@nickmmark Two that are top of mind:
1. “We can stop the antihypertensives since the patient is on pressors.”
2. “We can stop midodrine since we are resuming the patient’s home antihypertensives.”
I’m happy to share others if needed.
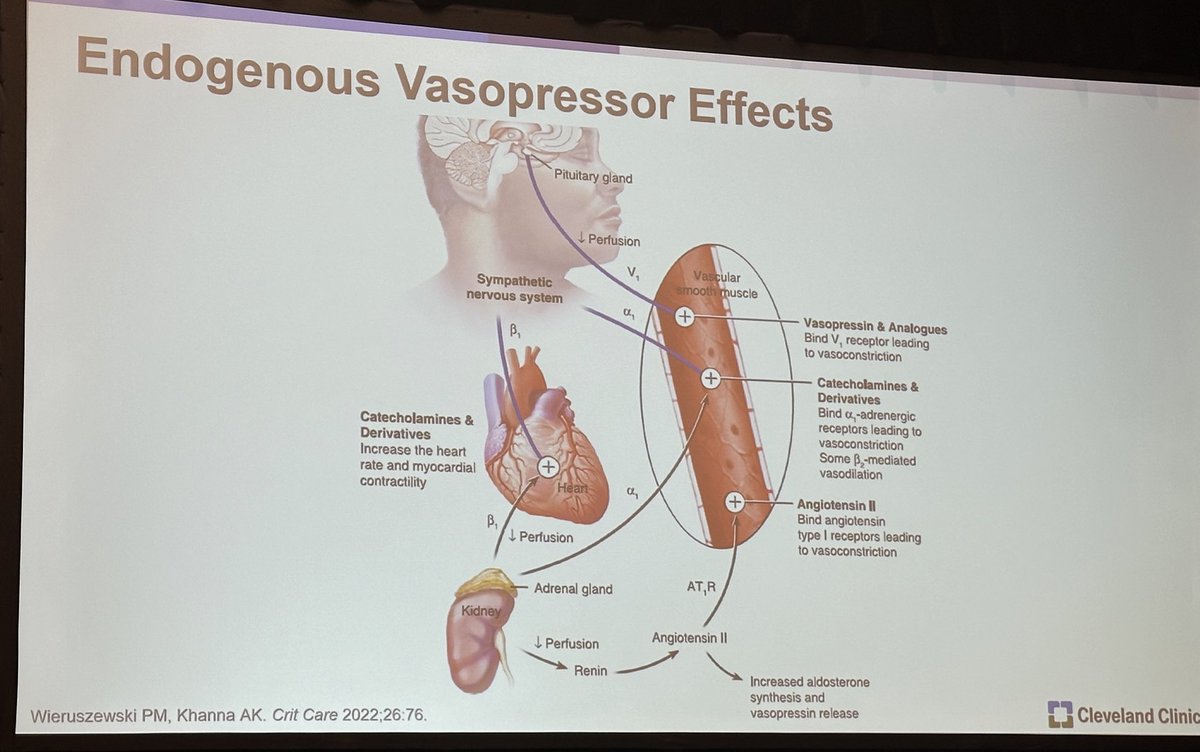
@SethRBauer next up on vasopressor choice after norepinephrine (NE) failure-
#CHEST2024
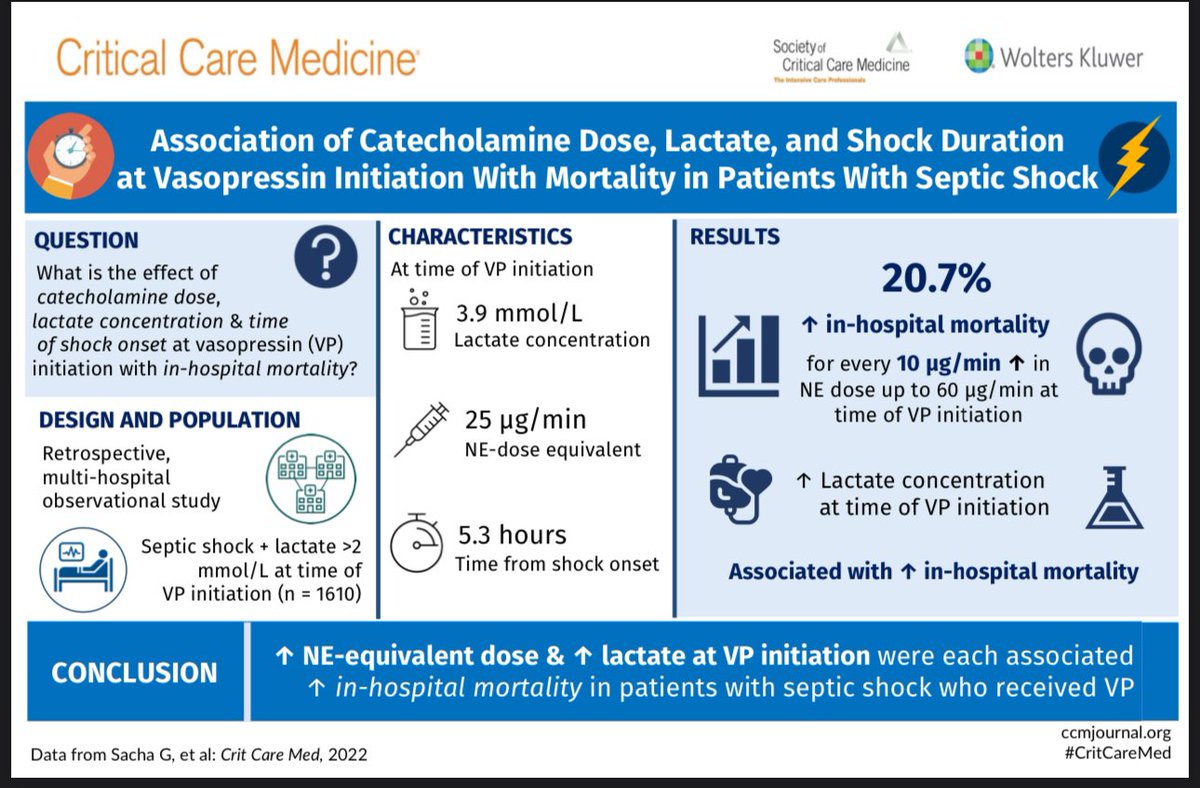
NE dose at which vasopressin should be started @gretchensacha ‘s paper https://t.co/wmPleXz9uD
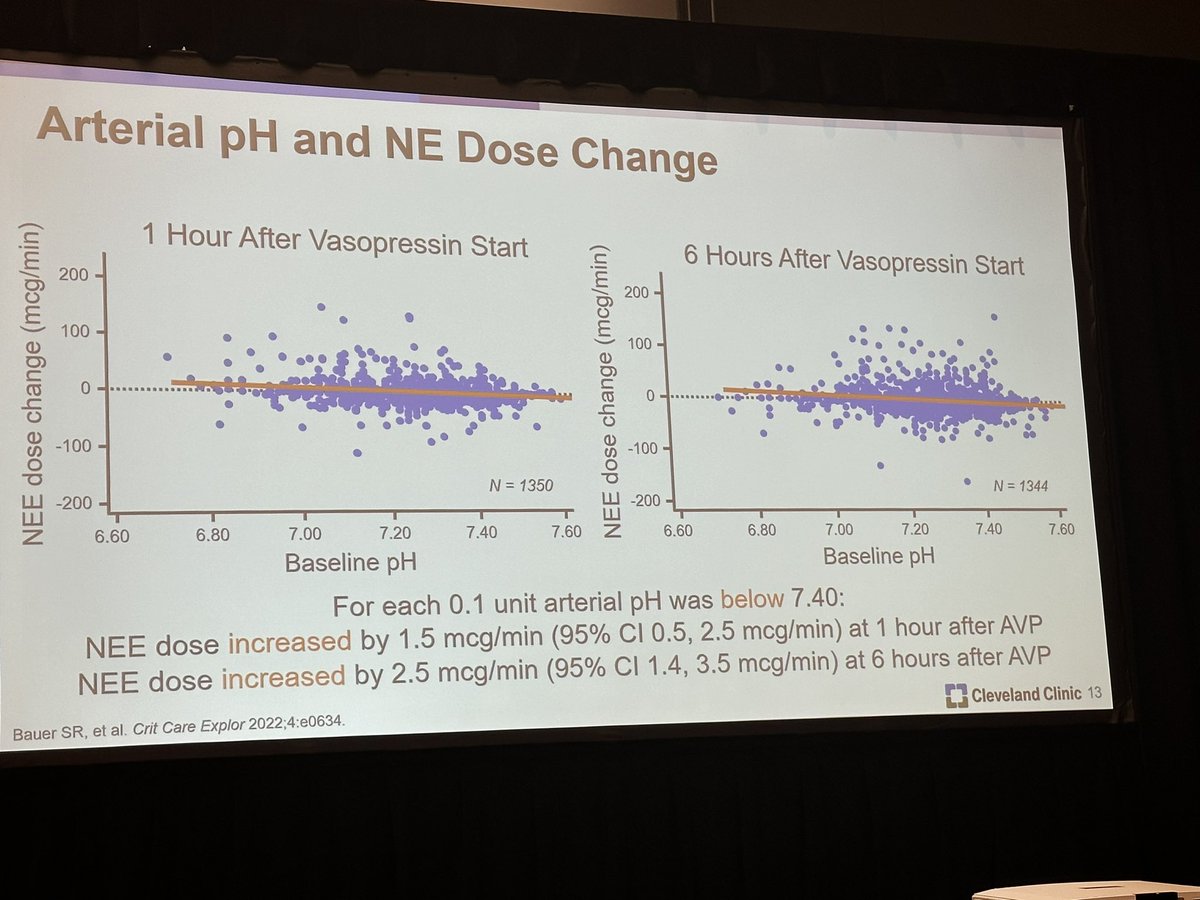
Vasopressin response: arterial PH and NE dose https://t.co/baicUoRtvz
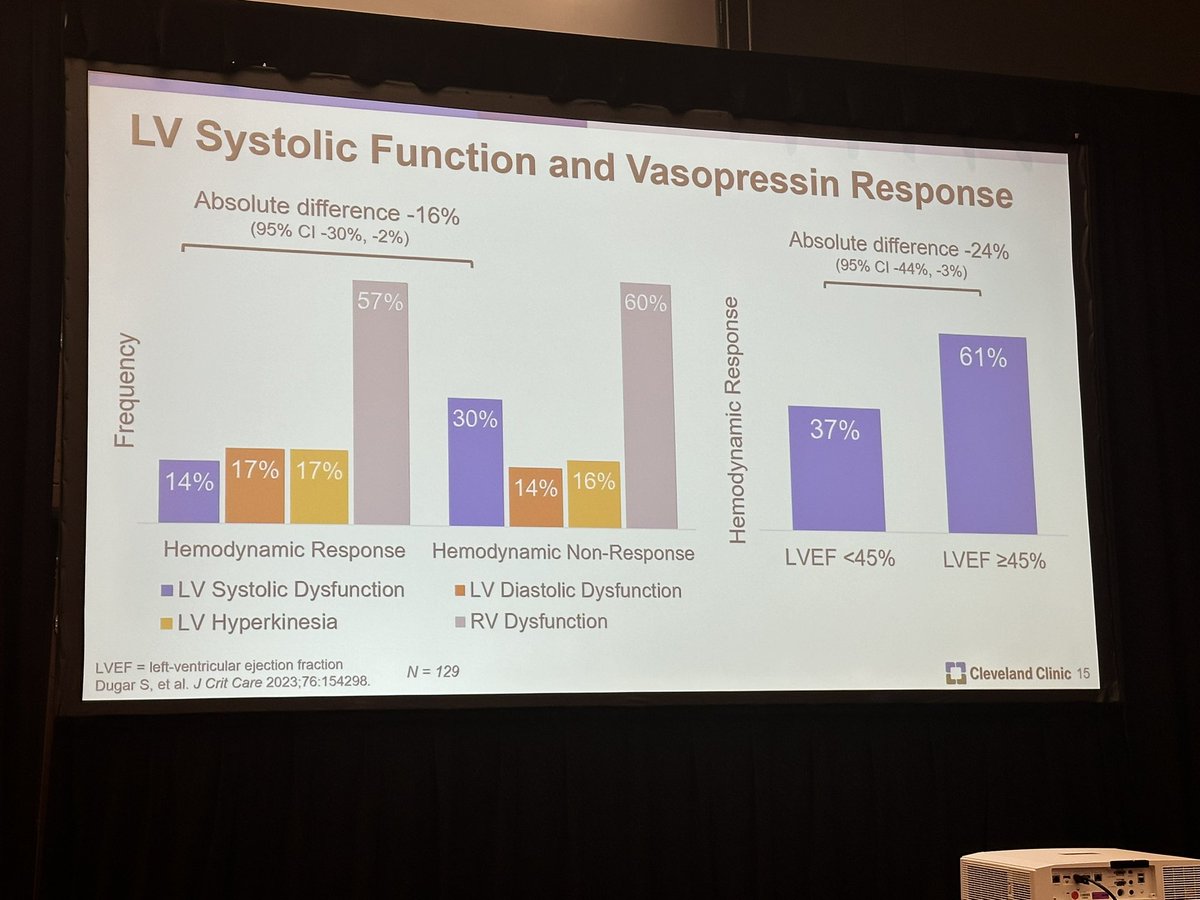
Cardiac function and vasopressor response https://t.co/FmeC8w7wZr
Angiotensin II @KhannaAshishCCM refresher on ATHOS https://t.co/Wo68vtfRh0
Renin and angiotensin II response: renin could be used as a bio marker https://t.co/UDOGyCZq1k
👀
A comprehensive rigorously composed list of renally-dosed and nephrotoxic medications - the #AKIP LIST!
The journal has made it open access til 10/05! Go get it and take a look!
https://t.co/JcB3c8vqEL
#Pharmacovigilance, #QI, #CDSS, the possibilities are endless!
My current thinking is:
1️⃣We should consider angiotensin II for this rationale particularly if renin is “high” (https://t.co/FLjBpcZbNv)
2️⃣🤷🏻♂️ but we probably should be titrating vasopressin and treating it as a vasopressor, not “endocrine replacement”😜
What do you think?
Framing I didn’t previously consider (inspired by @pwierusz):
When the kidneys sense hypoperfusion they release renin to activate the RAS. Since the downstream effect of renin is to increase angiotensin II, the kidneys interpret hypoperfusion as a deficiency of angiotensin II.
This has me pondering for shock:
1️⃣Why do we use exogenous vasopressin for a “relative deficiency” but not angiotensin II for the same rationale?
2️⃣If we use angiotensin II for a “relative deficiency” why do we titrate the dosage instead of using a fixed dosage like vasopressin?
Thinking about vasopressor verbiage in light of a recent discussion with @pwierusz. Our thinking is aligned but I’m curious about your opinion. If a patient is on norepinephrine, vasopressin is added, then norepinephrine titrated off, is the vasopressin adjunctive or monotherapy?
@AndreaSikora@pwierusz Thanks @AndreaSikora for continuing this conversation. My view is based on intent - in this case vasopressin was intended as adjunctive therapy when started. The fact that vasopressin ended up as the sole agent doesn’t change the intention. But apparently I’m in the minority. 🙃
This article from the Mayo pharmacy group (co-authored by @erin_barreto and @pwierusz) is downright amazing. 🔥 They have accomplished incredible things! After reading I immediately sent to our team as a model to emulate.
It’s not lost on me that I work at a center of immense privilege, and also I still stand in awe of the people who are trying to build something new.
New is tiring, uncomfortable, met with roadblocks, viewed with skepticism.
New is also transformative for us and others…
@GeorgeICUrias I’m not sure if titrated will be better, but note it’s the strategy used in the large vasopressin trials (VASST and VANISH). The mortality effect is small (if any) and predictive enrichment is likely necessary. We discussed dosing on @PharmacyToDose here: https://t.co/GsrsYN1fRy
🚨NEW POD ALERT🚨
🧂Norepinephrine Position Paper & Sepsis Research Priorities 🥇
Ft. Brittany Bissell Turpin @BissellTurpin
Patrick Wieruszewski @pwierusz@mayoanesthesia@curiousboxwood
Seth Bauer @SethRBauer
History of norepinephrine formulation reporting 📜
Clinical & research implications ⚔️
Management in the drug shortage era 😬
Top 5 clinical sepsis research priorities 5⃣
Why this matters for more than just researchers ⭐️
Important basic science questions 🧑🔬
& much more!
(Listen to the intros for a surprise or two)
https://t.co/UoGK2GRBnF
https://t.co/aqvpsFTTio