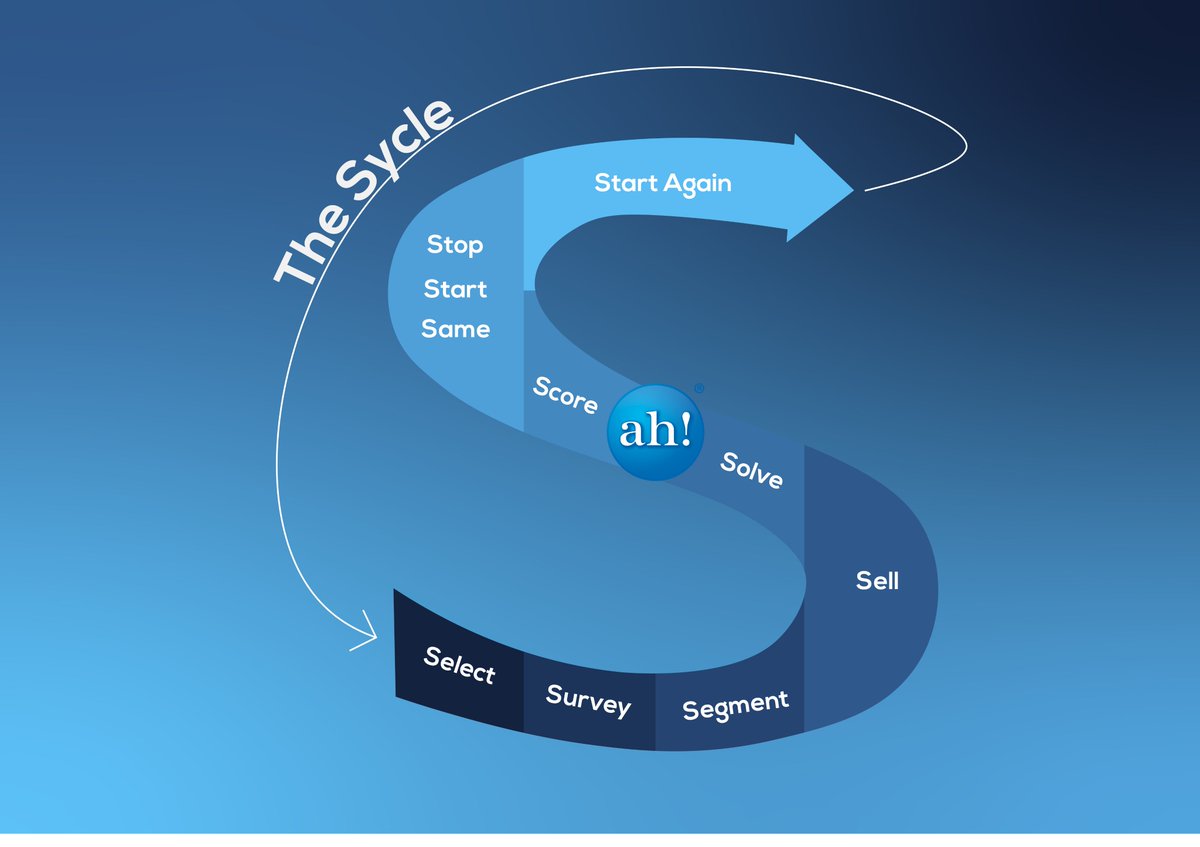
Ready to stop settling for mediocre outcomes? Let’s audit your PopHealth Sycle(tm).
👇 Read how to execute a true Stop/Start/Same review:
https://t.co/gdphg3YkIZ
#PopulationHealth#HealthcareROI#ContinuousImprovement
People, Health, Research, and Reality 🤔 | PopHealth Pulse
"Show me the data." A fierce defense of scientific research funding, a takedown of medical quackery, and a timeless lesson from an early HIV/AIDS physician.
https://t.co/d2iYNJK6eG
#PublicHealth#EvidenceBasedMedicine
Moving from descriptive data to predictive AI changes the game in population health management.
Stop just tracking, start scoring where your patients are going. Here’s how to master leading vs lagging indicators: This week's PopHealth Pulse, The SCORE Step https://t.co/UfdgJIZaPC
@EPotterMD Yes, big problem and there's more blame to go around than just upcoding for the broken system ... 20 years later, and these are still issues "The Word of those with Whom We Do Business"
https://t.co/g1pnmdAFja
Precision medicine shouldn't just be for individuals—it needs to work at scale. 📈
Step 3 of the Population Health Sycle™ the Segment phase. Move beyond basic risk scores by using AI personas and SDoH data to find the "why" behind the utilization.
https://t.co/7VR5SwjaLV
Hey @mcuban Try the Health City Cayman Island Approach of Dr. Devi Shetty... "A Bill You Can Understand: One Page, One Line, One Price" https://t.co/kbYIDFjNdR
The greatest problem in healthcare ? Hospitals, even market dominant hospitals, won’t walk away from the big ins companies that underpay, late pay, clawback, deny claims, waste their time in denial appeals, and require them to pay up to 8 pct of revenue to RCM consultants so they think they are getting what they are owed.
Here is the crazy part. The ins companies ARE NOT THE ONES ACTUALLY PAYING THEM on commercial plans. Employers are.
60 pct of employees get their insurance from their self insured employers. The ins carrier is just a middleman that pretends to add value.
All the clinical “value” they add, the hospital could do better, for both medical and pharmacy.
Most hospitals have no idea whether they make or lose money with their big ins contracts. They are just afraid to lose patient flow.
But. They actually know which companies their patients are coming from. They actually know or can find out, how much more the employers are paying the ins company, than what the ins company pays them (the spread, just like in pharmacy )
And to make it worse, those ins companies negotiate their rates as a discount from the “charge master “, which is like WAC in pharmacy. Just a made up list price.
Because the hospitals are afraid or too uninformed to walk away from these deals, the hospitals use the inflated charge master prices as the basis to charge uninsured , or out of network , or insured but not covered for their care, at charge master rates. Which of course the patients can’t afford. And it crushes their finances or they go without care
I’ll summarize. Employers , and their members , are paying far more than they should to companies they don’t like working with , that effectively rip off both the employer and hospital , and they could eliminate the middlemen if they went directly to to the employer.
It’s so simple. Sell your services to the employers that use your services at a price that is less than what nine companies charge for your services and you will make MORE money and employers will save a ton
And if they did this, they could dump the chargemaster and reduce the price they bill patients when they are at their most vulnerable
But they don’t want to change. And don’t get me started on how much hospitals over pay for drugs and devices because of the GPO deals they do. It’s just stupid.
Which in turn leads to the hospital being a bad actor with 340b , facilities fees and afraid of their doctors who demand they pay more for things like glue and implants so they can get vacations.
If you are a politician and reading this. Now you know why this is so fucked up and it’s not about capping rates. The insurance companies are smarter than you. They will just move the money to other places. It’s not about giving money to patients. You can’t shop for care from hospitals that are too gutless to walk away from the ins companies that distort all of healthcare economics
Go to your local hospitals , particularly those at risk of closing and ask for their profitability by carrier. Fully burdened. Ask how much they spend on RCM and consultants. In many cases they could survive if they ran like a real business and hired execs that could do the work rather than just manage consultants. They could work out contracts in their communities rather than with ins companies and benefit everyone.
The middlemen are not needed. Get rid of them
CMS is finally timing the "black hole" of drug prior auths ⏱️ But we’re also cutting the NIH budget?
MAGA-MAHA-HAHA (Hurting America’s Healing Arts)✂️🔬
You can't "Make America Healthy" by defunding the research.
👉 https://t.co/GHQ78JLVvd
#PopHealthPulse#NIH#Healthcare
@BrentAWilliams2 So true, and at the same time let's not ask or fund them to fix it.... "Running to the Ball: The Shiny Object of Social Determinants ot Health". https://t.co/FMInTAyOgw
Is your population health strategy lagging? Get the momentum back with the PopHealth Sycle. From risk stratification to patient engagement, we help you master every phase of the wheel. Let’s get started. ah! 🎡 #AccountableHealth#Strategy#MedTwitter
In 2026, "Value" is shifting from administrative precision to real-world outcomes. Whether you're navigating CMS ACCESS in the States or integrated care models abroad, the goal is the same: proactive engagement. Get the blueprint w/ #AccountableHealth ah! 🏥 #VBC#PatientOutcomes
The math is simple: Better outcomes = better margins. The PopHealth Sycle is our blueprint for sustainable Value-Based Care. We don't just consult; we calibrate your entire operation for long-term health. ah! 🏥
Contact Us https://t.co/sNr2rZiPpE
#VBC#PopHealthSycle#ROI
Burnout happens when systems fail, not people. The PopHealth Sycle(tm) streamlines workflows by identifying high-risk populations before they become high-cost crises. Work smarter, not harder, with #AccountableHealth. ah! 💡
#HealthcareAdmin#SycleSuccess
Healthcare isn't linear; it’s a cycle. If your data isn't leading to action, and your action isn't improving outcomes, you’re stuck. Break the loop with the PopHealth Sycle (tm). Let #AccountableHealth show you how to close the gaps. ah! 🔄
#PopulationHealth#HealthValue
Your team is working hard, but are they working smart? Optimize your practice’s workflow and boost efficiency with #AccountableHealth. We’ll help you find that a-ha! moment of peak performance. #healthcare consulting #efficiency
@EvanKirstel I still have my 1984 Compaq ⬆️$2,000. It was fully loaded: 512K of RAM, dual floppies. Minor upgrade to a 30 mb hard drive years later. Still have all the software. Wordperfect, Lotus 123, spellchecker, Flight Simulator, Gato, CPM, DOS, & more. Lugged through many airports 😂
CMS handed $26B back to MA plans, but is it a win for anyone but their P&L? 🤔📉
This week’s PopHealth Pulse is live:
🔹 MA Rate Pivot vs.Scrutiny
🔹 Record-Low Fertility
🔹 Long COVID Heart Risk ❤️⚡
🔹 DEHP & Premature Births 👶⚠️
Read here: https://t.co/Qhl7O0n0zQ
#PopHealth