Low back pain is defined as pain located below the costal margin and above the inferior gluteal folds, with or without leg pain and is the leading cause of years lived with #disability worldwide, affecting people of all ages.
📝 This JAMA Review summarizes the epidemiology, pathophysiology, clinical evaluation, prognosis, and treatment of nonspecific low back pain in the outpatient setting.
https://t.co/2E9vJ71LQA
Low back pain is defined as pain located below the costal margin and above the inferior gluteal folds, with or without leg pain and is the leading cause of years lived with #disability worldwide, affecting people of all ages.
📝 This JAMA Review summarizes the epidemiology, pathophysiology, clinical evaluation, prognosis, and treatment of nonspecific low back pain in the outpatient setting.
https://t.co/FBOXpOrkWn
Color Flow Doppler in Echocardiography:
Color Doppler imaging displays blood flow direction and velocity within the heart. By convention:
🔴Red = Flow toward the transducer
🔵Blue = Flow away from the transducer
(BART rule: Blue Away, Red Toward)
The color velocity scale (shown on side) indicates flow speeds brighter hues = higher velocities.
The Nyquist limit (e.g., 69 cm/s here) defines the max velocity measurable without aliasing. Exceeding this limit causes aliasing: an apparent "color wraparound" mimicking reversed flow.
Limitations:
- Aliasing at high velocities
- Angle dependency: inaccurate if Doppler angle isn't aligned with flow
- Lower spatial resolution compared to 2D imaging
Clinical Significance:
Essential for detecting valve regurgitation, stenosis, septal defects, and abnormal shunts. Vital in assessing intracardiac flow patterns and diagnosing cardiac diseases early.
(Ref: Bulwer BE, Rivero JM. Echocardiography Pocket Guide, Jones & Bartlett, 2011, 2013)
2026 AHA/ACC/ADA/ASN Guideline for the Prevention, Detection, Evaluation, and Management of Cardiovascular-Kidney-Metabolic Syndrome
https://t.co/0POS80XBM2
💊مسكنات الألم غير الستيرويدية
مع اهم التوجيهات و الفروق بينها
Nonsteroidal anti-inflammatory drugs (NSAIDs)
💊 ديكلوفيناك Diclofenac
الجرعة المعتادة : 50 ملجم كل 8–12 ساعة
الحد الأقصى اليومي : 150 ملجم
ملاحظة :
يستخدم للألم والالتهاب مثل التهاب المفاصل الروماتويدي
💊 إندوميثاسين Indomethacin
الجرعة المعتادة : 25–50 ملجم كل 8–12 ساعة
الحد الأقصى اليومي: 150 ملجم
(قد يصل إلى 200 ملجم لبعض الأمراض الروماتيزمية)
ملاحظة :
مفيد في نوبة النقرس الحاد وبعض أنواع الصداع، و امراض الروماتزم ، لكن آثاره الجانبية العصبية أكثر شيوعاً مثل الصداع والدوخة.
💊 حمض الميفيناميك Mefenamic acid
الجرعة المعتادة : 250 ملجم كل 6 ساعات
أو 500 ملجم ثلاث مرات يوميًا
الحد الأقصى اليومي: 1000 ملجم
(لعسر الطمث قد نصل إلى 1500 ملجم)
ملاحظة :
شائع لآلام الدورة الشهرية، ولا يُنصح باستخدامه لأكثر من 3–7 أيام
💊 ميلوكسيكام Meloxicam
الجرعة المعتادة : 7.5–15 ملجم مرة يومياً
الحد الأقصى اليومي : 15 ملجم
ملاحظة:
مفعوله طويل و بداية مفعوله بطيئة ، وتأثيره أقل على الصفائح الدموية مقارنة ببعض NSAIDs.
💊 إيبوبروفين Ibuprofen
الجرعة المعتادة : 400 ملجم كل 4–6 ساعات
أو 600–800 ملجم كل 6–8 ساعات
الحد الأقصى اليومي :
3200 ملجم للحالات الحادة
2400 ملجم للاستخدام المزمن
ملاحظة:
من أكثر المسكنات استخدامًا، مناسب قصير المفعول، لكن يجب الحذر مع أمراض المعدة والكلى.
💊 نابروكسين Naproxen
الجرعة المعتادة: 250–500 ملجم كل 12 ساعة
أو 250 ملجم كل 6–8 ساعات
الحد الأقصى اليومي :
1250 ملجم للحالات الحادة
1000 ملجم للاستخدام المزمن
(قد يصل إلى 1500 ملجم أثناء النوبات الحادة)
ملاحظات:
يفضل للألم المزمن و الحاد مع الالتهاب ، وقد يكون أقل خطورة قلبية مقارنة ببعض NSAIDs الأخرى.
💊 سيليكوكسيب Celecoxib
الجرعة المعتادة : 200 ملجم يوميًا
أو 100 ملجم كل 12 ساعة
الحد الأقصى اليومي : 400 ملجم
ملاحظات :
_ أقل خطورة على الجهاز الهضمي مقارنة بمضادات الالتهاب غير الانتقائية (NSAIDs)
_ قد تقل هذه الأفضلية عند استخدام جرعات منخفضة من الأسبرين بالتزامن معه، وقد يحتاج المريض لحماية معدية
_ لا يؤثر على وظيفة الصفائح الدموية
_ المخاطر القلبية والكلوية تعتمد على الجرعة وقد تكون مشابهة لبقية NSAIDs
_ قد يكون مناسبًا لبعض المرضى الذين لديهم حساسية أو تفاعلات شبه تحسسية تجاه NSAIDs الأخرى (مثل الربو أو التهاب الأنف التحسسي المرتبط بالأسبرين)
ملاحظات عامة أسفل الجدول :
_ هذا النوع من المسكنات مفيد لعلاج الألم والالتهاب الحاد والمزمن وقد تقلل الحاجة للأفيونات
_ يُفضل استخدام أقل جرعة فعالة لأقصر مدة ممكنة
_ في الألم الحاد: يُفضل استخدام NSAIDs قصيرة إلى متوسطة المفعول مثل Naproxen أو Ibuprofen
_ في الحالات الالتهابية المزمنة: قد يحتاج تقييم الفعالية إلى تجربة لمدة أسبوعين أو أكثر
_ كبار السن ومرضى القلب أو الكلى أو الجهاز الهضمي يحتاجون حذرًا أكبر
_ قد تكون هناك حاجة لاستخدام حماية للمعدة مثل مثبطات مضخة البروتون (PPI)
_ الجرعات المذكورة مخصصة للأشخاص ذوي وظائف الكبد والكلى الطبيعية
_ بعض الأدوية قد تتطلب جرعة تحميل في حالات الألم الحاد
_ يجب الانتباه للتداخلات الدوائية قبل وصف العلاج
♦️UpToDate
Coronary artery territories
The main epicardial coronary arteries supply distinct regions of the myocardium, which can be mapped and assessed during an ultrasound examination. For standardization, the left ventricle (LV) is divided along its long axis into four quadrants: anterior, inferior, septal, and lateral.
At the basal and midventricular levels, the septal and lateral walls are further subdivided into anterior and inferior segments. Each wall is then divided in short-axis views into basal, mid, and apical thirds. Beyond the LV cavity, the distal apex forms a cap segment. Altogether, this results in a total of 17 myocardial segments.
Most of the heart’s blood supply comes from the left main coronary artery, which divides into the left anterior descending (LAD) and left circumflex (LCx) arteries. The LAD supplies most of the anterior ventricular wall, while its septal branches supply the anterior two-thirds of the interventricular septum. Its diagonal branches supply the anterolateral wall. In some cases, a large LAD may wrap around the apex and supply the distal portion of the inferior wall.
The LCx travels in the atrioventricular groove, and its obtuse marginal branches supply the inferolateral wall. The right coronary artery (RCA) supplies the inferior third of the septum and the inferior wall, and it also provides blood to the right ventricle.
Adapted from Bulwer BE, Rivero JM, eds. Echocardiography Pocket Guide: The Transthoracic Examination
🫀The failing right ventricle:
the most misunderstood chamber in critical care
For years, we focused on the left ventricle.
But in the ICU, the real killer is often the right ventricle.
->What is acute RV failure?
👉 Not just “weak contraction”
It’s a hemodynamic collapse syndrome:
RV dilation
↓ LV preload
↓ cardiac output
↑ venous congestion
➡️ → multi-organ failure
->The key pathophysiology (the vicious cycle)
1. ↑ Afterload (PE, ARDS, PH)
2. → RV dilation
3. → Septal shift → LV underfilling
4. → ↓ CO → hypotension
5. → ↓ RCA perfusion
6. → RV ischemia
👉 And the cycle accelerates
->The most important concept
👉 The RV does NOT tolerate pressure
Handles preload very well
Fails rapidly with afterload
➡️ Even small ↑ PVR → collapse
->Main causes you MUST think first
🔴 Pulmonary embolism
🔴 RV myocardial infarction
🔴 ARDS / mechanical ventilation
🔴 Decompensated pulmonary hypertension
🔴 Post-cardiac surgery
->Diagnosis is NOT obvious
There is no single sign.
👉 It requires suspicion + integration:
Clinical: congestion + hypoperfusion
ECG + biomarkers
POCUS (your best friend 🤓)
Hemodynamics
->Echo mindset (fast ICU approach)
👉 Don’t overcomplicate
Look for:
✔ RV dilation
✔ Septal shift (D-sign)
✔ TAPSE ↓
✔ Venous congestion
The real ICU mistake
❌ Treating RV failure like LV failure
->Management principles
👉 Think in 4 pillars:
1. Preload — “not too much, not too little”
Hypovolemic → small fluid
Congested → REMOVE fluid
👉 CVP is not a target, it’s a warning
2. Afterload, THE key target
✔ Treat PE
✔ Optimize ventilation
✔ Reduce PVR
👉 If afterload stays high → RV will fail
3. Contractility
Dobutamine
Milrinone
Levosimendan
👉 Choose based on context
4. Perfusion pressure
👉 Norepinephrine is your anchor
✔ Maintains coronary perfusion
✔ Supports RV function
->Ventilation: the silent killer
⚠️ Positive pressure = ↑ PVR
👉 Over-ventilate → worsen RV failure
->When nothing works
👉 Think early:
VA-ECMO
RV assist devices
🤓Key insight
This is NOT just a cardiac problem.
👉 It is a ventriculo–arterial coupling failure
When:
Ees / Ea ↓ → RV collapses
🤓Bottom line
✔ RV failure is preload dependent BUT afterload sensitive
✔ Small mistakes → rapid collapse
✔ Early recognition + physiology-based treatment saves lives
->Clinical mindset
👉 Don’t ask:
“Is the RV failing?”
👉 Ask:
“Why is the RV failing and, what is driving the afterload?”
📃Reference
Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 https://t.co/gri8ZaHHsI
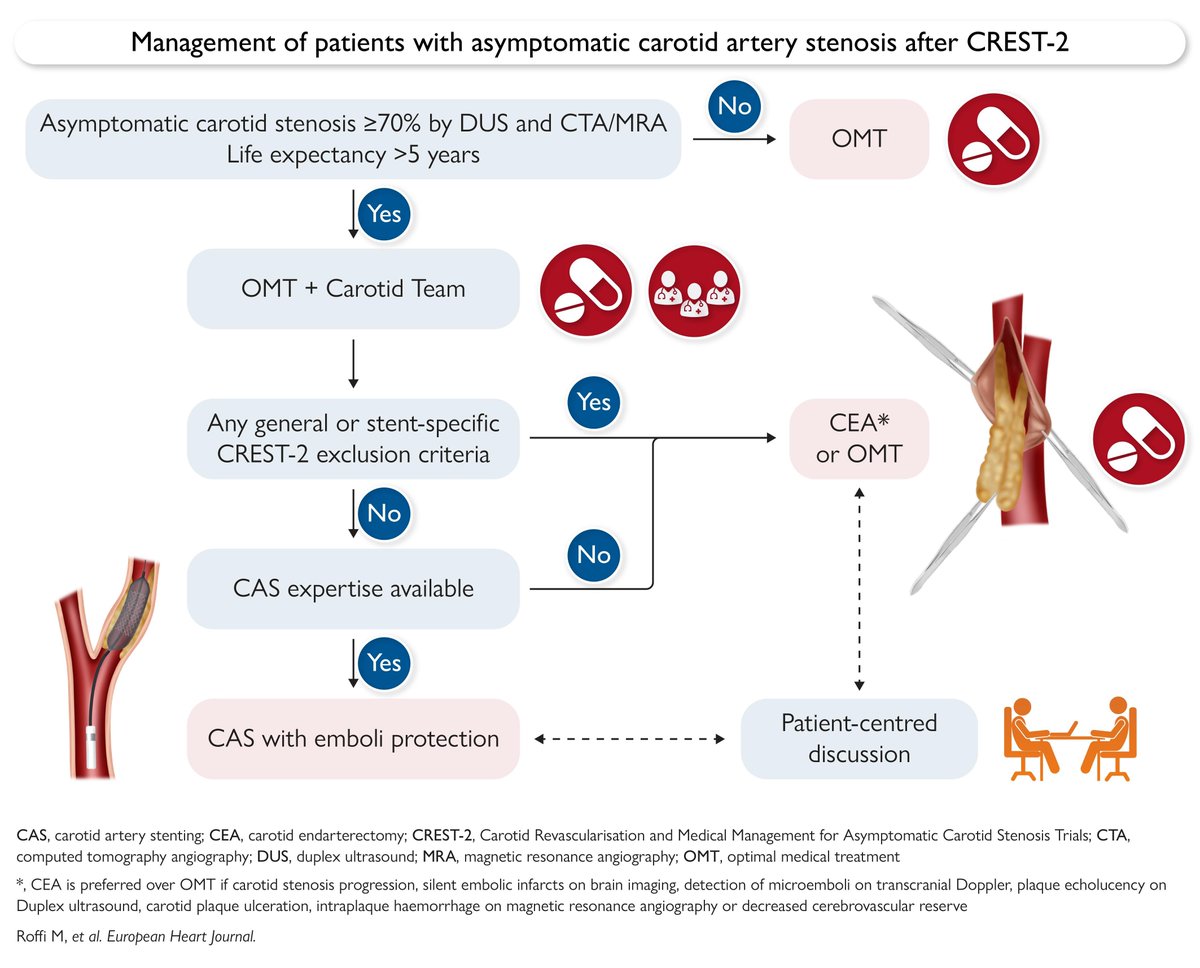
Carotid artery stenting in asymptomatic disease: a new paradigm after CREST-2 trial. Read this Viewpoint in #EHJ
👉 https://t.co/RwusA1pPcV
@RoccoMontone@ehj_ed