The National Screening Committee leaned heavily on the new SCHARR prostate cancer screening model in their recent draft recommendations.
In the SCHARR report, the “familial risk” group is defined very broadly — essentially any first-degree relative with breast, ovarian or prostate cancer at any age. In practice, that creates a group that is much larger and less high-risk than many clinicians mean when they say “high-risk family history”.
Why does that matter?
Because if you define high-risk too widely, you dilute the risk signal. You end up screening a big cohort whose average risk is only modestly elevated, and unsurprisingly the model will show:
•more men entering the pathway
•more tests, MRIs and biopsies
•more “extra” cancers detected
•but only a modest increase in deaths prevented per 1,000 screened
That doesn’t tell us much about the group we actually worry about clinically — men with genuinely strong family histories, such as:
•≥1 first-degree relative with prostate cancer diagnosed <60
•≥2 first-degree relatives affected
•aggressive disease clustering / multiple affected relatives
•families with known pathogenic variants (BRCA2, Lynch syndrome, CHEK2 etc.)
Those men often have a much clearer risk elevation (and a different harm–benefit balance) than “any first-degree relative with any of three cancers, any age”.
SCHARR have chosen to model a different question than the one most urologists are actually trying to answer in practice:
“Should we screen a very large ‘mildly higher risk’ group?”
rather than
“Should we offer a risk-targeted programme to truly high-risk families?”
If the familial subgroup includes ~a third of men in their late 50s/early 60s (as the model implies), it’s no surprise that “familial screening” looks only slightly better than population screening. That’s a definitional artefact as much as a finding.
What would be more clinically useful?
A tiered approach, e.g.:
•Moderate FH: one first-degree relative with CaP any age
•High FH: CaP <60 in a first-degree relative, or ≥2 first-degree relatives, or dense clustering
•Very high FH / genetic: BRCA2, Lynch, CHEK2 and similar variants
Then we can ask sensible policy questions: does screening make sense in the high and very high tiers, where absolute risk is higher and where a modern MRI-first pathway may have a better harm–benefit profile?
It is great that the NSC is considering modelling evidence — but the modelling needs clinically realistic risk definitions. Otherwise “high risk” becomes “slightly above average”, conclusions about targeted screening risk being unduly pessimistic and many of those men truly at risk will lose the opportunity of earlier cancer detection.
Brilliant news. Not full screening for every man yet, but a genuine step in the right direction. The extra £18m for the TRANSFORM trial will help find the best way to screen men for prostate cancer, with all eligible Black men aged 45 to 74 invited to take part. Not a national programme, but excellent progress. Well done to all involved.
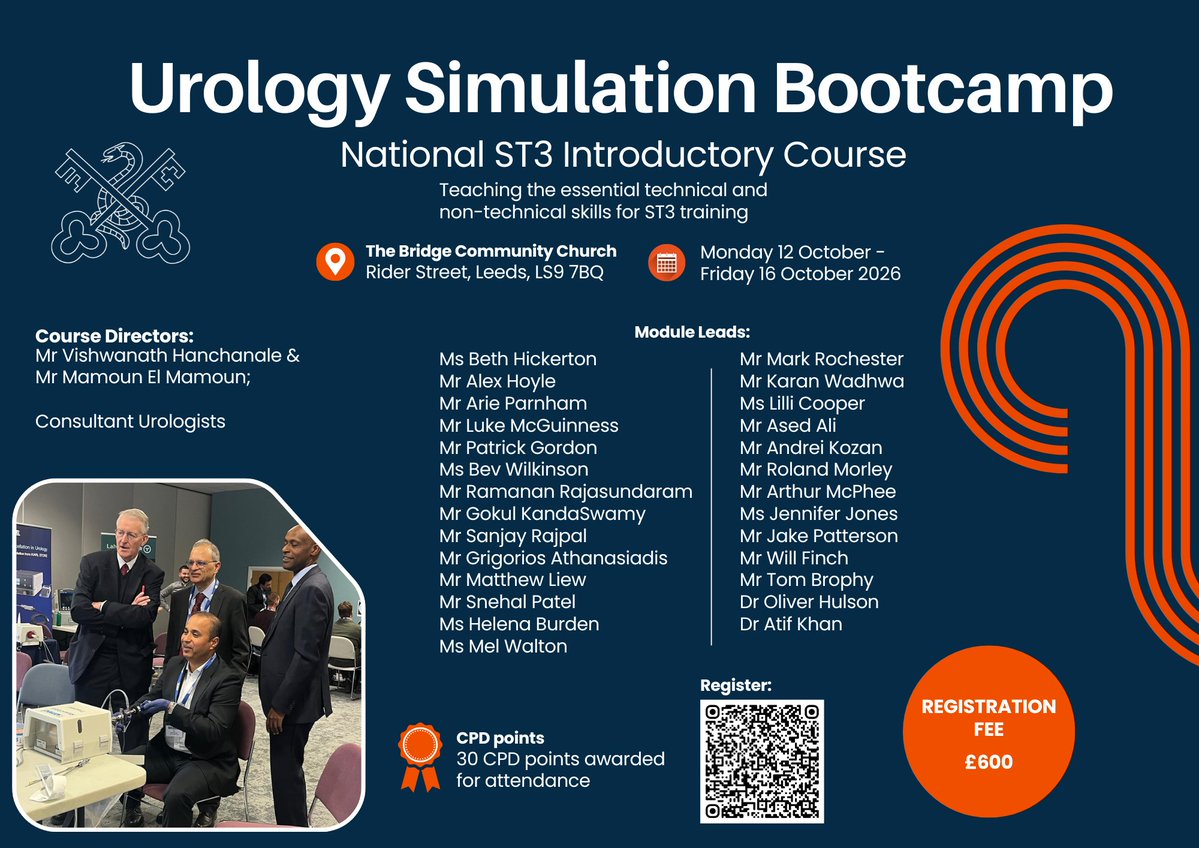
We have a wide range of interactive teaching and skills courses at the @BAUSurology annual scientific meeting to suit every career stage including some brand new courses.
Filling up fast- don’t miss out:
https://t.co/IsP8zZHkgI
🗣️ BAUS Statement on the UK National Screening Committee Recommendation on Prostate Cancer Screening
▶️ Read our full statement here: https://t.co/em0RS6Ukro
Day 3 Bike4TUF - the home straight.
Edinburgh across to Fife, the Campsie fells and into Glasgow - tired legs
Please consider donating to @TUF_tweets
https://t.co/KCznlTlQ6q
Day 2 Bike4TUF - still going! Berwickshire and East Lothian coast into Edinburgh. Windy but scenic.
Please consider donating to @TUF_tweets
https://t.co/KCznlTlQ6q
Humanoids are quietly crossing the line from lab demo to operational endurance machines.
What started as an 8 hour stress challenge just ran for 200 continuous hours without failure. The real breakthrough in robotics is persistence, reliability, spatial intelligence and long duration autonomy.
As humanoids scale into logistics, manufacturing, retail and real world navigation, they will need more than computer vision alone. They need to understand where they are, what surrounds them and how humans interact with space in real time...
"decentralized spatial infrastructure becomes important"
Projects like @AukiLabs are building machine perception layers that allow robots, devices and AI agents to share spatial understanding collaboratively.
trends most people are missing:
• Humanoid robotics is shifting from cloud dependent AI toward edge & distributed intelligence because latency becomes critical in physical environments
• Spatial mapping markets are expected to become foundational infrastructure for warehouses, smart cities and autonomous commerce
• Multi agent robotics systems will likely require shared localization protocols, similar to how the internet needed TCP/IP
• The next trillion dollar AI opportunity may not be chatbots, but embodied AI interacting with the physical world 24/7
200 hour uptime tests are a glimpse of what’s coming, companies building the robots will matter and protocols enabling machines to understand and coordinate in the real world would become even bigger
Cochrane updated its PSA screening meta-analysis. 789,086 men across 6 RCTs.
➡️ PCa-specific mortality: rate ratio 0.87 (moderate certainty)
➡️ Metastatic diagnosis: RR 0.65
➡️ Adverse events / QoL: little to no difference
Why this matters: 💡 PSA screening is back on stronger evidentiary footing for disease-specific mortality. Shared decision making still drives the recommendation downstream and additional tools (biomarkers and MRI) continue to improve the gap.
https://t.co/VZk9tKRW0V
@EBMUrology #ProstateCA #Screening #Cochrane #GUonc #AUA26
There is only one European nation with fewer hospital beds per capita than the UK
Sweden but they have the highest number of care home & nursing home beds
26% fewer care home beds
23% fewer nursing beds
Fewer hospital beds
Then people wonder why A&E is blocked
Please considering supporting me as I take part in the Bike4TUF Challenge which will see us cycle from Newcastle to Glasgow via Edinburgh in 3 days. ~400km with 3,400m of climb.
https://t.co/ywO0dIzEp4
How the 2026 run rates of the top AI labs and pharmaceuticals compare
1. Tirzepatide (~$51 B)
2. Anthropic (~$45 B)
3. Semaglutide (~$33 B)
4. Pembrolizumab (~$32 B)
5. Apixaban (~$25 B)
6. OpenAI (~$25 B)
7. Dupilumab (~$20 B)
8. Risankizumab (~$18 B)
9. Daratumumab (~$16 B)
10. Biktarvy (~$14 B)
Tech people, come to bio: there are lots of diseases left to solve
Final @BAUSurology trustees meeting for outgoing president @IPearce82
Many thanks for your considerable contributions to the specialty.
(in front of Frère Jacques, 17th c lithotomist)
The Urology Foundation funds research, education and raises public awareness into urological diseases from UTIs to prostate cancer. About half of the population experience a urological condition at some point their lives.
Please considering supporting me as I take part in the Bike4TUF Challenge which will see us cycle from Newcastle to Glasgow via Edinburgh in 3 days. ~400km with 3,400m of climb.
https://t.co/ywO0dIzEp4