Static vs. cidal: it’s not complex; it’s simply incorrect
@BradSpellberg et Al
Honored to be part of this amazing group who challenges dogmas and debunk ID myths #idxposts
https://t.co/4bldEnYTK5
What is the best approach for parenteral sedation to manage severe acute behavioral disturbance in the emergency department? A commentary by @KIsoardi, @bobhoffmd, @geoff_isbister and Jon Cole
https://t.co/rtkBgzPzDB
Do you have unused or expired meds? Saturday, April 25 is Drug Take Back Day! Stop by a collection event and drop your items into a bin, no questions asked.
Find a collection event near you: https://t.co/vDsE4rPXc2
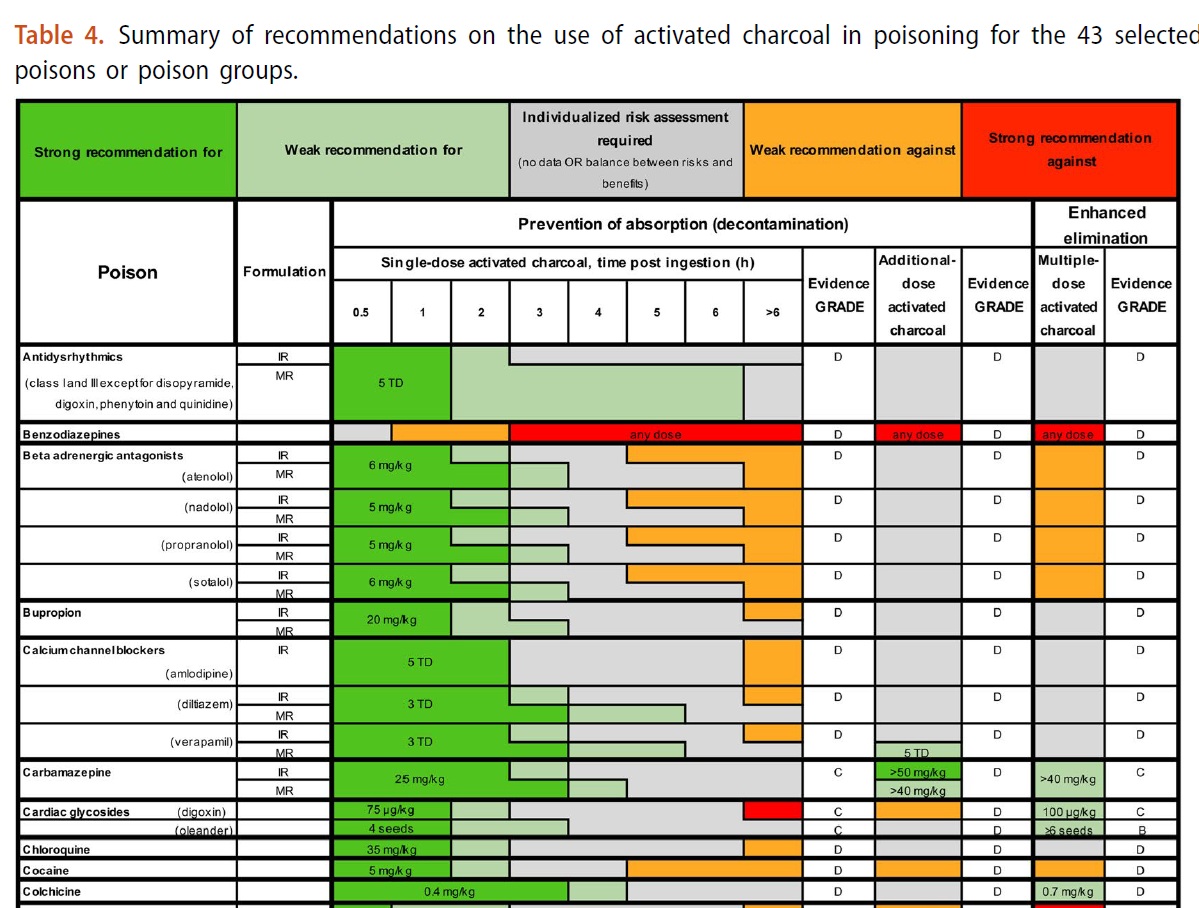
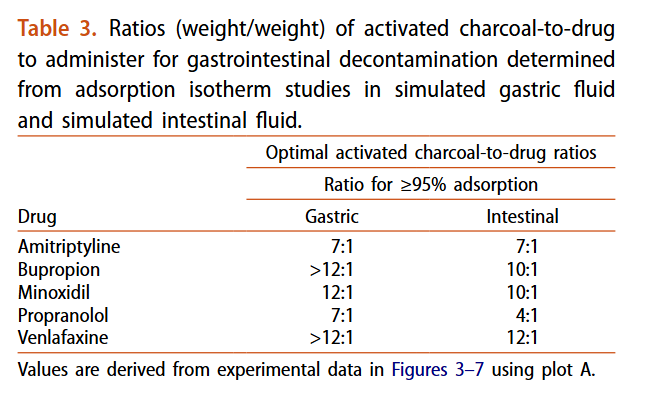
The Clinical Toxicology Recommendations Collaborative provides their recommendations on activated charcoal in acute oral overdoses. The paper includes recommendations on the use activated charcoal for 43 poisons/poison groups. Here's a peak of Table 4:
https://t.co/XSHLj2Whi8
The long awaited "Recommendations from the Clinical Toxicology Recommendations Collaborative on the administration of activated charcoal in acute oral overdose" are finally published. Open access downloads are available here: https://t.co/alIvryYfjJ
🔥⚠️We are fighting fever… when we should be using it 🤓
Every day in ICU...Paracetamol, Cooling blankets, Aggressive temperature control
But what if fever is not the problem 🤔
*Fever is not a failure of physiology
It is an adaptive response
Driven by cytokines and Controlled by the hypothalamus
🫀 Clinical implication
Fever is not noise...It is a signal
*Heat boosts immunity
At 38–41°C:
• ↑ Neutrophil activation
• ↑ NK cell activity
• ↑ Antigen presentation
• ↑ T-cell interaction
🫀 Clinical implication
You are suppressing immune function when you suppress fever
*Bacteria don’t like heat
Most pathogens:
• Optimal growth ~37°C
• Growth impairment near 40°C
Even more interesting
β-lactams work better at higher temperatures
🫀 Clinical implication
Fever may act as a natural antibiotic enhancer
*The paradox: treating fever may worsen outcomes
Observational data show:
• Higher fever → lower mortality
• Hypothermia → worse outcomes
And even more concerning
Antipyretics in sepsis → ↑ mortality
🫀 Clinical implication
We may be harming patients with “routine care”
*The myth of temperature control
Antipyretics reduce temperature by 0.3–0.5°C
No mortality benefit
Sometimes harm
🫀 Clinical implication
We are treating a number, not a patient
*The real strategy: permissive hyperthermia
Target:
~38–40°C
Not normothermia
Not aggressive cooling
🫀 Clinical implication
Fever should be tolerated, not eliminated
*When should we treat fever?
✔ Extreme hyperthermia (>40°C)
✔ Patient discomfort
✔ Cardiovascular stress
❌ Routine suppression in sepsis
🫀 Clinical implication
Treat symptoms, not physiology
*The uncomfortable truth
We were trained that fever is dangerous, but evidence suggests that Fever is PROTECTIVE and its suppression may be HARMFUL 🫨
🤓Final reflection
In sepsis, the goal is not comfort alone. The goal is survival, and sometimes survival requires heat😎🔥
📚 Tilanus A, Villamil W. Open Forum Infectious Diseases, 2025
“Fever in Sepsis Revisited: Is a Little Heat What We Need?”
https://t.co/sj6uLIOAey
🚫The American College of Emergency Physicians (ACEP) Will Not Endorse New Sepsis Guidelines from the Surviving Sepsis Campaign 🚫
The decision to not endorse the guidelines was based on concerns about conflicting guidelines for the treatment of adult and pediatric patients, and a belief that the guidelines developed do not fully reflect the most up-to-date and reality-based approach to the care of all patients in the emergency department, including those with sepsis😱
ACEP is worried that the focus of the SSC is strictly on those patients with sepsis while appearing to ignore the potential harm the guidelines might cause for patients without sepsis🎯 https://t.co/2Noqs9LFoq
Today our Outreach Coordinator, Bre, had the opportunity to be on Fox6 to share some information about the Wisconsin Poison Center and how we can help prevent and treat poisonings!
🔗Check it out here! https://t.co/WyvQHcxfoI
#NPPW26
Today we had the wonderful opportunity to visit Children's Wisconsin, where we connected with patients, families, and staff to share important information about National Poison Prevention Week.
Thank you to everyone who took the time to chat with us today!💚 #NPPW26
Check out this behind-the-scenes look at the Wisconsin Poison Center!
A typical day at the office includes taking calls, conducting educational sessions, and packing outreach materials for community partners! #NPPW26
https://t.co/7Ha0Q3yqfc
In vitro data show strong but drug- and pH-dependent adsorption of common antidepressant/cardiac drugs; a standard 50 g dose may be inadequate for bupropion, venlafaxine, and minoxidil overdoses
https://t.co/0j2bi4c6A2
Can sodium channel blockade treat sodium channel blockade?
https://t.co/nbqhP8K7Lx
In massive diphenhydramine overdose, VT may persist despite bicarbonate. In our case, QRS narrowed after lidocaine. Not causation—but plausible. Fast on–off may displace slow toxins.
#MedEd
1/4
Not all social media challenges are safe. Some can lead to serious poisonings, especially when medicine or household products are involved. Save the Poison Help line (1-800-222-1222) in your phone today! #PoisonPrevention#SocialMediaSafety
Fresh paper.
Adenosine is metabolized by red blood cells.
Do people with higher hematocrit need higher Adenosine doses?
Nope, but now we know. Negative studies matter 😂
Amazing work by our past resident Dr. Seth Carroll (@SethCPharmD)
https://t.co/VxgcJe0xiD
Hi Friends,
Join me tomorrow @1230pm, ill be on Larry Meiller's "Garden talk" on Wisconin Public Radio, i'll be talking about the new edition of Poisonous Fungus Amongus!