Acute Care of Elderly (ACE) Practitioners, University Hospital Ayr. RMN, RN and OT providing CGA in the acute setting. Some of our thoughts and interests.
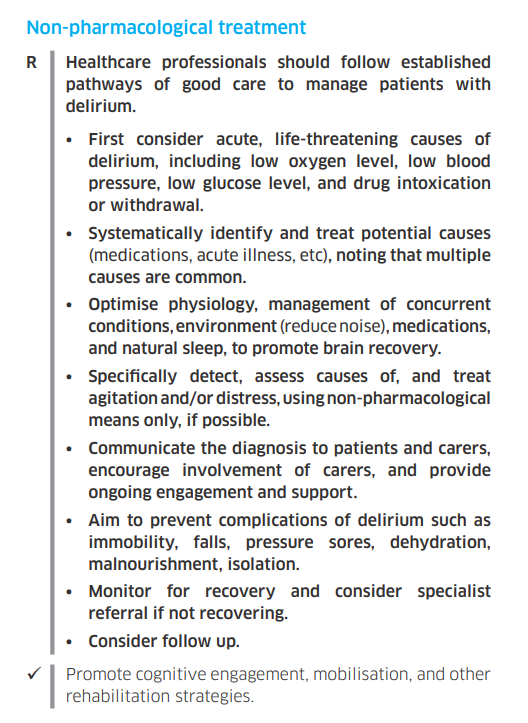
⚡ SIGN Guidelines on #Delirium = one of the few recent comprehensive guidelines in the field globally.
🆗 Here is the section on #delirium treatment.
Quick reference guide (free):
🔗 https://t.co/9Txcl8tSIK
The ‘React to Falls’ App is an evidence-based smartphone resource that enables #carehome staff to tailor actions to support each individual resident. It includes practical tips and examples of what staff can do, whilst enabling residents to remain active https://t.co/zAYZmsIMgy
We argue for diagnosing delirium, by the way. "Misdiagnosis ... is characterized in medicine as diagnostic error and not under-recognition. If delirium were considered a diagnosis, its diagnostic error rate would be an unacceptably high rate of around 70%"
I’m worried about seniors in this coronavirus outbreak. What’s the best way to keep them safe? The Globe asked. My reply, with part of the tricky conversation about people living with late-stage dementia. Where does Covid19 fit in allowing a natural death? https://t.co/0twspoPSVm
Delighted to announce that the Scottish Delirium Association teaching day 2020 is on 18 June at Glasgow Caledonian University in central Glasgow.
Keynote: Prof Graham Ellis - National Clinical Lead for Older People.
See below for details.
RT & share with colleagues!
#delirium
In our experience constipation is more likely to the main contributing factor for delirium (if you only have one cause you’re not looking looking hard enough)
@DrTerryQuinn Also something about how common a non-infective delirium is - stop giving trimethoprim and start sorting laxatives, analgesia, reading glasses and hearing aids etc
I’ve told this before but it’s a good one.
‘We’ve lost a patient. You need to come’
‘As in died?’
‘No. Lost’
‘How do you know?’
‘We can only find a slipper’
As I walked to the ward, a fox headed out the back door with a pink slipper in its mouth.
Pt was in the toilet. Barefoot.
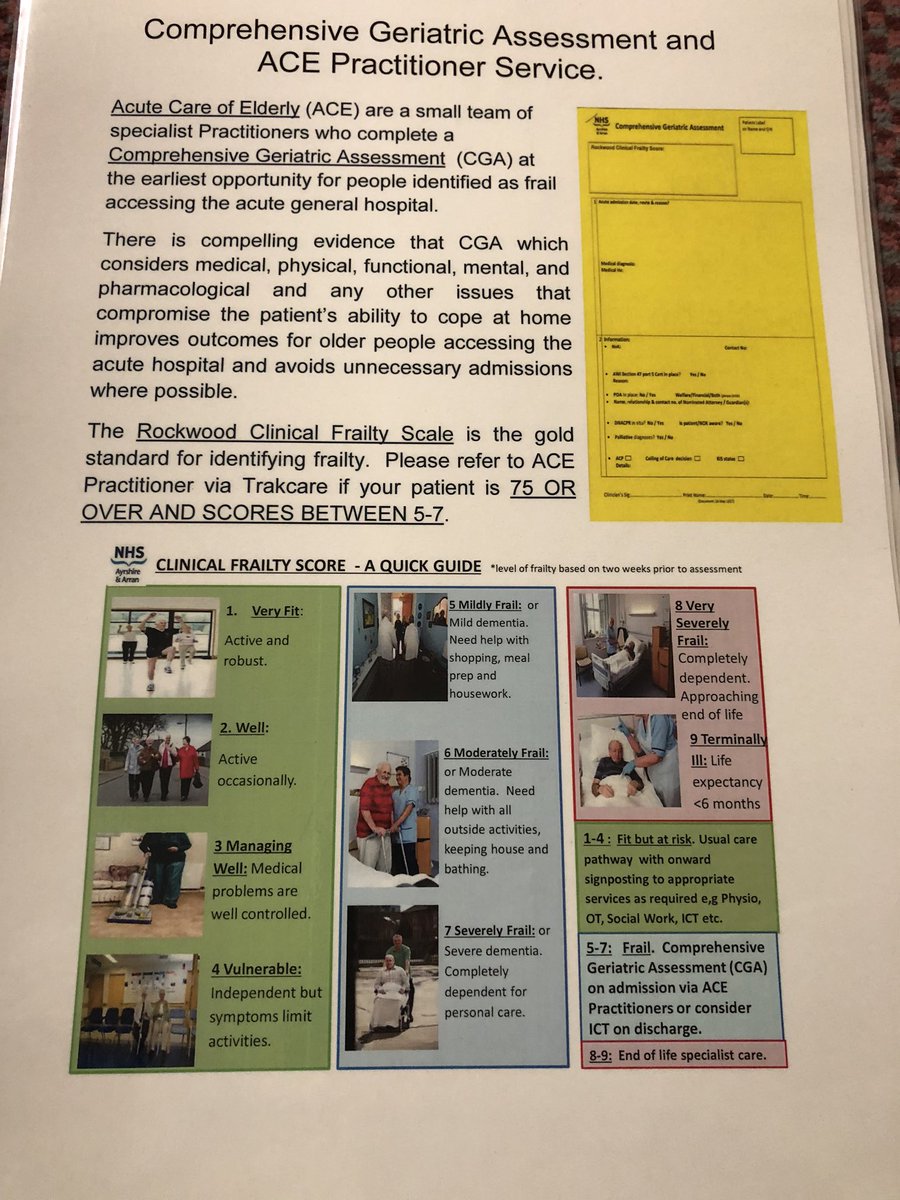
1/9 Was asked good questions re: the Clinical Frailty Scale, so this Tweetorial. Case 1: 84 year old woman; hypertensive, hypothyroid (meds for each) IADLs OK. Walks 5-7 km/day + 15km/week to visit her sister. "Would you still classify her as CFS =3 due to her chronic diseases?"