Which condition characteristically presents with diffuse ST-segment elevations and PR-segment depressions on ECG?
A. Acute myocardial infarction
B. Acute pericarditis
C. Pulmonary embolism
D. Dilated cardiomyopathy
A 32-year-old pregnant female at 28 weeks gestation comes in for routine prenatal visit. She has type 1 diabetes mellitus.
Her self-monitoring blood glucose logs show:
* Fasting: 90 – 95 mg/dL
* 1 hour postprandial: 130 – 140 mg/dL
However, her lab HbA1c is reported as 4.8%.
The physician also notes she has homozygous sickle cell anemia (HbSS).
Which of the following laboratory markers would provide the most accurate assessment of her glycemic control over the past 2 – 3 weeks?
A) Fasting plasma glucose
B) Fructosamine
C) HbA1c repeat test
D) OGTT
E) Urine ketones
Explain your answer in the comment section.
🚨 A 7-year-old boy comes for follow-up.
One week ago he had episodes of bloody diarrhea that have now resolved.
Today:
* Elevated BUN and serum creatinine
* Anemia + thrombocytopenia
* Coagulation studies completely normal
His peripheral blood smear is shown in the image below.
=> What’s the most likely diagnosis?
=> What finding do you expect to see on that smear?
Reply with your reasons.
Most Likely Diagnosis:
✅ Acute Pulmonary Embolism (PE) with right ventricular strain
Why?
=> Hospitalization is a major risk factor for venous thromboembolism.
=> The sudden onset of pleuritic chest pain, dyspnea, tachycardia, tachypnea, and hypoxemia is classic for PE.
=> Markedly elevated D-dimer supports ongoing thrombosis.
=> Mildly elevated troponin and elevated BNP suggest right ventricular (RV) strain, indicating an intermediate-risk (submassive) PE.
🚨 A 68-year-old man with hypertension and CKD is admitted for community-acquired pneumonia.
On hospital day 3 he develops acute pleuritic chest pain and dyspnea.
Vitals: HR 118, BP 138/82, RR 26, O₂ sat 92% on 4L NC.
Labs:
* D-dimer markedly elevated
* Troponin mildly elevated
* BNP elevated
* Cr 2.8 mg/dL (baseline 1.9)
=> What is the most likely diagnosis?
=> What's the appropriate next step?
🚨 A 7-year-old boy comes for follow-up.
One week ago he had episodes of bloody diarrhea that have now resolved.
Today:
* Elevated BUN and serum creatinine
* Anemia + thrombocytopenia
* Coagulation studies completely normal
His peripheral blood smear is shown in the image below.
=> What’s the most likely diagnosis?
=> What finding do you expect to see on that smear?
Reply with your reasons.
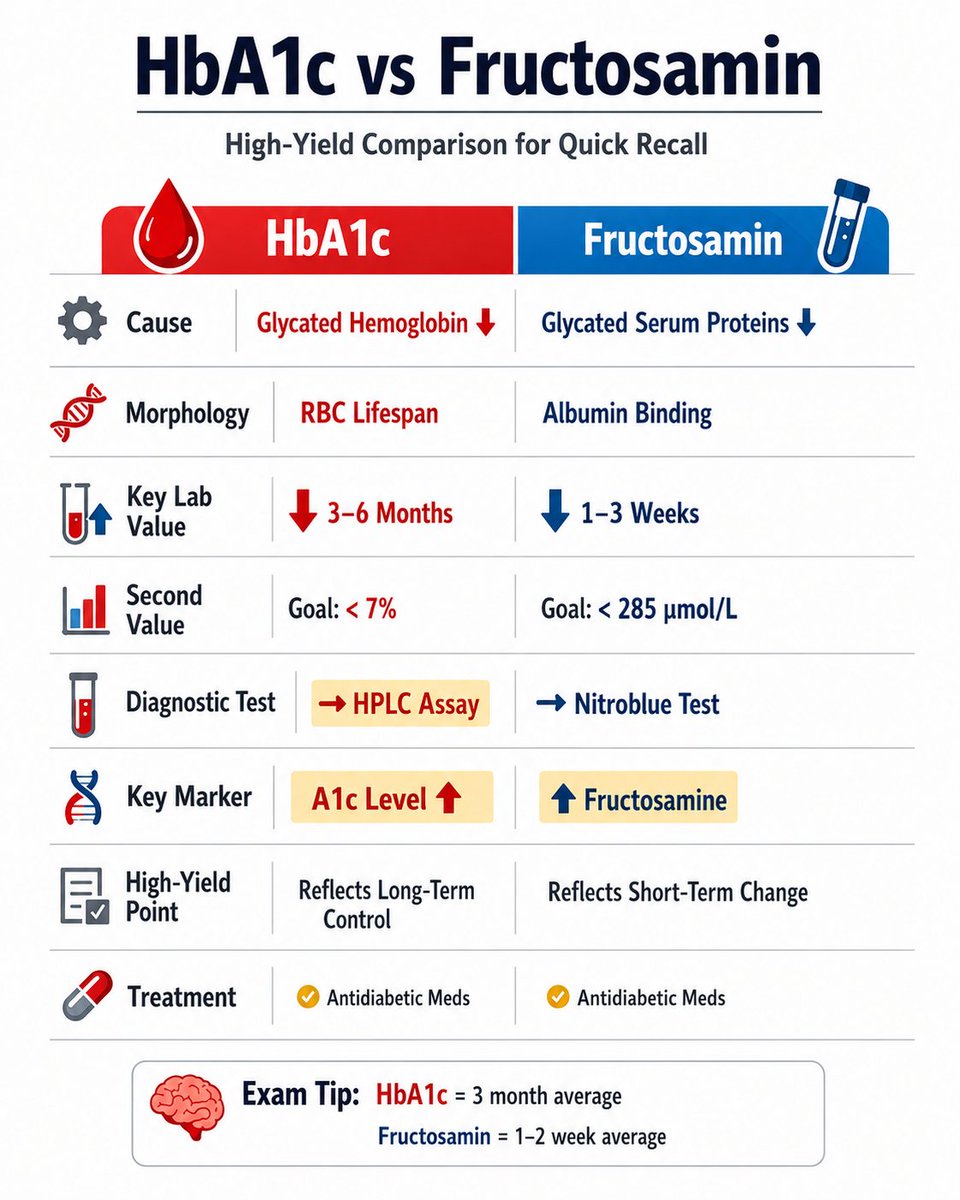
Answer: B) Fructosamine ✅
=> HbA1c is unreliable in patients with sickle cell disease (HbSS) because the shortened red blood cell lifespan reduces the time available for hemoglobin glycation, resulting in a falsely low HbA1c.
=> Fructosamine measures glycated serum proteins (primarily albumin) and reflects average blood glucose over the previous 2-3 weeks, independent of red blood cell survival.
=> In this patient, the HbA1c of 4.8% is falsely reassuring despite glucose logs suggesting higher average glucose levels. Therefore, fructosamine provides the most accurate assessment of recent glycemic control.
A 32-year-old pregnant female at 28 weeks gestation comes in for routine prenatal visit. She has type 1 diabetes mellitus.
Her self-monitoring blood glucose logs show:
* Fasting: 90 – 95 mg/dL
* 1 hour postprandial: 130 – 140 mg/dL
However, her lab HbA1c is reported as 4.8%.
The physician also notes she has homozygous sickle cell anemia (HbSS).
Which of the following laboratory markers would provide the most accurate assessment of her glycemic control over the past 2 – 3 weeks?
A) Fasting plasma glucose
B) Fructosamine
C) HbA1c repeat test
D) OGTT
E) Urine ketones
Explain your answer in the comment section.
Why not the others?
A. Adenosine deaminase => SCID
B. Glucose-6-phosphatase => Von Gierke disease
D. Xanthine oxidase deficiency => Xanthinuria (low uric acid, not gout)
Answer: C. HGPRT
=> The combination of developmental delay, self-mutilation (lip/finger biting), hyperuricemia, and gout is classic for Lesch-Nyhan syndrome.
=> Lesch-Nyhan syndrome is caused by deficiency of Hypoxanthine-Guanine Phosphoribosyltransferase (HGPRT), a purine salvage enzyme.
=> Loss of HGPRT leads to increased purine degradation and excess uric acid production, causing gout and neurologic manifestations.
Answer: B. Severe Combined Immunodeficiency (SCID)
=> The thymus is the site of T-cell maturation, so an absent thymic shadow suggests a profound T-cell deficiency.
=> SCID is characterized by severe defects in both T-cell and B-cell function, leading to severe lymphopenia and recurrent infections early in life.
=> On chest X-ray, infants with SCID often have an absent thymic shadow due to lack of normal thymic development.
An absent thymic shadow on a newborn X-ray combined with severe lymphopenia indicates which defect?
A. Bruton agammaglobulinemia
B. Severe combined immunodeficiency (SCID)
C. Chronic granulomatous disease
D. C5-C9 complement deficiency
@_uakbar ✅ Correct
Diffuse concave ST elevation + PR depression = pericarditis until proven otherwise.
What’s the most common cause of pericarditis in a young healthy patient vs an older one?
Which condition characteristically presents with diffuse ST-segment elevations and PR-segment depressions on ECG?
A. Acute myocardial infarction
B. Acute pericarditis
C. Pulmonary embolism
D. Dilated cardiomyopathy
@ajlkfad2333 ✅ Correct
Diffuse concave ST elevation + PR depression = pericarditis until proven otherwise.
What’s one ECG finding that would make you worry about tamponade instead?