Reimagining Alzheimer’s (Part 1) via @forbes https://t.co/Pat6HmSXTi
Three part series.
Topic: #Alzheimers w/focus in Part 2+Part 3 on #ApoE4 gene status. ApoE4 associated w/
⬆️ cardiovascular risk
⬇️ inflammation control
⬆️ leaky blood brain barrier (think certain infections)
@awanderingkelly 👏🏻 wishes for another 9years and the same report, Kelly 👏🏻
Still out here hoping for Myasthenia Gravis or Sjogrens sooner than later. Be well.
1/ 🚨 New study alert! 🚨
Can your gut #microbiota predict how you'll react to dietary emulsifiers? 🤔 Our lab's latest work explores this question using an in vitro microbiota model. 🌟 Published in @gutBMJ! 🧵👇
https://t.co/VTVu6wZGXr
I highly urge folks to listen to this incredible and informative podcast episode. We NEED people appropriately dosed with doxy after a tick bite. In many Lyme-endemic areas in the northeast, almost all ticks now carry Lyme and it can spread mins-hrs, not days, after the bite
Just saw a neighbor share this CNN story tagging an RA family member. Word is spreading Dr Tracey. Another neighbor sent you an email a couple weeks ago curious about her Tourette’s+Ulcerative Colitis situation for pilot studies or being a case study on her dime if possible. 🙌🏻
What began as a scientific question in the lab is now a treatment for RA patients. Congratulations to the entire @SetPointMed team for developing the innovative device to stimulate the vagus nerve inflammatory reflex, and for sponsoring and leading the clinical trials with excellence, persistence, and compassion, culminating in FDA approval.
This is a great journey in translational science, in collaboration with hundreds of people, all for the benefit of patients. Which is what the destination has been all along.
On the verge of bankruptcy, but after a year of combing the world for answers, the Xolair + Doxycycline + Qulipta + Celebrex + HistaQuel + Perrin Technique (i.e., glympathic drainage) combo is doing work. We are already coming off of my Topamax. Adding doxy to my mast cell regiment was the exact thing I needed. I am still struggling with cerebral hypoperfusion, but that's why we have the vascular and spine team.
I wanted to see if it could be done. I did this for everyone who has died trying. There's been many. I share my story for them and everyone who comes after me.
#millionsmissing
#solveME
"When you start treating hypermobility as the fifth vital sign, [the list of differentials] completely changes."
--------------
"You know what's wild, as a GI doctor, there was things I were taught in fellowship that I would never see in my career, Median Arcuate Ligament Syndrome (MALS), Superior Mesenteric Artery Syndrome, Retrograde Cricopharyngeus Dysfunction (R-CPD), are zero [incidence]. Really, really rare, but once you start treating people with hypermobility, you realize that they aren't that rare anymore. In fact, they are quite common, and it completely changes the way you think.
In general, when we think "peptic ulcer disease", we think "h pylori". When we hear "bloating", we think "celiac disease, lactose tolerance." However, when treating hypermobility, the menu completely changes. You are thinking, "structural instability, motility issues, vascular compression,."
So yes, in general, these conditions are rare, but not in people with hypermobility, which makes me think we don't have a rare disease problem, we have a pattern recognition problem."
AS I HAVE BEEN SAYING, THE AUTONOMIC NERVOUS SYSTEM IS RESPONDING TO HYPERMOBILITY. If an infection triggered or worsen hypermobility, then "dysautonomia"
will follow suite to signal:
1.) "Hey, we are stressed about this neck instability, this joint dislocation, panic panic, please tighten your muscles"
2.) "Hey, your vascular compression and other blood vessel issues are now causing poor venous return, please overcompensate with increased heart rate to improve blood flow."
Mast cells are in connective tissue. They will degranulate more frequently as hypermobility worsens, causing a floodgate of inflammatory mast cell mediators to rush the brain and body. This will cause neuroinflammation, more dysautonomia.
If we stay stuck only thinking about the brain, then we miss out of most of the story.
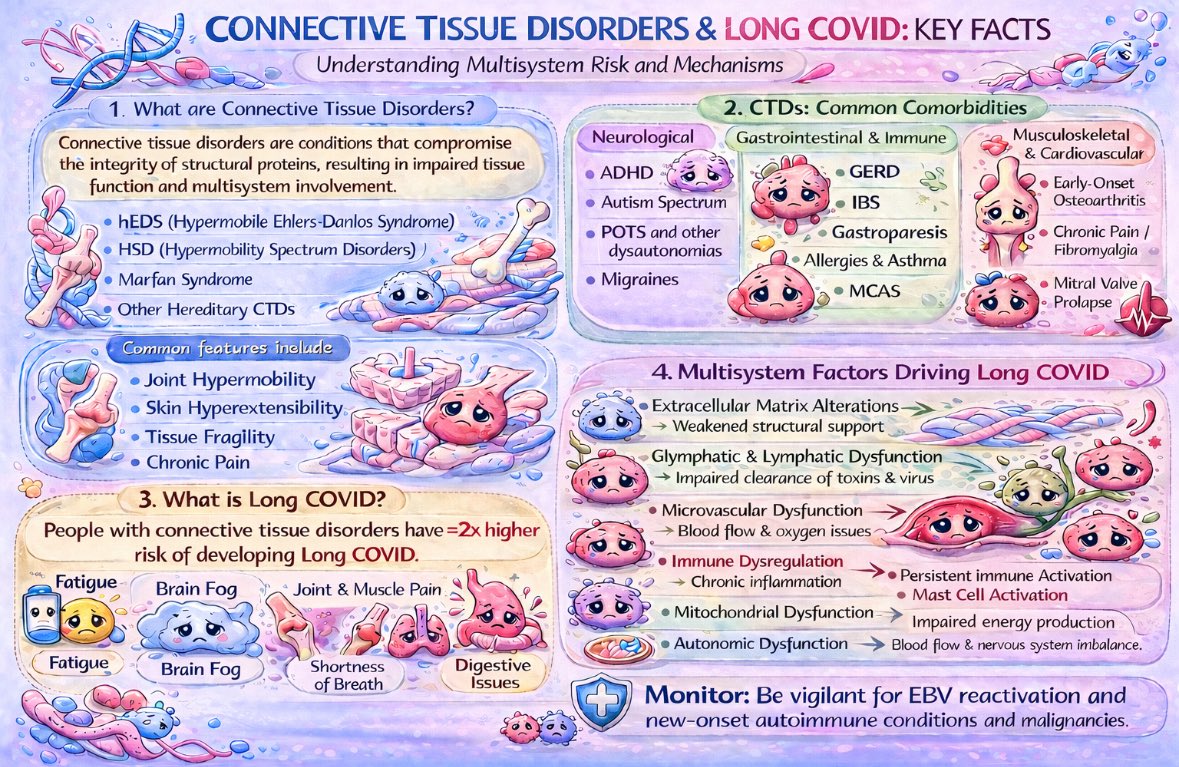
When my colleagues and I became severely sick and disabled over the past year, I knew I had to spring into action to learn about the mechanisms behind Long COVID. Our doctors were not giving us answers because the risks and drivers behind persistent spike are poorly understood and underecognized in medicine--the perfect recipe for disaster, disease, and mortality.
I have been researching these mechanisms for the past year--perhaps my most impactful work in neurodevelopmental medicine was while on short-term disability leave while I try to determine how to stay alive and recover as a person with hypermobile Ehlers Danlos Syndrome (only diagnosed in December at age 36) and ADHD.
Hopefully my next poster is a research-informed protocol targeting all of the multisystem factors indicated in section 4!
Niche terms like "Fascial restrictions" hold people back from connecting to the much broader and more understood clinical concept of "adhesions" (or perineural fibrosis) and nerve entrapment. Same issue I have when people talk about "acquired tethered cord" vs "spinal adhesion".
Today is a big final day. Teshia Zuniga with @RuchiMathurMD and @GabrielaGSLeite show that rheumatoid arthritis is associated with #sibo. Is there a link to autoimmune diseases or does SIBO fuel the fire? More work is needed. @MASTprogram#microbiome
This one is for the skeptical academics. We measured breath hydrogen sulfide and methane then immediately scope the patient and measured the same in duodenum and symptoms and microbiome. Guess what...breath correlates with duodenum and symptoms so gases are from small bowel!
This morning is a big one from @MASTprogram@CedarsSinaiMed. We sequenced and characterized vinculin antibodies on the path for new drug development for #IBS patients positive for these antibodies! Come hear Dr. Germano in room W184d.
Severe asthma coupled with a bladder pain disorder introduced me to a concept that changed (and saved) my life. The idea that chronic infections can fuel diseases considered to be idiopathic and/or purely autoimmune. #ChlamydiaPneumoniae#Lyme+
My initial Lyme Dx missed 2 persistent infections *Babesia microti & *Bartonella henselae. Ten years of treatment - missing puzzle pieces. I’m mostly well - but unresolved relapsing symptoms: fatigue, low-grade fevers, rib pain. Thx to researchers who won’t give up, I know why.
🔥 LYME FOUND IN HEART & PANCREAS of 30-year-old male tissue donor w history of Lyme! Why do blood tests miss over 50% of Lyme cases? It evades blood! It persists, like other pathogens, by hiding in organs & tissue where it’s hard to detect and kill!
YES. CHRONIC LYME IS REAL.
Every experiment needs to be logged in the blockchain and then released publicly upon submission. Manual custody of data is a relic of the past. Physical lab notebooks are dead. I can give specific examples of how recent events have exposed the absurdity of this. Manual peer review is performative. Closed peer review is no longer needed.
Important Study - #LongCOVID
TY @polybioRF
Also, a shoutout to @UTSWMedCenter for another example of supporting one of your own in their pursuit of thinking outside the box and advancing science as a PI 👏🏻
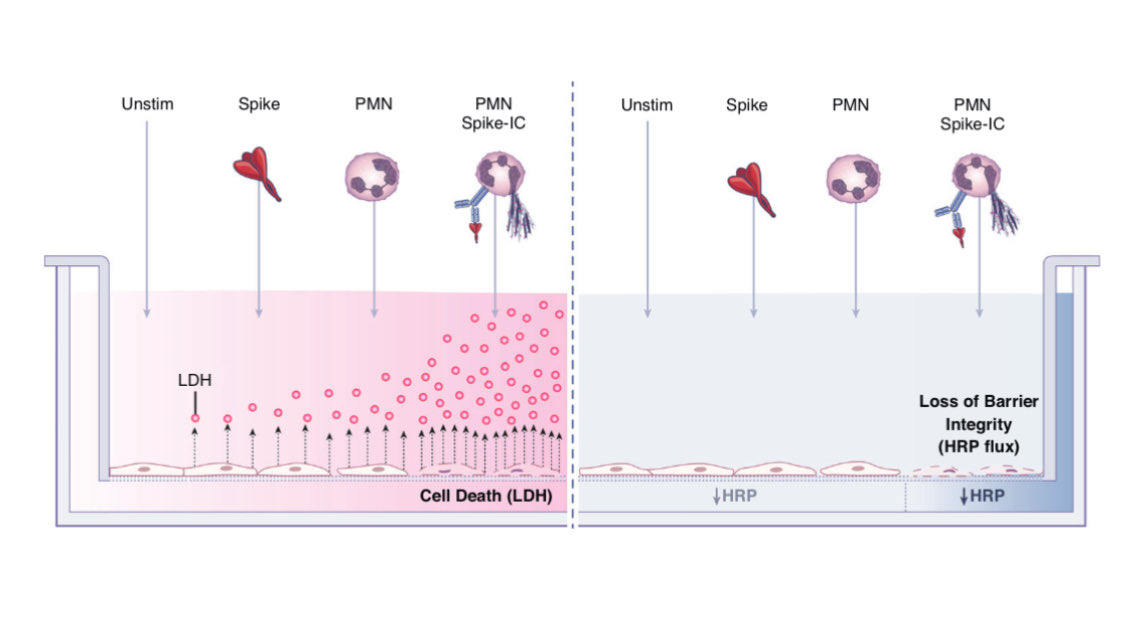
Breaking: New PolyBio-supported Study Identifies Microclots, Endothelial Injury Markers and Neutrophil Activation in Children and Young Adults with Long COVID
A new study supported by PolyBio Research Foundation studied children and young adults with Long COVID, providing evidence linking endovascular inflammation, increased quantity and size of fibrin-amyloid “microclots,” and neutrophil activation, and finding detectable Spike protein in a subset.
https://t.co/hOR1mWHRdc
@dysclinic 👏🏻 Impressive group DrB! Dr Peters dx’d me w/uro comorbs of hEDS, POTS, MCAS, SFN. He has helped many of us. Thrilled to know he included your perspective. Maybe Neurology will hear of your presentation and bring you back for a Dys/POTS talk at the Wm Beaumont med school 😉




























![gymrat_bookworm's tweet photo. "When you start treating hypermobility as the fifth vital sign, [the list of differentials] completely changes."
--------------
"You know what's wild, as a GI doctor, there was things I were taught in fellowship that I would never see in my career, Median Arcuate Ligament Syndrome (MALS), Superior Mesenteric Artery Syndrome, Retrograde Cricopharyngeus Dysfunction (R-CPD), are zero [incidence]. Really, really rare, but once you start treating people with hypermobility, you realize that they aren't that rare anymore. In fact, they are quite common, and it completely changes the way you think.
In general, when we think "peptic ulcer disease", we think "h pylori". When we hear "bloating", we think "celiac disease, lactose tolerance." However, when treating hypermobility, the menu completely changes. You are thinking, "structural instability, motility issues, vascular compression,."
So yes, in general, these conditions are rare, but not in people with hypermobility, which makes me think we don't have a rare disease problem, we have a pattern recognition problem."](https://pbs.twimg.com/media/HHsW7WvWUAIPY-8.jpg)