplatelet therapy may trigger myocardial infarction, stent thrombosis, or stroke (Thompson et al., 2024; Douketis & Spyropoulos, 2023).
For elective surgery, timing matters. After PCI, elective non cardiac surgery should ideally be delayed until the minimum recommended DAPT period is completed. If surgery cannot wait, aspirin should usually be continued when bleeding risk is acceptable, especially in patients with coronary stents. P2Y12 interruption, when necessary, should be as short as possible: clopidogrel usually 5 days, ticagrelor 3 to 5 days, and prasugrel 7 days before surgery (Thompson et al., 2024; Swan et al., 2024).
Emergency surgery is different. The decision becomes procedural urgency, bleeding site compressibility, last dose, platelet function recovery, and whether the antiplatelet effect can be tolerated. Platelet transfusion may partially reverse irreversible agents such as aspirin and clopidogrel, but it is much less reliable for ticagrelor because circulating drug can inhibit transfused platelets (Swan et al., 2024).
Recent evidence also challenges dogma. In stable patients with previous drug eluting stents undergoing low to intermediate risk non cardiac surgery, aspirin continuation did not clearly reduce ischemic events compared with temporary interruption, although minor bleeding increased (Kang et al., 2024). This does not mean “stop aspirin in everyone.” It means individualize.
The practical question is not:
“Should antiplatelets be stopped?”
It is:
What is more dangerous for this patient: bleeding today, or thrombosis tomorrow?
#Anesthesiology #PerioperativeMedicine #Cardiology #AntiplateletTherapy #Aspirin #Clopidogrel #Ticagrelor #Prasugrel #NonCardiacSurgery #PatientSafety
References 📚
Douketis, J. D. NEJM Evidence, 2(6). https://t.co/zms5Bz8MAE
Kang, D. Y. Journal of the American College of Cardiology, 84(24), 2380–2389. https://t.co/p9iMZBqx7M
Swan, D., Research and Practice in Thrombosis and Haemostasis, 8(6), 102548. https://t.co/61A5TyzWbO
Thompson, A., Journal of the American College of Cardiology, 84(19), 1869–1969. https://t.co/ExOBujTyfY
#ASCO26#AML#leusm
Does venetoclax duration matter in frontline HMA+Ven for AML?
Poster: In a @MayoCancerCare analysis of 540 newly diagnosed AML patients, outcomes were driven primarily by disease biology, not venetoclax duration. Led by Dr. Naseema Gangat 👏👏👏
🔹 Similar OS across 7-, 14-, 21-, and 28-day schedules
🔹 Comparable outcomes within ELN 2024 and Mayo genetic risk groups
🔹 Higher early mortality with shorter durations likely reflected selection of frailer patients
🔹 In ELN high-risk AML, 14-day venetoclax was associated with inferior survival compared with 21- and 28-day schedules
Take-home: Venetoclax duration should be individualized based on genetics, response, cytopenias, and patient fitness rather than a one-size-fits-all approach.
Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
HR SMM, "peripheral neuropathy (20%), mostly grade 1–2 and 1 case of GBS". This seems really high for a patient population that has not received any prior treatment....Grade 1/2 neuropathy can have unporportional impairement on QoL.
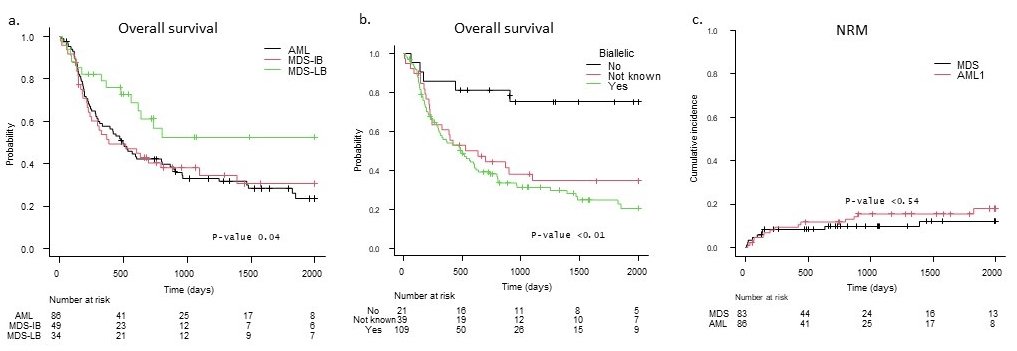
I look forward to this very important presentation in #EHA2026 about value of transplant in TP53 mutated #MDSsm and #AMLsm. The results clearly indicate a tail at end of curve and around 20% 23-year OS even among biallelic TP53mut patients, and especially in those with lower blast counts. Do NOT deprive patients from the opportunity of transplant without a very well-informed discussion!
Patients with KPS >80 had an estimated 3-year OS of 49.3%, compared with 30.2% for KPS ≤80. Biallelic TP53 was associated with inferior survival (HR 4.05, 95% CI 1.76–9.32; p=0.001) (figure 1b), reaching statistical significance only in the MDS subgroup. A low blast count at diagnosis was associated with improved survival (HR 0.50, 95% CI 0.29–0.88; p=0.02).
No clear associations were observed for age, HCT-CI, donor type, conditioning intensity or ATG. NRM did not differ significantly between MDS and AML (figure 1c).
ALLOGENEIC HSCT FOR TP53-ABERRANT MYELOID NEOPLASMS: REAL-WORLD... - Myhre A - EHA-6995 - Jun 13 2026
These are really challenging times for academic medicine. You have to set your goals. If you want to be at the top of the field what matters is truly enduring contributions that help improve patient outcomes. Visibility, titles, fame are transient. Enduring contributions to your field or to the delivery of excellent care at your own institution will set you apart.
Success in any field needs a huge amount of hard work, talent, perseverance, and yes, luck. You need to want to do what you are doing. Passion.
Whether your efforts are in research, practice or education, what will set you apart is always hard work, talent, and perseverance. With that luck is more likely to be on your side.
The American Heart Association mourns the passing of the legendary cardiologist Eugene Braunwald, M.D., widely recognized as one of the most influential figures in the history of cardiovascular medicine. Over seven decades, his work reshaped the understanding and treatment of heart disease, leading many to call him the father of modern cardiology.
Braunwald was a lifelong contributor to the American Heart Association, helping advance its research and scientific mission, and was honored with some of the Association’s highest honors for his lasting influence on cardiovascular care and research. His influence extended well beyond his own discoveries, as generations of Association‑supported investigators, clinicians and academic leaders were trained by Braunwald or guided by the clinical trial standards and mentorship models he helped establish.
https://t.co/ieZuHYMyOP
Many leaders in medicine are focused on AI and how it’s going to solve problems in medicine. Maybe.
But doctors with great clinical acumen, empathy, and the wisdom to make the right judgment call are the ones we need more of, and who patients want and seek out. This is the important stuff.
Honourable Sirs @TelanganaCMO@PMOIndia,
Lost my brother today to Paraquat poisoning. It’s terrifyingly lethal and widely misused for self-destruction. Shocked by how easily it is available everywhere. Doctors are overwhelmed by the amount of cases.Please ban it ASAP-save lives🙏🏽
We have come a long way in myeloma and we are on the threshold of saying it may be a curable disease.
We have come a long ways in myeloma that we may even be able to use a strict definition to identify patients who are potentially cured.
Thanks to @Myeloma_Society for giving me the opportunity to present at the Cure summit. @NikhilMunshiMD@myelomaMD@thanosdimop@mvmateos@SagarLonialMD@IMFmyeloma
We have now 3 CT with T-cell redirecting therapy vs. Triples in 1-3 prior LOT in MM with OS superiority. I don't consider acceptable to start randomized trials with DPd/Kd/EPd/etc control when we have proven superior "established therapy with clinical benefit". #mmsm
Our loyalty is to our patients, not our treatments. Defining ourselves by the treatment we administer blurry our reasoning, bias our research, delays the progress. We can be proud of the skills we acquire, but need to be ready to let them go as the field moves forward. #mmsm
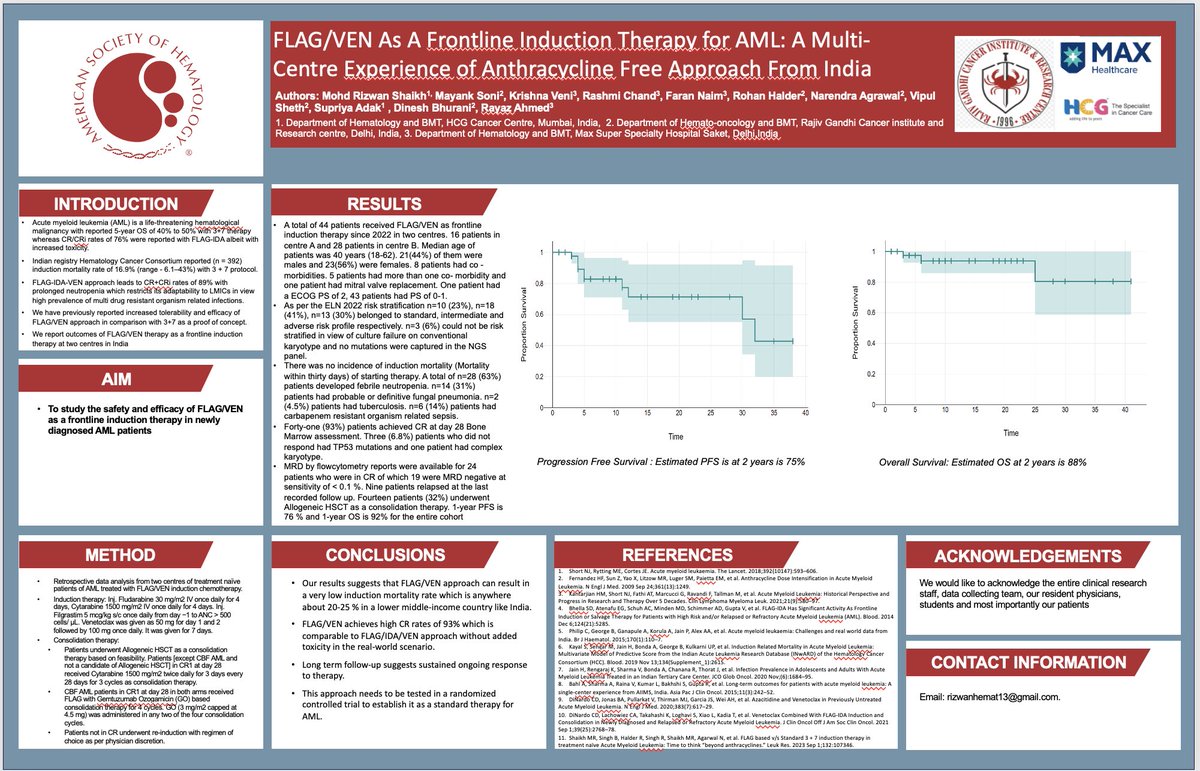
It’s an honour to be part of this collaborative effort aimed at improving outcomes in newly diagnosed fit AML patients from India
n = 44
Median age = 40y
Standard risk 23%
Intermediate risk 41%
Adverse risk 30%
Induction mortality = 0
CR rates = 93 %
PFS 2y = 75 %
OS 2y = 88 %