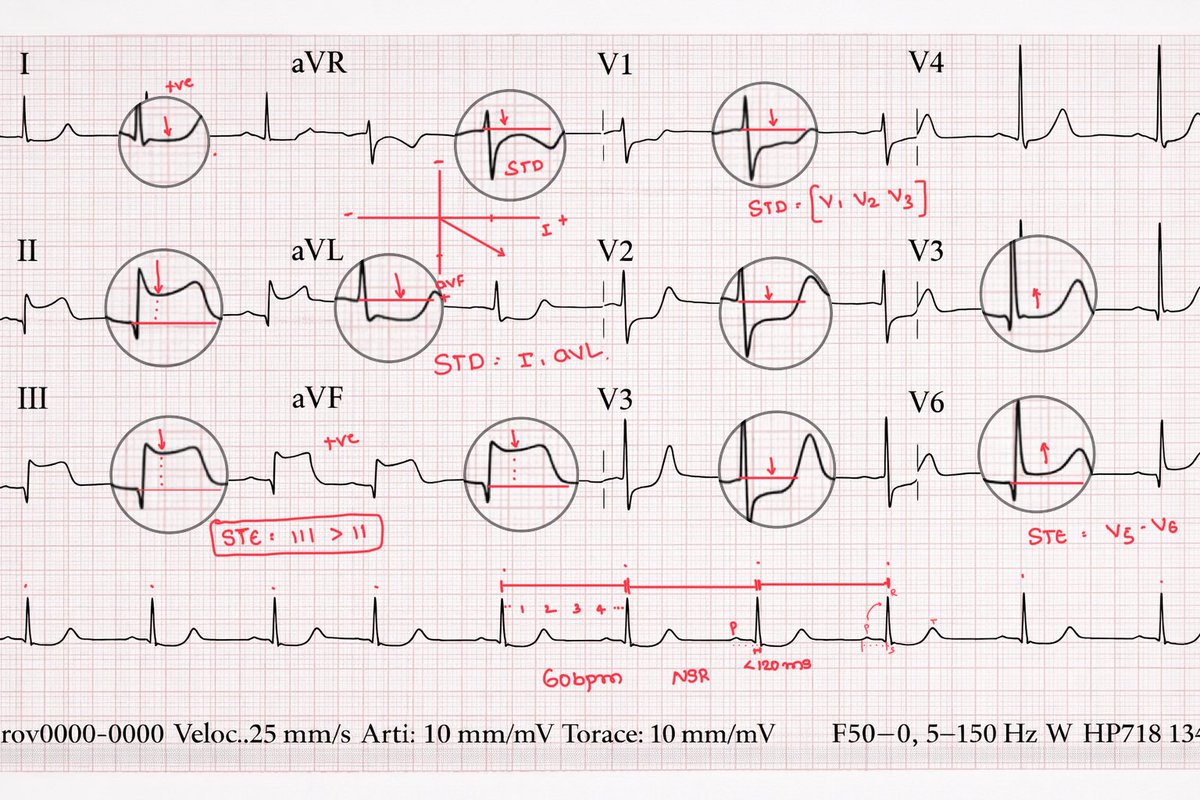
Breakdown of this ECG :
What the ECG Shows
✅ Inferior STEMI
STE in II, III, aVF
Reciprocal ST depression in I, aVL
STE in III > II → favors RCA over LCx
✅ Posterior Wall Involvement
ST depression in V1–V3
Tall R waves in V1–V2 (posterior Q equivalent)
👉 This = posterior extension of inferior MI
✅ Lateral ST Elevation (V5–V6)
There is STE in V5–V6
But why?
So this is not a “pure” inferior MI.
What Pattern Is This?
👉 Infero-posterolateral STEMI
Now the key question:
If RCA is culprit, why lateral wall involved here ?
The Explanation :-
It depends on coronary dominance.
In a dominant RCA.
RCA supplies:
▶️Inferior wall
▶️Posterior wall (via PDA)
▶️Sometimes posterolateral branches
If the occlusion is:
👉 Proximal RCA before the posterolateral branch
Then you get:
Inferior STE
Posterior STD (V1–V3)
Lateral STE (V5–V6)
So lateral wall involvement can still be RCA especially in a dominant system.
Now look at aVR, it seems like there is ST depression is there?
What does it signifies?
In the setting of:
STE in II, III, aVF
Reciprocal STD in I, aVL
Posterior involvement
👉 ST depression in aVR usually reflects transmural inferior injury vector directed away from aVR.
#MedTwitter #MedX #ECG #cardiology
In DKA you give 5-8 litre fluid
1 litre 1st, next 2 hrs, next 2 hrs, next 4 hrs, next 4 hrs, next 6 hrs
K+ 10mmol/hr, but OMIT 1st fluid bag
Insulin @ 0.1 U/kg/hr
↓Ketones by ≥0.5/hr & glucose by 3 mmol/L/hr
+Dextrose when RBS < 14mmol
Give S/C LMWH ppx
Follow for more!