@LoriMills4CA42 , what you're doing this week matters more than the outcome of any single hearing. This is a war against cancer, and you're walking straight into one of its most important battles, not for a stock, not for a headline, but for every family staring down a diagnosis after being told there's nothing left to try.
We don't know if we win this one. Nobody does. But we show up and we fight anyway, because restoring the immune system instead of only poisoning the tumor is the right side of this fight, and history tends to remember the people who stood there first. People like you and @DrPatrick and every single person who cares.
So go tell them your husband's story. Tell them about the families who can't afford to wait. You go fight girl. Let's make this battle count.
Thank you so much for your incredible support and continued generosity. It’s finally happening!
Andrew and I are flying to Washington, D.C. tomorrow, and I will be testifying before the FDA to help get natural killer cells and ANKTIVA released and available to all cancer patients. I can't promise it will happen, but I can promise I'm fighting for you.
Please keep us in your prayers.
Your kindness has truly meant the world to us. We would not be able to make this trip without your support, and we are so deeply grateful.
Here’s a quick update...
$IBRX A blue whale carries about a thousand times more cells than you do. Every one of those cells can, in principle, turn cancerous. By the plain arithmetic of cancer, a creature that large should be riddled with tumors long before it ever reaches the open ocean.
It isn't. Whales live eighty, ninety, past a hundred years, at a size that should be a death sentence, and they do it while barely getting cancer at all.
Biologists have a name for the puzzle: Peto's Paradox. And the answer, as far as we understand it, is that evolution got there first. Whales carry extra copies of the genes that suppress tumors, and DNA repair machinery far more precise than ours. Nature ran the experiment over fifty million years and solved a problem we are still losing to.
On Saturday night, @DrPatrick who built ANKTIVA pointed at that exact fact and posed a riddle. Then he walked away from it.
THE ANTIBODY NATURE ALREADY BUILT
His first message: "Ever wonder why camels, llamas, sharks and whales don't often get cancer?"
The whales are the lesson in resistance. The camels and the sharks are something else: they are the source of a tool.
Camels and llamas make a kind of antibody no human makes. Where ours are large and Y-shaped and built from four pieces, theirs come stripped down to a single small piece, about a tenth the size. Scientists named the working tip of it a nanobody. Sharks evolved their own version of the same trick, separately, in their own branch of the tree of life.
These tiny antibodies are sturdier than ours. They reach into folds and pockets on a target that a full-size antibody is too bulky to touch. They are far easier to engineer. Sharks have been carrying them for something close to four hundred million years, longer than there have been trees on land.
WHAT NATURE ACTUALLY PROVED
Notice how carefully he said it. He wrote that these animals "don't often get cancer," not that they never do. That one word, often, is the honest word, and it is worth pausing on, because the shark has a dark history here. In the 1990s an entire industry sold ground shark cartilage to desperate cancer patients on the false promise that sharks don't get cancer and so their cartilage must cure it. It was a scam, a cruel one, and it was wrong twice over: sharks do get cancer, and the cartilage cured nothing. Soon-Shiong is not repeating that lie. He chose "often" precisely because he knows the difference, and what he is pointing at has nothing to do with cartilage. It is narrower and far more interesting. The shark and the camel did not cure cancer. They invented a better antibody. And the whale is proof that cancer can be held at bay at scale, by a body that evolved the defenses to do it.
Nature, in other words, has already written the proof of principle. Not for a drug. For an idea.
His second message tells you what he wants to build from it: "From Nanobodies to Nantibodies. The goal: ADCC and ADCP. I know that's a foreign language, but I'm sure many will figure that out."
So here is the answer, using only his own words, public biology, and his own company's filings.
THE TWO GUARDS
A week ago, in a post called THE GUARD CANCER CANNOT FOOL, we walked through how the body polices itself. Two cells do the work.
The T cell is an inspector. It can only attack a cell that displays an ID badge, a surface marker called MHC-I, showing what is inside it. Cancer's oldest trick is to take the badge down. No badge, nothing to read, and the inspector lets it pass.
The NK cell runs the opposite rule. It kills any cell that is NOT wearing the badge. So when cancer drops the badge to dodge the inspector, it lights itself up for the NK cell. The move that beats one guard arms the other.
ANKTIVA's job, written into its FDA label, is to wake both of those cells and multiply them. It is an IL-15 receptor agonist. It arms the guards. That was the story, and it was true.
But it was not the whole story, and the riddle is Soon-Shiong telling you where the story breaks.
THE CELL THAT BEATS BOTH
Both guards key off the same badge, in opposite directions. The inspector needs it present. The NK cell needs it absent. So picture the smartest cancer cell of all. It keeps the badge on. And rather than hide from the inspector, it disarms him directly, by waving a chemical flag that orders him to stand down, a flag he is built to obey.
That cell wears the badge, so the NK cell waves it through. It disarms the inspector, so the T cell holds fire. It walks through both checkpoints in the uniform of a healthy cell.
Think of the badge as a fighter jet's transponder, the coded signal that tells your own air defenses "friendly, hold fire," so they don't shoot you out of your own sky. MHC-I is exactly that, for your cells. The clever cancer keeps broadcasting a perfect friendly signal while it jams the one inspector who could see through it. The guns stay silent. It crosses the line untouched.
THE ONE THAT GOT AWAY
Now give that cell a name you know. In a real person, the cell that survives both guards is the one that comes back. It is the recurrence. It is why a patient can finish treatment, ring the bell, scan clean, and then, a year on, hear the word again. The body did not fail to fight. It fought, and it won almost everywhere. But one cell kept its badge, jammed the inspector, and broadcast friendly the whole way through, and one cell is enough.
Arming the guards harder does not reach that cell. A stronger gun still will not fire on something broadcasting friendly. You do not need more firepower. You need a way to mark the enemy that does not depend on the signal it is sending.
THE FORWARD OBSERVER
That is the second half of the riddle, and it rests on a mechanism that is sixty years old.
ADCC, antibody-dependent cellular cytotoxicity, was first described in 1965. It is in every immunology textbook. It is bedrock. Here is how it works, plainly.
- An antibody grabs a specific marker on a target cell with its two tips. Its tail sticks out
- The NK cell carries a receptor, called CD16, that grabs antibody tails
- When CD16 locks onto the tail of an antibody that has tagged a cell, the NK cell kills that cell
In plain language: the antibody is a forward observer who paints the target with a laser. CD16 is the targeting receiver on the NK cell that homes on the paint. And here is the line that closes the gap the recurrence slips through. CD16 does not read the badge. It does not hear the friendly signal. Once a cell is painted, the NK cell fires, no matter what that cell is broadcasting.
ADCP is the same idea with a different soldier. Instead of an NK cell killing the painted target, a macrophage eats it. A second weapon, locked onto the same paint.
The disguise that beat both guards, the badge held high and the inspector jammed, stops working the instant a forward observer paints the cell by a mark it cannot fake.
EVERYTHING IS ALREADY ON THE TABLE
Here is why he could pose the riddle and trust that many would solve it. Every piece is already sitting in plain view.
The antibody format is real, and ancient. The shark has carried it for four hundred million years.
The killing mechanism is real, and old. ADCC has been understood since 1965.
The effector is real, and already built. ImmunityBio engineered a natural killer cell it calls haNK, designed to overexpress "high-affinity CD16" so that it can, in the company's own words, "directly bind to IgG1-type antibodies and enhance cancer killing efficacy" through ADCC. They built the perfect ADCC shooter and have been holding it, waiting for the right antibody to paint the targets.
The synergy is real, and published. ANKTIVA began life under the name ALT-803. Same molecule. In 2014, in the journal Blood, researchers showed that ALT-803 made NK cells markedly better at antibody-directed killing. Paired with rituximab, a real cancer antibody, it boosted NK-cell ADCC against lymphoma in the lab, and in mice the combination sharply reduced the cancer in the bone marrow and beat either drug alone on survival. A later study showed the same effect pairing it with cetuximab against head-and-neck cancer. The exact molecule that is now ANKTIVA was shown, more than a decade ago, to sharpen the very mechanism the antibody depends on.
And the antibody itself is no longer just an idea. Immunotherapy NANTibody LLC is listed as a wholly owned ImmunityBio subsidiary in the company's most recent annual report to the SEC. The entity has been on the books. Saturday night, he switched on the lights.
Read the dots in a row. Nature proved the format. The textbook proved the mechanism. A 2014 paper proved his own molecule supercharges it. The company already built the shooter. The subsidiary already exists. The antibody finds the cell that got away. ANKTIVA wakes the shooter and makes its aim deadlier.
It is, on paper, a complete machine.
THE ONE STEP THAT HASN'T HAPPENED
And here is the truth the science demands we say out loud, because everything above is the blueprint, not the building.
This combination has not been tested in a patient. The Nantibody platform has no published trial, no announced results, no approval. Every piece has been proven on its own. Nature proved the antibody. The textbook proved the mechanism. The lab proved the synergy in a dish and in a mouse. The company proved it could build the cell. But no one has yet put the whole machine together, aimed it at a human cancer, and shown that it works.
That is not a small caveat. It is the entire distance between a beautiful idea and a treatment a person can be given. Biology is littered with machines that were perfect on paper and failed in the body. Until the trial runs, this is a hypothesis with an extraordinary pedigree, and nothing more.
But sit with what that pedigree actually is. The proof of principle is not a model or a slide. It is a shark that has used this antibody for four hundred million years. It is a whale that holds cancer at bay at a scale that should overwhelm it. It is a mechanism science has trusted since 1965, a molecule already published doing the job, an effector cell already engineered to receive it, an entity already incorporated to carry it.
The parts are all on the table. Nature laid most of them there. The only thing that has never been done is to assemble them on purpose and point them at the thing that is killing people. And somewhere right now there is a patient who responded, who rang the bell, who is waiting on exactly that one step that has not yet been taken.
THE GUIDANCE SYSTEM
For two years, the story of this medicine was about waking the immune system up. ANKTIVA armed the guards. The guards caught the cancer that hid by dropping its badge, and the cancer that showed it.
The riddle is about the one that got away. The cell that keeps its badge, jams the inspector, and broadcasts friendly the whole way through. The cell that becomes the recurrence. You do not beat that cell with more firepower. You beat it with a forward observer who paints it by a mark it cannot fake, and a shooter that fires on the paint instead of the signal.
The cancer's entire survival depended on one thing. Broadcasting "I am one of you." The Nantibody does not read the broadcast. It reads the paint.
Nature already proved it can be done. He said many would figure out the rest. Now you have. What is left is not to imagine the machine. It is to build it, and to test it, before the next bell rings.
$IBRX In a bladder somewhere this weekend, one cancer cell is doing the thing every cancer eventually learns to do. It is making itself invisible to the immune cells that should kill it. By the time enough cells have done it, the drug the patient is on stops working.
On Friday, the company that makes one of the drugs used in this disease published comparative data. The numbers showed it did not statistically beat J&J's competing therapy on response rate.
Here is what Friday actually measured, the bigger question it did not, and who is building the only drug cancer cannot fool.
WHAT FRIDAY MEASURED
On Friday May 22, 2026, ImmunityBio released two press releases tied to ISPOR 2026, a health-economics conference in Philadelphia. Both compared ANKTIVA plus BCG against J&J's TAR-200, in the same FDA-approved indication both drugs hold today: BCG-unresponsive non-muscle-invasive bladder cancer with carcinoma in situ.
The same head-to-head comparison had already been presented three days earlier at the AUA Annual Meeting on Tuesday May 19. The efficacy and safety numbers from that May 19 presentation, exactly as the company published them:
- 12-month complete response rate: 49.2% for ANKTIVA plus BCG vs 45.9% for TAR-200; odds ratio 1.14 (95% CI 0.61 to 2.15) -> not statistically significant
- Treatment-related adverse events, any grade: 61.7% vs 83.5%; odds ratio 0.32 (95% CI 0.15 to 0.67); E-value 5.70 -> statistically significant, roughly 68% lower odds of any adverse event
In plain English. About half of patients in either trial reach a complete response - meaning the cancer is no longer visible on cystoscopy or biopsy. The three-percentage-point edge for ANKTIVA plus BCG sits inside the confidence interval. The honest reading on efficacy: equivalent.
What ANKTIVA plus BCG did do in the same comparison was meet a much higher bar on safety. Sixty-two percent of patients had a treatment-related adverse event of any grade, versus eighty-four percent on TAR-200. That difference is statistically robust. It is not a rounding artifact.
Friday's two PRs added the economic layer on top of that comparison. Vanderbilt urologist Ruchika Talwar ran the same indirect comparison through a multi-state Markov cost model over three years in a Medicare population. The results, exactly as the company published them:
Cost savings vs TAR-200 per complete responder: $313,775 at Year 1, $282,013 at Year 2
Cost savings vs TAR-200 per cystectomy avoided: $109,622 at Year 1, $151,438 at Year 2, $60,393 at Year 3
In plain English. For every patient who responded to ANKTIVA plus BCG, the system was projected to spend about three hundred thousand dollars less in the first year than it would have spent reaching the same response with TAR-200. For every cystectomy avoided - the surgical removal of the bladder - the projected savings ranged from sixty to one hundred and fifty thousand dollars across the three modeled years. The driver, per the press release, is straightforward: ANKTIVA plus BCG carries a lower drug-acquisition cost than TAR-200.
Tied on efficacy. Safer. Cheaper. That is what Friday's data is.
WHAT THE CAVEATS ARE
The comparison is what is called an unanchored matching-adjusted indirect comparison. It weights individual patient data from one company's trial against aggregate statistics from another company's trial. The patient populations are statistically matched. The drugs were not given head-to-head in the same study. ImmunityBio's own Limitations section on the May 19 press release said the analyses "should be interpreted with caution."
Both drugs were originally approved on single-arm Phase 2 trials. Five drugs in this disease across twenty-seven years, all five on single-arm trials, under the FDA's own 2018 guidance. The methodological floor is roughly the same on both sides.
What survives the caveats is real, and bounded: a tie on efficacy, a meaningful edge on safety, an edge on cost. In one slice of the disease.
THE QUESTION FRIDAY DOES NOT ANSWER
The headline frame on Friday was: does ANKTIVA plus BCG beat TAR-200 in salvage CIS? The honest answer, after Friday, is no. They are tied on response rate; ANKTIVA plus BCG wins on side effects and price.
But that frame is the small question.
The big question is the one the man with bladder cancer should actually want answered. It is: of every drug being developed for his disease, which one is built to handle what cancer actually does to evade immune therapy? Because that is what decides whether the response lasts.
This is the question Friday did not measure.
HOW THE CANCER HIDES
This is textbook immunology, not a company theory. T cells, the immune cell most cancer immunotherapy aims at, can only see a tumor cell if the tumor wears a surface ID tag called MHC-I. Tumors evolve. A documented mechanism of resistance to checkpoint-inhibitor drugs like Keytruda and Tecentriq is that the tumor stops making the tag. No tag, no T-cell vision. The cancer slips past.
Now the elegant part, known to immunology for decades. The NK cell, a different immune cell, runs the opposite logic. A normal cell shows the tag, the NK cell passes it by. A cell that has dropped the tag screams "missing self" - and the NK cell destroys it.
The tumor's classic trick against T cells is the exact signal that turns NK cells loose.
A drug that revs up only T cells gets fooled the moment the tumor drops its tag.
A drug that revs up both T cells and NK cells does not. That is what an IL-15 receptor agonist does. Per the ANKTIVA FDA label, section 12.1: ANKTIVA trans-presents IL-15 to the IL-15 receptor on both CD4+ and CD8+ T cells AND on NK cells. Label fact, primary source.
This is the question THE MISSING LINK, the prior post in this series, walked through in mechanism terms. The question for any drug in this disease is no longer "does it activate the immune system?" It is: "which arm of the immune system, and what happens when the cancer hides from that arm?"
WHO IS BUILDING WHAT
There are five Phase 3 or registrational trials in BCG-naive non-muscle-invasive bladder cancer that have surfaced on https://t.co/j6TST0ZdM2 as of this Sunday. They are the field. They are who the patient and his urologist will eventually have to choose between.
- ALBAN (UNICANCER, Europe): atezolizumab plus BCG. Anti-PD-L1, releases the T-cell brake. Engages T cells. Does not engage NK cells.
-KEYNOTE-676 (Merck): pembrolizumab plus BCG. Anti-PD-1, releases the T-cell brake. Engages T cells. Does not engage NK cells.
- QUILT-2.005 (ImmunityBio): ANKTIVA plus BCG. IL-15 receptor agonist. Engages both T cells AND NK cells.
- ADVANCED-3 (Protara): TARA-002 vs chemotherapy. Broad immune stimulator from an inactivated bacterial preparation. Engages multiple immune cell types indirectly; not specifically dual-axis by design.
- SunRISe-3 (J&J): TAR-200 with or without cetrelimab vs BCG. Sustained-release gemcitabine chemotherapy plus optional anti-PD-1. Engages T cells in the cetrelimab arm. Does not engage NK cells.
Four out of five hit only one of the two guards, or none specifically. One hits both, by mechanism written into its FDA label.
This is not a prediction about which drug will read out positive or get approved. PD-1 and PD-L1 inhibitors have worked in many cancers; they may well work here. This is a different point: of the registrational programs in front of regulators, only one is designed for the failure mode the science of this disease has known about for decades.
TWICE AS LONG, MEASURED
The two-guard advantage is structural. It also has a number under it.
ANKTIVA's mechanism, per the FDA label and the company's own published description, does more than activate NK cells. It also drives "the generation of memory killer T cells that have retained immune memory against these tumor clones." That is the durability mechanism. The immune system is not just hitting the cancer once. It is remembering it.
On May 19, 2026 - the same week as Friday's headlines - ImmunityBio also presented an indirect comparison against nadofaragene firadenovec, a gene therapy approved in the same indication as ANKTIVA. Two drugs, same disease, same failure population, same regulatory pathway. The published numbers, from the company press release verbatim:
- Median duration of complete response: 22.1 months for NAI plus BCG vs 9.7 months for nadofaragene
- Difference: 12.45 months (95% CI 8.17 to 17.09)
- Hazard ratio for end of response: 0.57 (95% CI 0.34 to 0.95) - statistically significant
- Cystectomy-free survival HR: 0.40 (95% CI 0.21 to 0.75) - sixty percent reduction in cystectomy risk, statistically significant
- Overall survival HR: 0.85 (95% CI 0.22 to 3.31) - not statistically different
In plain English. When ANKTIVA plus BCG works, it works more than twice as long as the closest gene-therapy comparator before the cancer comes back. The cancer is sixty percent less likely to require removal of the bladder. These are statistically significant findings, from the same unanchored-MAIC methodology Friday's TAR-200 comparison used. The same caveats apply, including the honest one: with the available follow-up, overall survival between the two arms is not yet statistically different.
The point of these numbers is not that they prove superiority. The point is that they are the consequence of the mechanism. Memory T cells generated by IL-15 signaling are why the response lasts. The drug's label says it. The 22.1 versus 9.7 month comparison shows it.
NO ONE ELSE IS BUILDING FOR THIS
No other drug in the BCG-naive registrational field uses this mechanism. Pembrolizumab and atezolizumab release T-cell brakes through PD-1 or PD-L1 blockade. They do not directly activate NK cells. They do not by mechanism generate IL-15-driven memory T cells. They are not durability machines; they are brake-release machines.
Cetrelimab in J&J's combination arm is the same drug class. TAR-200 alone is sustained-release gemcitabine - cytotoxic chemotherapy. It kills dividing cells. It does not engage immune memory. TARA-002 is a broad immune stimulator without dedicated dual-axis IL-15 signaling. And BCG alone induces local inflammation but does not specifically restore the lymphocytes the disease has depleted.
Five trials. One mechanism designed for the failure mode immunology has known about for decades. Two of the other four ride the T-cell axis the cancer learns to evade. The remaining two work either through chemotherapy that does not engage immune memory at all, or through broad immune stimulation that is not specifically built around the missing-self logic.
WHAT WAS ALREADY ON THE RECORD
That broader case has been built across earlier work in the receipts library, post by post.
THE MISSING LINK on May 18 walked through the three blood lines: chemotherapy depletes red cells, neutrophils, and lymphocytes. Drugs exist to rebuild the first two. For the third, the cancer-killing one, nothing existed until ANKTIVA.
THE 7X NUMBER on May 7 walked through the JAMA Zidar data on lymphocyte counts and mortality. Patients in the lowest-lymphocyte category carry roughly seven times the mortality from influenza and pneumonia, four times from cardiovascular disease, and three times from cancer.
The molecule the FDA approved in 2024 is the one the NCI ranked first in 2007 across more than a hundred immune candidates.
THE CALENDAR
Each trial's primary completion, sourced to the https://t.co/j6TST0ZdM2 record on May 24, 2026:
- ALBAN (atezolizumab + BCG, UNICANCER): June 2025. Already past. No US filing program; investigator-initiated. Results not yet formally published.
- KEYNOTE-676 (pembrolizumab + BCG, Merck): July 31, 2026. Trial-level primary completion. The trial has both a BCG-unresponsive cohort and a BCG-naive cohort; the BCG-naive endpoint is event-free survival and may read later than the trial-level date.
- QUILT-2.005 (ANKTIVA + BCG, ImmunityBio): September 30, 2026. 129 days from today. ImmunityBio has guided a Biologics License Application filing in Q4 2026.
ADVANCED-3 (TARA-002 vs chemo, Protara): April 2028. Trial has not started enrollment yet.
SunRISe-3 (TAR-200 +/- cetrelimab vs BCG, J&J): September 18, 2029.
Three of the five primary completions fall inside the next eighteen months. The other two fall in 2028 and 2029.
ANKTIVA is not first. Merck's trial reads out first at the trial level. ANKTIVA is the only one in the field that is designed, at the receptor level, to catch a cancer that hides from T cells.
WHAT FRIDAY IS AND IS NOT EVIDENCE ABOUT
Friday's data is from a different trial (SunRISe-1, not SunRISe-3), in a different patient population (BCG-unresponsive, not BCG-naive), against a different drug pairing (TAR-200 alone, not TAR-200 plus cetrelimab), on a different endpoint (response rate, not event-free survival).
The bear reading of Friday extrapolates an indication-1 efficacy tie into a forecast about the bigger BCG-naive franchise. The math does not support that extrapolation. Different evidence.
A bull reading that extrapolates the IL-15 mechanism advantage into an approval forecast also does not work. A trial is not an approval. A mechanism written into a label is not the same as a positive readout. Both extrapolations are unjustified.
What is true today is this:
- In the indication both drugs hold, ANKTIVA plus BCG and TAR-200 are equivalent on efficacy, ANKTIVA plus BCG is safer, and ANKTIVA plus BCG is cheaper. That is the honest read of Friday.
- In the indication ANKTIVA's sBLA was accepted for last Tuesday, May 19, 2026, TAR-200 has no presence. ImmunityBio gets to that papillary-only label first if January 6, 2027 goes well. The previous post in this series, THE LETTER, walked that one through.
- In the indication that matters most, the BCG-naive first-line setting, five trials are running. Only one is designed to hit both NK cells and T cells.
None of that is a forecast. All of it is a structure.
WHAT THE PATIENT IS ACTUALLY WATCHING
For someone whose loved one has this disease, four things are worth holding:
- The cancer may try the same trick cancer always tries. It may stop showing the tag. If the patient is on a drug that only sees the tag, the drug stops working.
- The drug their urologist can offer today, ANKTIVA plus BCG, activates NK cells by mechanism. The FDA label says so on section 12.1.
- The Phase 1 origin program for that drug, dosed in 9 patients starting in 2014, reported 100% complete response at 24 months. Eight of those nine were still in remission at year 8.8.
- The randomized BCG-naive trial that grew out of those nine patients, in 369 patients, reaches its primary completion on September 30 this year.
What matters is not the headlines. It is the calendar.
THE GUARD CANCER CANNOT FOOL
There is a question, in this disease, that the headlines did not ask Friday. It is not whether ANKTIVA plus BCG beats TAR-200 on a cost-per-responder line. It is whether the drug the patient takes still works after the cancer has done what cancer always does.
Of the five drugs racing for the BCG-naive label, one is built to be the answer to that question by mechanism. Not by marketing. By label. By trans-presentation of IL-15 to two cell types instead of one. By a guard the cancer cannot fool, on top of the guard it can.
Cancer learns to drop the tag. Four drugs in trial miss the trick. ANKTIVA was built for it.
ANKTIVA's BCG-naive trial in 369 patients reaches its primary completion in 129 days, on September 30, 2026
Great question. The patents cover the COMBINATION (ANKTIVA + an approved BCG strain), not any specific BCG strain.
ANKTIVA + TICE (Merck's strain, the only US-approved BCG since 2012): the existing approved use today, covered.
ANKTIVA + Tokyo-172 (Japan BCG Lab's strain): covered if/when the FDA approves that combination. The May 18 SEC 8-K disclosed an exclusive US Development and Supply Agreement with Japan BCG Laboratory.
ANKTIVA + any future approved BCG strain: the same patent estate applies.
So it doesn't lock anyone out. Merck keeps making TICE BCG; what the IBRX patents lock in is the IL-15 + BCG combination across whatever strain is flowing through it.
Source: ImmunityBio IR PR, May 18 2026. Five issued US patents (Nos. 11,173,191; 11,679,144; 11,890,323; 12,268,731; 12,318,432), terms through at least 2035.
$IBRX Imagine you love someone with high-grade papillary bladder cancer that came back after BCG. They were told the next step was to take out the bladder. They went looking for anything else they could try. Last week they came across a drug, ANKTIVA, that the FDA approved in 2024 for the closely related form of the same disease, but not yet for theirs. They asked their urologist whether it could be used. The urologist said they were waiting to see what the FDA was going to do.
This Tuesday, the FDA answered.
WHAT THE LETTER SAID
On May 19, 2026, the FDA accepted ImmunityBio's supplemental Biologics License Application for ANKTIVA in combination with BCG, for BCG-unresponsive high-grade papillary-only non-muscle-invasive bladder cancer.
The action date the FDA committed to, the day by which it will issue its final decision, is January 6, 2027.
THE SIXTY DAYS THAT BECAME SEVENTY-ONE
The same application was turned away last year. The FDA refused to file it.
The company met with the FDA in January 2026 and was told what additional information was needed. No new clinical trials. A written submission detailing the overlapping features of papillary disease and CIS. The company submitted it. On March 9, 2026 the FDA acknowledged receipt, and the formal sixty-day filing-review clock started.
Sixty days from March 9 is May 8.
May 8 came and went. So did May 9, 10, 11, 12, 13, 14, 15.
On Saturday, May 16, at the American Urological Association Annual Meeting, the company's founder stood on a stage and said, into a microphone: "The 60 days have passed. We've not heard anything from the FDA. We're awaiting some response. I'm hopeful."
Three days later, on Tuesday, the response came.
Seventy-one days from receipt. Eleven days past the formal window. And then accepted.
ACCEPTED IS NOT APPROVED
Accepted means the FDA looked at the resubmitted application, decided it was complete enough to review on the merits, and started the formal clock. The decision comes in January 2027.
Between now and then the FDA reviews the application, may ask further questions, may convene advisory panels, may extend its own timeline. None of that has happened yet. This week, only one thing happened. The door opened.
But the door opening matters.
THE PAPER ANYONE CAN READ
The trial behind this application is QUILT-3.032 (NCT03022825). Its papillary-only cohort, Cohort B, was published in the Journal of Urology in January 2026, peer-reviewed and Open Access. The lead author is Sam S. Chang at Vanderbilt.
That is unusual for a binary regulatory event. Most of the time, the data on the FDA's desk is summarized through press releases and conference slides while the peer-reviewed publication lags by months or years. Here, the peer-reviewed publication landed first. The FDA is reading the same paper a patient's spouse can read tonight.
The link: https://t.co/E6Fma7y4Fu.
From the paper, with a data cutoff of July 15, 2024:
- Disease-free survival at 12 months: 58.2% (95% CI 46.6, 68.2)
- DFS at 24 months: 52.1% (CI 40.3, 62.7)
- DFS at 36 months: 38.2% (CI 25.6, 50.6)
- Progression-free survival at 12 months: 94.9% (CI 86.9, 98.0)
- PFS at 36 months: 83.1% (CI 69.5, 91.0)
- Disease-specific survival at 12 months: 98.7% (CI 91.4, 99.8)
- DSS at 36 months: 96.0% (CI 88.2, 98.7); median not reached
- Cystectomy avoidance at 12 months: 92.2% (CI 83.4, 96.4)
- Cystectomy avoidance at 36 months: 81.8% (CI 68.1, 90.1); median time to cystectomy not reached
- Treatment-related adverse events: 61% Grade 1 to 2; 3% Grade 3; no Grade 4 or 5
In plain English. Disease-free survival measures whether the cancer comes back at all, including in non-aggressive forms. About six in ten patients had no return of any kind at one year. By three years that has fallen to roughly four in ten, which sounds modest. The next three lines are the ones that change a patient's life.
Progression-free survival measures whether the cancer becomes muscle-invasive, the stage at which the bladder has to be removed or the disease becomes lethal. At one year, nineteen out of twenty patients had kept the cancer in the bladder lining, where it was still treatable. At three years, that was true for more than four out of five.
Disease-specific survival measures whether the bladder cancer kills you. At three years, ninety-six out of a hundred patients were still alive from this disease. The median, the point at which half the patients have died, has not been reached. The statisticians cannot yet draw the line.
And cystectomy avoidance, the line that means the patient still has a bladder: more than four out of five at three years. The median time to cystectomy, the point at which half had needed the operation, has not been reached either. They still have their bladders.
These are not press-release marketing numbers. They are the numbers in a peer-reviewed paper, downloadable as a PDF, sitting under a DOI.
The patients were told to lose their bladders.
Most still have them.
WHAT THE FDA WROTE ABOUT THE REVIEW
The FDA did not just accept the application. The acceptance letter, summarized in the company's press release on Tuesday, said two things.
The first set the review focus. The company quoted the FDA verbatim:
"The scientific data detailing these overlapping features will be the focus of the review of this sBLA to determine if there is adequate justification to allow for such an extrapolation and expansion of the indication of Anktiva with BCG to include the treatment of patients with BCG-unresponsive NMIBC with papillary tumors."
The FDA committed to spend the months between now and January 6 on the exact question the workshop spent Monday answering.
The second the company described in its own narrative prose, attached to the first by the word "while." Per the press release, the FDA reiterated its concerns relating to single-arm trials in papillary disease alone (Cohort B), given that the initial indication for CIS and papillary disease (Cohort A) has already been approved on a single-arm trial.
That second statement, even in the company's paraphrase, is the most interesting thing about the letter.
The concern, as reported, is that Cohort B was a single-arm trial. Patients received ANKTIVA plus BCG; their outcomes are reported; there is no randomized control arm receiving a different therapy for comparison. The FDA has historically preferred randomized controlled trials.
But the FDA approved Cohort A, CIS with or without papillary disease, from the same QUILT-3.032 trial, on the basis of a single-arm result in April 2024.
The exact methodology the FDA is reported to be reiterating concerns about is the methodology the FDA itself accepted as adequate two years ago, for the closely adjacent indication, in this same disease.
The review will turn on whether what was acceptable for one face of the disease is acceptable for the other.
WHAT THE FDA HAS ALREADY APPROVED
The FDA has approved five drugs for BCG-unresponsive non-muscle-invasive bladder cancer in the last twenty-seven years. All five were approved on single-arm trials.
- Valrubicin, 1998. Single-arm Phase 2 in 90 patients.
- Pembrolizumab, January 2020. KEYNOTE-057, single-arm Phase 2 in 96 evaluable patients. The advisory committee voted nine to four in favor.
- Nadofaragene firadenovec, December 2022. Single-arm in 98 evaluable patients.
- ANKTIVA's Cohort A, April 2024. The same QUILT-3.032 single-arm design, 77 patients.
- TAR-200, 2025. SunRISe-1 Cohort 2, single-arm Phase 2b in 85 patients.
In 2018, the FDA published its own guidance on developing drugs for BCG-unresponsive NMIBC. The guidance states, in writing, that a single-arm trial design is appropriate in this disease for patients with no standard therapy other than cystectomy. The FDA wrote the rule. The FDA then approved five drugs under it.
There is precedent outside this disease as well. In May 2017, the FDA granted the first-ever tissue-agnostic cancer approval to Merck's Keytruda (pembrolizumab) on the basis of 149 patients across five single-arm trials covering fifteen tumor types.
ANKTIVA's Cohort B sBLA uses the same single-arm methodology, in a population the FDA's own letter describes as having overlapping clinical and non-clinical profile with the indication already approved. Eighty patients. Three years of published peer-reviewed follow-up.
WHAT HAPPENED MONDAY
The day before the acceptance, on Monday May 18, the FDA's Oncology Center of Excellence convened a public workshop on non-muscle-invasive bladder cancer.
The first panel asked, on the record, whether CIS and papillary disease are the same disease.
The panel concluded they probably are. Different anatomical presentations of one biological process. A urologist on the panel testified that about one in twenty US urologists routinely use blue-light cystoscopy, which means CIS is missed at the initial diagnosis in most cases when it is there. Several panelists testified that when they treat high-grade papillary disease, they treat it the same way regardless of whether CIS is found alongside it. Because the FDA has not yet approved any therapy specifically for papillary-only BCG-unresponsive disease, urologists routinely use therapies labeled for CIS off-label in this setting, because what else is there.
ImmunityBio's own acceptance press release the next day restated the workshop conclusion in nearly the same language: that CIS and papillary disease "arise from the same cancer inducing clone, is therefore the same disease." The company's submission, the panelists' testimony, and the FDA's filing letter about "overlapping features" of the two presentations all converge on the same sentence.
That is the answer to the exact question the FDA's review will turn on.
It was on the record at the FDA the day before the FDA accepted the file.
The workshop happened on Monday.
The letter went out on Tuesday.
The timing is not a coincidence and was never supposed to be.
WHAT WAS ALREADY IN PLACE
While the application sat at the FDA, several other pieces had been locking into place around it.
The National Comprehensive Cancer Network added ANKTIVA plus BCG for BCG-unresponsive papillary-only NMIBC to its bladder cancer Clinical Practice Guideline as a Category 2A recommendation in March 2026. The NCCN's Drugs and Biologics Compendium, the publication that the Centers for Medicare and Medicaid Services consults under §1861(t)(2)(B)(ii)(I) of the Social Security Act, tracks the Guideline. The statutory pathway to Medicare coverage for off-label use was already open before the FDA accepted the file.
The United Kingdom's Medicines and Healthcare products Regulatory Agency approved ANKTIVA plus BCG for BCG-unresponsive CIS in July 2025. The European Medicines Agency followed in February 2026. International regulators had already decided the data was strong enough for the closely related indication.
On Monday, the day of the workshop, ImmunityBio also disclosed a US patent estate of five issued and one pending patent, with coverage extending through 2035, written to apply to any FDA-approved BCG strain rather than to a single supplier. The same day, a separate SEC 8-K disclosed an exclusive ten-year US supply agreement for the Japanese BCG-Tokyo-172 strain, structured with no payment due to the supplier until FDA approval of the combination. The US BCG supply has been served by a single FDA-approved strain, rationed since 2019; adding a second strain matters.
None of those pieces are the trial data. None of them substitute for FDA approval. But all of them are the pieces you would put in place if you were preparing for the moment a regulator opened the door.
WHAT JANUARY 6 MEANS
It does not mean approval. It means the day by which the FDA has committed to issue its decision, and the decision can be one of several: approve, approve with restrictions, issue a Complete Response Letter requiring further work, extend the timeline. The decision lands on or before that day.
It also does not mean a fast decision. From the FDA's receipt of the application on March 9 to the action date on January 6 is about ten months, the Standard Review goal for an efficacy supplement. Priority Review would have been six. The FDA, by the calendar, did not expedite.
For the patient whose spouse read about ANKTIVA last week, whose disease is high-grade papillary-only and whose next medical step is removal of the bladder, January 6 is not the end of the wait. It is the new shape of the wait. There is now a calendar date, set by the FDA itself, by which the FDA has committed to answer.
There was no such date on Monday.
There is one now.
THE LETTER
The letter came on Tuesday.
The patients in the paper were told to lose their bladders. Most still have them.
January 6 is the day the FDA decides who else gets to keep theirs.
@DrPatrick Thank you, @DrPatrick . The aim was only to make the science legible to the people it is actually about. Good done for others has a way of being seen - and of coming back. We will keep doing exactly that, for the patients.
A man walks out of his oncologist's office with a normal-looking blood test. Hemoglobin: fine. Neutrophils: fine. There is a third line on that same sheet almost nobody reads back to him. It is the one that tracks whether he lives.
On Saturday, in a room of urologists at the AUA annual meeting, @DrPatrick stood up and explained why that line goes untreated. Then he kept going - announcement after announcement, on a stage, on the record. Here is what he said.
THE THIRD LINE
On the AUA stage Saturday, Soon-Shiong said: "We've addressed anemia, we've addressed neutropenia, we've never addressed lymphopenia. And ironically... chemo and radiation causes lymphopenia. Now you begin to see the frustration and the madness of what we are doing."
That is the whole thesis in three sentences. Every routine blood test counts three things chemo and radiation knock down: red cells, infection-fighting neutrophils, and lymphocytes - the T cells and NK cells that kill cancer. Medicine built a drug to rebuild the red cells. A drug to rebuild the neutrophils. For the third - the cancer-killing one - nothing. The drugs given so patients can tolerate more chemo never touched the cell line chemo itself depletes.
How much does that third line matter? Not a company number - a 31,178-person US population study (Zidar et al., JAMA Network Open, 2019):
- Severe lymphopenia, all-cause death: about 1.8x the risk (age- and sex-adjusted).
- Cause-specific at severe lymphopenia: roughly 3x death from cancer, 4x from cardiovascular disease, 7x from infection and pneumonia.
In plain English: a $10 line on a standard blood count, that almost no oncologist treats, sorts who lives from who dies - across cancer, the heart, and infection at once. From the stage Soon-Shiong put it harder than the paper does ("if your ALC is below 2,000, your chances of dying early from all cause is 200 to 300%") - that is his framing; the published, adjusted figures are the ones above. They are damning without rounding up.
JUST A NUMBER
And here is what he says the agency said back. By his account, at a regulatory meeting with the FDA, the response to all of this was that the absolute lymphocyte count "is just a number." His reply from the podium: "PO2 is just a number - do you need oxygen? Hemoglobin A1C is just a number. Blood sugar is just a number." The same line a 31,178-person study ties to dying early at up to seven times the rate, waved off as not worth treating.
And look at which of those figures is largest. Not cancer. Infection. That is why Soon-Shiong does not present this as only a cancer drug - he extended the same logic to sepsis and infectious disease: one collapsed immune line, several different ways to die.
WHY IT EVEN WORKS
This is the part that makes the rest click, and it is textbook immunology, not a company theory. Tumors hide from the immune system's T cells by deleting a surface ID tag called MHC-I. That is why checkpoint drugs like Keytruda eventually fail: they rev up T cells, but a tumor wearing no tag is invisible to T cells no matter how revved. Loss of that tag is a documented mechanism of checkpoint-inhibitor resistance.
Now the elegant part, known to immunology for thirty years. NK cells run the opposite logic. A normal cell shows the tag and the NK cell passes it by. A cell that has dropped the tag screams "missing self" - and the NK cell destroys it. The tumor's single best trick against T cells is the exact signal that turns NK cells loose.
In plain English: every cell wears one ID badge. The T cell is a guard who can only grab a troublemaker he matches to his list, and the only way he checks is by reading that badge. A cancer cell that rips its badge off goes invisible to him. No badge, nothing to read, nothing he can do. Giving that guard more muscle (checkpoint drugs like Keytruda) changes nothing, because there is still no badge to read. The NK cell is the opposite kind of guard, with one rule: no badge, you are out. So the cancer's smartest escape from the first guard is the exact thing the second guard exists to catch.
ANKTIVA is the growth factor for those NK cells and T cells. It comes through the door the tumor opens when it slams the other shut. That mechanism is written into the federal label - section 12.1 states it is an IL-15 receptor agonist that stimulates CD8+ and CD4+ T cells and NK cells without expanding the regulatory T cells that would otherwise blunt the response. Soon-Shiong told the room he worked "desperately hard" to get that sentence into the label and is "not aware of any medicine in the history of medicine" carrying it. The cell line the death-predicting blood test measures is the cell line the label says the drug rebuilds.
THE FIRST PROOF IT MOVES THE LINE
For the first time, on that stage, he showed a randomized comparison from a lung-cancer trial: ANKTIVA plus Keytruda against Keytruda alone, with the same starting lymphocyte count. Over 27 weeks the ANKTIVA arm's count rose and held while the control arm's drifted down (P=0.0065). In the subgroup with the highest level of a key tumor marker, the ANKTIVA patients also went longer before their cancer progressed - a median of 7.0 months versus 2.2 (hazard ratio 0.40). It is his data, shown for the first time and not yet peer-reviewed - but it is the first randomized human signal that the drug raises the exact line that predicts who lives, and that raising it tracks with the patient doing better. (In a separate, earlier lung study he showed the patients whose count recovered lived a median 17.4 months versus 11.8 for those whose did not - he flagged that one himself as a correlation, not a randomized proof. The honest weight is on the randomized result above.)
In plain English: imagine a patient, Tom, with advanced lung cancer. Tom and a matched group all start the standard immunotherapy, Keytruda, with their cancer-killing lymphocyte count at the same level. Half of them, Tom included, also get ANKTIVA. Over the next six months Tom's group sees that count climb and hold; the Keytruda-only group watches theirs sag - and that split was not chance (the odds of a fluke were well under one in a hundred). Among the patients whose tumors carried the most of the marker immunotherapy keys off, Tom's group went about three times longer before the cancer started growing again, roughly seven months instead of two. It is a first look at his own data, not yet peer-reviewed. But it is the first time, with the comparison built in, that the drug has been shown to lift the very line that tracks who survives - and for that lift to move with the patient doing better.
THE DOCUMENT, AGAIN
So the drug raises the line, and raising the line tracks with living longer. The question that should follow - then why is it not everywhere? - has an answer, and it does not start with the drug. It starts in 2007.
In 2007 the US government answered a question oncology rarely asks out loud: of every immune molecule known, which has the best shot at curing cancer? The National Cancer Institute polled the field - NIH, the FDA, the major cancer societies. Out of more than a hundred, one came first: in Soon-Shiong's words from the AUA podium Saturday, "the number one that could address cancer is IL-15." ANKTIVA is built on it.
Then he added the part that should stop you. He had discussed that government ranking on the Sean Spicer show, and, he said, "I got a warning later about talking about a nice NCI document."
Sit with that.
Nearly two decades after the FDA sat among the bodies that ranked this molecule number one, the agency sent the man building it a warning letter for citing that ranking on air.
The ranking went to print in 2008 under a title the agency cannot take back: Mac Cheever, Immunological Reviews, "Twelve immunotherapy drugs that could cure cancers." IL-15 at the top. He didn't write that list. The government did, and the FDA was in the room.
On that same list, checkpoint inhibitors ranked second. The industry poured itself into number two - by his account more than forty approvals across tumor types, many of them won on the kind of single-arm trial we are about to come back to. Number one waited twenty years for someone to build it.
THE RULE THEY SAID DIDN'T BEND
Still in the same talk: "When the previous heads of the FDA, Dr. Prasad and Dr. Makary said... no trial has ever been approved for single arm, that's not true... Merck got it approved for single arm trial for 149 patients for all tumor types."
He is right, and this one is fully checkable. On May 23, 2017 the FDA gave Keytruda the first-ever tissue-agnostic cancer approval on 149 patients across five single-arm trials. The standard the prior CBER leadership held ANKTIVA to is one the agency itself waived for the market leader, on 149 single-arm patients. We built the file on that asymmetry; he said it to a room of urologists.
Stay on that for a second.
The two people who pressed that standard ran US drug approval. Dr. Vinay Prasad was Director of CBER, the FDA center that regulates biologics, which is to say the center that regulates ANKTIVA. Dr. Marty Makary was the FDA Commissioner.
What they said was untrue was not some obscure footnote. It was their own agency's most famous modern cancer approval. How do the two officials gatekeeping this drug get the single most checkable fact in their own building wrong, and then invoke it as the reason to make the drug wait?
And by the time Soon-Shiong called them "the previous heads" on Saturday, both were already gone. Prasad left the FDA at the end of April. Makary resigned on May 12, four days before the talk, and the day before he was scheduled to testify before a Senate subcommittee. The men who set the standard against this drug were out the door while the FDA's own record kept disproving it.
And it is not only that 2017 record. By his account on that stage, the same FDA has already granted ANKTIVA Expanded Access for any patient who has failed chemotherapy, radiation, and a checkpoint inhibitor, across cancers. Expanded Access is not a verdict on whether a drug works; it is the agency judging it safe enough to give patients with nothing left to try. So the FDA has opened a broad door to this drug for those patients, while the narrow approval that would let earlier ones through still sits unanswered. His objection to that sequence was the obvious one: why force a patient to fail everything else before being allowed this at all? That is his account from the stage, not an FDA letter we have read.
THE SECOND SOURCE
ANKTIVA is only approved given together with BCG. No BCG, no ANKTIVA - that is the label, not a preference. And BCG in the US has been a one-company, one-strain shortage for over a decade. We walked through that history yesterday.
So on Saturday he announced he had locked exclusive US rights to a second strain, Tokyo-172. The obvious doubt writes itself: a company secures its own backup and naturally swears it works. Here is why that doubt does not hold. He did not run the trial that proves it. The US government did - SWOG, the NCI-funded cooperative group, in a nine-year randomized head-to-head (Svatek et al., 2026): Tokyo-172 against the only US-approved strain. Result: non-inferior.
The part his own slide left out, kept here: that result held for the standard way of giving it; a second dosing schedule in the same trial did not work; and serious side effects ran somewhat higher with Tokyo-172. A proven equal, not a gentler one - and the government, not the company, paid for the proof.
Which is why his one blunt line on stage matters: "our approval just says any BCG. It doesn't say TICE." Hear what he is signalling. ANKTIVA's label never named Merck's strain, and the government's own nine-year trial just proved a second strain works. Tokyo-172 still needs the FDA to clear it. And Seth Lerner, the SWOG genitourinary chair he credited for that trial, is on the program at this week's FDA workshop: the proof is already in the FDA's own room, and so is the man who oversaw it.
WHAT THE SECOND SOURCE WAS REALLY FOR
The supply is not the prize. It is the runway for the prize. ANKTIVA today is approved only for patients whose cancer already came back after BCG - a fraction of the disease. BCG is given far earlier, first-line, to almost everyone who gets it. That first-line population is several times larger than the one the drug reaches today. By his account: the first-line trial, QUILT-2.005, finished enrolling in February, an independent committee reviewed it and said it had seen enough, and the application is ready to file. He says it; the FDA has not confirmed it. But the sequence is deliberate - lock a proven, government-validated BCG supply first, then file the first-line regimen that cannot exist without it, for a population many times the size of the one ANKTIVA serves now.
THE QUESTION THAT IS GENUINELY OPEN
Bladder cancer shows up in two shapes. Flat patches in the bladder lining, which doctors call carcinoma in situ, or CIS. And little finger-like growths, called papillary. ANKTIVA is already approved when CIS is present. The application that has been stuck is the one for the papillary-only form. So everything hangs on a single question: are these two shapes the same disease, or two different ones?
Soon-Shiong argues they are one - a single rogue cell line that just grows in two patterns. The science is genuinely split: some genetic studies show a shared origin; others find real molecular differences. It is honestly unsettled. That is not a footnote - it is the whole ballgame for the stuck application. And it is one of exactly two items on the agenda of the FDA's public workshop this Monday. The other item is the BCG shortage and what it does to clinical-trial design - the fight running through the rest of this post. The FDA did not convene a meeting on a side issue. It put on its agenda the two questions this drug's future turns on.
A BUREAUCRATIC RUT
And while that question waits on a workshop, the FDA's answer for the stuck application, by his account, is a randomized trial against chemotherapy.
Sit with what that asks.
Chemotherapy is the thing that causes lymphopenia - the collapsed third line a 31,178-person study ties to dying early. The comparator the agency wants is itself a driver of the harm. The problem he raised was ethical, not regulatory: how do you look a patient in the eye and randomize them into the chemotherapy arm - chemotherapy the FDA itself approved this past September, with serious adverse reactions in roughly a quarter of patients on its label - when chemotherapy is the very thing that collapses the cells keeping them alive? He said he would still run the trial. He also said he did not know how he could ethically recruit for it. He had a phrase for the loop: "a bureaucratic rut," he said. "It's not biology."
He spelled it out himself: the workshop asks "exactly the question we posed to the FDA group that's reviewing our BLA six months ago."
Sit with the timing.
Two days before the FDA sits down to decide whether CIS and papillary are one disease, the man whose stuck application hangs on that answer made the case for it - in public, to a room of the urologists who treat the disease. We called this pre-positioning before he said so. Then he said so.
THE BODY THAT ALREADY SAID YES
Here is what makes the wait extraordinary. While that question sits "open" at the FDA, it is not open at the body that writes the treatment guidelines American oncologists actually follow. This past March the NCCN added ANKTIVA plus BCG for BCG-unresponsive papillary-only disease - the exact stuck indication - as a Category 2A recommendation.
That is not a company press release.
By federal statute, Social Security Act section 1861(t)(2), a Category 1 or 2A listing in NCCN's drug compendium is a medically-accepted indication for Medicare coverage. In plain terms: the federal payer's own statutory test for what counts as covered cancer care is already met - while the FDA approval it would normally follow is not. Soon-Shiong's stage framing for it - "unanimous," "30 independent comprehensive cancer center directors," "bigger than an ODAC" - is his characterization; the guideline change and the statute are not.
THE MISSING LINK
One thing he could not announce that day: "The 60 days have passed. We've not heard anything from the FDA. We're awaiting some response. I'm hopeful."
That is the honest center of an enormous day. The first randomized proof the drug raises the line. The first-line filing ready to go. A government-validated second BCG supply locked. Saudi Arabia already approving it for lung cancer the US has not. Everything moving - except the one application that would let the next patient actually reach it. On one clinic's list, by his count, fifteen thousand of them are waiting.
The story was never whether the science works. It was whether anyone would treat the line on the blood test that decides who lives, and whether the agency that ranked this molecule number one would let the patient have it.
A foreign regulator already crossed that line - by his account the Saudi FDA accepted the whole frame, that the root cause is the collapse of the immune system and the cancer is only its symptom.
On Saturday the man who built it answered the first question, on the record, in a room of the doctors who will use it. The second answer is still sitting on a desk at the FDA, sixty days unanswered - on the very day the agency finally sits down to debate the very questions it turns on.
He gave Saturday its own name: "maybe we've actually closed the missing link." Everything in this post says he did. The last word on whether the patient ever gets it is not his.
A woman is told her bladder cancer has come back. Then she is told something stranger: there is a therapy the FDA approved for exactly this - and she still might not be able to get it.
Not because it failed her. Not because she can't afford it. Because it only works paired with a second drug, and that second drug has been in short supply in this country for more than a decade.
THE PROBLEM
First, what BCG is. It is the standard treatment for early bladder cancer, and has been for roughly fifty years. It is not a chemical drug. It is a live, weakened bacterium - the same one first used as the tuberculosis vaccine - put directly into the bladder to wake the immune system up against the cancer. Bladder cancer was treated with immunotherapy decades before the word was fashionable. It works. The hard part has always been getting it.
ANKTIVA is FDA-approved for bladder cancer that comes back despite BCG. The label does not say "ANKTIVA." It says ANKTIVA in combination with BCG.
So the rescue therapy for a patient whose cancer survived BCG needs more BCG.
And BCG in the United States has had one FDA-approved supplier - Merck - and one strain, in shortage since 2012, more than a decade, and allocated by Merck for years. Doctors splitting doses. Delaying patients. Turning people away.
An approved drug whose approved regimen could not always be filled. That is the problem nobody was solving.
WHAT HAPPENED SATURDAY
On Saturday, May 16, on stage at the American Urological Association annual meeting, ImmunityBio announced it had secured exclusive U.S. rights to a second source of BCG - the Tokyo-172 strain. ImmunityBio, not the manufacturer in Japan, would be the one to take it to the FDA.
Not a promise. A signed agreement, with the head-to-head trial already done.
THE DATA
The proof is SWOG S1602: a randomized Phase 3 trial run by the National Cancer Institute through a federally funded cooperative group, in patients getting BCG for the first time - the standard first-line setting. It put the Tokyo-172 strain head to head against the only BCG the FDA has approved. Presented by Svatek and colleagues at the ASCO genitourinary symposium, 2026.
The results:
- High-grade recurrence-free survival: Tokyo-172 non-inferior to the standard strain. Pre-specified non-inferiority bar met.
- 5-year high-grade recurrence-free survival: 64 percent (Tokyo-172) vs 58 percent (standard).
- This held for the straight intravesical schedule. A separate priming schedule in the same trial did not.
- Serious (grade 3-4) side effects: higher with Tokyo-172 than the standard strain.
In plain English:
"Non-inferior" means the new BCG was statistically shown to be not worse than the old one at keeping high-grade cancer from coming back. The trial set a bar in advance for how much worse it could be and still count as equivalent; Tokyo-172 stayed inside that bar. This is the result that matters for a shortage: a second source proven non-inferior in a government-run trial - not a marginally better drug.
Five years out, 64 of every 100 patients on Tokyo-172 had no high-grade recurrence, versus 58 of every 100 on the standard strain. Directionally favorable, but the trial's claim - and the honest claim - is equivalence, not superiority.
Two caveats that belong in the open: only the standard intravesical way of giving it worked; a different dosing schedule tested in the same trial failed. And serious side effects were more common with Tokyo-172. This is "as effective, by the government's own randomized data" - not "gentler."
THE PATH
Who does what, and exactly where this stands.
Done:
- The trial. SWOG S1602 was designed, run and analyzed by the National Cancer Institute and the SWOG cooperative group - publicly funded, independent of the company. It showed Tokyo-172 non-inferior to the approved strain.
- The supply. Japan BCG Laboratory, which has made this strain for decades, signed an exclusive U.S. development and supply agreement with ImmunityBio on May 16, 2026.
- The rights. ImmunityBio - not the Japanese manufacturer - is the sole U.S. applicant. ImmunityBio is the one that will file with the FDA and would hold the U.S. license.
Not yet:
- The data agreement. To use the SWOG S1602 results in a filing, ImmunityBio is still negotiating a Data Use Agreement with SWOG, the NCI and Fred Hutchinson. In discussion. Not signed.
- The FDA conversation. Engagement with the FDA on the approval path is, in the company's own words, still "to be initiated."
- The filing. The Biologics License Application is planned. It has not been filed.
- The decision. No FDA review. No approval. No date - the company has given no timeline.
- The patient. Until all of that, a U.S. patient still cannot get Tokyo-172.
What changed on Saturday is not availability. It is that the road now exists - and it runs on data the government already paid for.
WHO WAS WAITING ON WHOM
The data that underwrites this was generated by the National Cancer Institute. Federal money. A public trial. Sitting in the public domain.
Two days after the Saturday announcement - Monday, May 18 - the FDA's own Oncology Center of Excellence holds a public workshop on contemporary issues in non-muscle invasive bladder cancer. The BCG shortage and what it does to clinical trials is on the agenda. The exact problem.
The company is not on that agenda. It does not speak there. It does not need to. It had addressed the regulator's own stated problem two days before the regulator's independent panel sat down to discuss it - using a randomized trial the government itself paid for and ran. Days earlier, in public, the founder had already named the frame: "S1602 is the kind of rigorous, publicly funded science that should inform FDA decision-making."
ANNOUNCED, NOT HEARD
There was a press release. There was a post from @DrPatrick. None of it was hidden. It still didn't land - because supply agreements are not supposed to be dramatic, a licensing deal does not trend, and it crossed the wire on a Saturday as a few words about "exclusive U.S. supply." Most people filed it under logistics and scrolled on.
Here is what they scrolled past: a company whose only approved drug legally requires a partner product it never controlled - BCG, rationed by Merck, which competes in the same disease with its own drug - just took exclusive U.S. rights to a second, trial-proven source of it.
WHAT THIS WAS REALLY FOR
The supply story is not even the real story. The woman in this post is in the smaller group: patients whose cancer already came back after BCG. But BCG is given far earlier - it is the standard first treatment for the disease. That first-line group is several times larger than the one the approved drug covers today.
That is exactly where ImmunityBio's next bladder-cancer application is aimed: its first-line trial, QUILT-2.005, behind a BCG-naive filing the company has guided for the end of 2026 - a far larger patient population than the approved use it sells now.
That filing is also a BCG regimen. The company could not deliver it at scale without a BCG supply it controls.
So the order matters. Secure a proven BCG first - validated by the government, in exactly that first-line population - then file. The supply deal was not the headline. It was the precondition for the one still to come.
THE MISSING HALF
For two years, the question about this therapy was never whether it works. It was whether the patient could ever get all of it.
That question used to have no good answer. A single supplier. A decade of shortage. Nothing a company could do about the half it didn't own.
It owns it now. The proof is done and public. The approval is not.
For the first time, what stands between the patient and a complete, approved therapy is a regulatory path - not a shortage.
$IBRX In an ICU somewhere in America tonight, a 65-year-old former electrician is on day four of sepsis. Call him Frank.
Frank came in with pneumonia that turned septic. The antibiotics worked. His blood pressure stabilized. He came off vasopressors. The acute crisis appears to be over.
His absolute lymphocyte count is 600 cells per microliter.
The infection his immune system was fighting is now technically controlled. His immune system is not. His doctors describe him as "still fighting." What they mean is that the second phase of sepsis has begun and there is no specific drug for it.
About 7 patients out of every 10 who die of sepsis die in this phase.
THE NUMBERS
Sepsis is the most common cause of hospital death in the United States. The Centers for Disease Control and Prevention estimates at least 1.7 million American adults are hospitalized with sepsis each year, and at least 350,000 die from it.
That is more deaths per year than colorectal cancer and pancreatic cancer combined.
Standard of care has not fundamentally changed in twenty years. Antibiotics. Intravenous fluids. Vasopressors. Mechanical ventilation when needed. The first phase of sepsis - the hyperinflammatory phase, where the immune system overreacts and damages organs - is what hospital protocols are built to control.
The second phase is not.
THE TWO PHASES
Sepsis is a biphasic immune disease. This is established in the medical literature.
The first phase is overreaction. The body responds to infection with such force that it damages its own tissues. This is the phase that produces the classic septic shock picture: fever, low blood pressure, organ failure. Modern critical-care medicine has gotten good at managing this phase.
The second phase is collapse. After the immune storm, the body shuts immune cells down. Lymphocytes die by apoptosis. Both arms of adaptive immunity collapse. Patients who survived the first phase are now defenseless against the next infection their body picks up in the ICU.
That second phase is when most of the dying happens.
THE 70 PERCENT
A 2014 study published in the journal Shock followed 335 adult patients with sepsis at a single academic center. Drewry and colleagues looked at the absolute lymphocyte count on day four after diagnosis and asked whether it predicted who would survive.
The results:
- Severe persistent lymphopenia (ALC ≤ 600 cells/uL on day 4): 39.5% died within 28 days
- Moderate lymphopenia: 24.6% died within 28 days
- Normal lymphocyte count: 10.4% died within 28 days
- 1-year mortality with severe persistent lymphopenia: 57.9%
- Only 30.3% of sepsis deaths occurred before day 4
In plain English:
The patients whose lymphocyte counts had collapsed by day four were almost four times more likely to die in the next 28 days than the patients whose lymphocyte counts held up. By one year out, more than half of the severely lymphopenic patients were dead.
And only about one in three sepsis deaths happened in the first four days. The other roughly seven in ten happened later, after the acute crisis appeared to be over.
The hyperinflammatory phase gets the headlines. The immunosuppressive phase gets the deaths.
THE DIAGNOSIS THAT EXISTED
The medical literature has named this problem for more than a decade. Hotchkiss and colleagues described sepsis-induced immunosuppression in Nature Reviews Immunology in 2013. Boomer demonstrated profound T-cell exhaustion in tissues from patients who died of sepsis. Subsequent reviews labeled the phenomenon "post-sepsis immune paralysis."
There has been an earlier attempt at a specific therapy. The IRIS-7 trial, published in JCI Insight in 2018, tested recombinant interleukin-7 (CYT107) in 27 patients with septic shock and severe lymphopenia. The result: a three- to four-fold increase in absolute lymphocyte counts, no cytokine storm, no worsening organ dysfunction. The trial was the first immunoadjuvant therapy ever tested in sepsis, and it worked at the level of restoring lymphocytes.
But IL-7 is not approved for any human indication. The IRIS-7 trial did not lead to a registered product.
The diagnosis existed. The proof-of-concept existed. The drug did not.
THE PROPOSAL THAT EXISTS
Yesterday a new clinical trial was posted to https://t.co/sq8TuetgBK.
NCT07578558. ResQ2204-SEPSIS. Sponsored by ImmunityBio. Phase 2, randomized, open-label. Fifty critically ill adults with sepsis and persistent lymphopenia, randomized 1:1 to nogapendekin alfa inbakicept plus standard of care, or standard of care alone.
The trial details:
- Phase: 2, randomized, open-label, parallel assignment, 1:1
- Enrollment: 50 participants (25 per arm)
- Population: ICU adults with sepsis per Sepsis-3 criteria AND ALC <1,000 cells/uL on two consecutive measurements within 72 hours
- Intervention: NAI 1.2 mg subcutaneously on Day 3 (or earlier if ALC <700), Day 14, optional Day 21
- Primary endpoint: 28-day all-cause mortality
- Secondary: ALC change, ICU re-admission, secondary infections, 90-day mortality, safety
- Sponsor: ImmunityBio, Inc.
- Study start: July 6, 2026
- Primary completion: August 3, 2027
First posted on https://t.co/sq8TuetgBK: May 11, 2026
In plain English:
ImmunityBio is testing whether the same molecule the FDA approved for bladder cancer in 2024 can keep septic patients with collapsed immune systems alive long enough to recover. The drug is the IL-15 superagonist sold as ANKTIVA. The mechanism rebuilds the natural-killer cells and memory CD8+ T cells that the second phase of sepsis destroys.
The trial is small: 50 patients. Sepsis mortality in this population runs roughly 40 percent at 28 days. If ANKTIVA cuts that materially, the effect will be visible. The point of a 50-patient trial in this setting is not to convince the FDA. It is to find out whether the molecule works in a non-cancer disease.
THE SECOND PILLAR
This is not a side bet. This is the cross-indication thesis.
The Q1 2026 quarterly report ImmunityBio filed with the SEC on May 7 formally defined the company's strategy as "first-in-class immunotherapy strategy designed to restore immune competence by reversing lymphopenia." That definition is not cancer-specific. It is mechanism-specific.
Lymphopenia is the substrate. Cancer is one disease in which lymphopenia kills patients. Sepsis is another.
@DrPatrick has been describing the strategy publicly for months as three pillars: cancer, longevity, sepsis. The framework was formally committed three months ago. On February 23, 2026, ImmunityBio's full-year 2025 earnings release included a section titled "3-Year Global Strategy: ANKTIVA as a Backbone to the Cancer BioShield Platform," explicitly naming six strategic areas: BCG-naïve bladder cancer, non-small-cell lung cancer, glioblastoma, sepsis, non-Hodgkin lymphoma, and treatment of lymphopenia. Yesterday's NCT07578558 is a new Phase 2 step inside that committed sepsis pillar.
THE SAME MOLECULE
The drug being tested in NCT07578558 is the same drug being given to bladder cancer patients in 60-plus US urology centers. The same drug Saudi Arabia approved for non-small-cell lung cancer in January 2026. The same drug the NCI selected for two cancer-prevention trials this week.
One molecule. One mechanism. Three disease pillars.
The Cancer BioShield framing was always the smaller half of the strategy. The bigger half is the immune-restoration thesis applied across every disease where lymphocyte collapse is the difference between living and dying.
THE STAKES
About 1.7 million American adults are hospitalized with sepsis every year. Roughly 350,000 die. If the Drewry data approximates the truth, somewhere around 245,000 of those deaths happen in the immunosuppressive phase that has no specific therapy.
The same week the NCI sponsored two cancer-prevention trials of ANKTIVA, ImmunityBio registered a Phase 2 trial asking whether the same molecule can address the leading cause of hospital death in the United States.
Frank is in an ICU somewhere tonight. His blood pressure has stabilized. His lymphocyte count has collapsed. The hospital protocol for his situation has not changed in twenty years.
A protocol that might change has just been posted to https://t.co/sq8TuetgBK.
BEYOND CANCER
NK cells were photographed in 1969. They were rejected as an artifact, then ranked first in 2007, then approved as ANKTIVA in 2024.
This week the NCI selected the same molecule for two cancer-prevention trials.
Yesterday ImmunityBio registered the trial that tests the same molecule against the second pillar.
A drug built to restore immune competence by reversing lymphopenia is not a cancer drug. It is a lymphopenia drug.
Cancer is the first indication.
Sepsis is the second.
Beyond cancer is where the strategy was always going.
$IBRX Somewhere in America this week, a 73-year-old retired teacher is being told she has metastatic non-small-cell lung cancer. Call her Maria.
The cancer is in her bones, her liver, possibly her brain. The doctor explains the standard sequence. Chemotherapy. Radiation. A checkpoint inhibitor. When that stops working, more chemotherapy.
Maria listens. She tells him she watched her sister go through chemo twenty years ago. She tells him she lives alone. She tells him she takes seven other medications for heart failure and diabetes.
The doctor closes the folder.
In 53 cases out of every 100 like Maria's, what happens next is nothing.
THE NUMBERS
A paper published in JAMA Oncology on May 7 looked at every American aged 65 or older diagnosed with metastatic non-small-cell lung cancer between 2006 and 2021. 254,611 people.
53.2 percent never received any systemic therapy. Not chemotherapy. Not immunotherapy. Not targeted therapy. Nothing.
39.8 percent were dead within 90 days of diagnosis. Of those, only 13.2 percent had received any treatment at all before they died.
The treated proportion barely increased between 2006 and 2021. Fifteen years of breakthrough cancer drug approvals. Half of older Americans diagnosed with metastatic NSCLC still get sent home with nothing.
The senior author, Gerard Silvestri at the Medical University of South Carolina, said: "Get patients to an oncologist - quickly - so that we can see if they're eligible for one of these new treatments."
The American Cancer Society projects more than 200,000 lung cancer diagnoses in the US in 2026. About half will be metastatic at diagnosis. Tens of thousands of those patients per year, on the patterns the JAMA Oncology paper describes, will receive nothing.
THE THREE BARRIERS
The paper names three reasons:
- Fear of chemotherapy based on its old reputation
- Lack of social support and transportation
- Treatment guidelines that exclude patients with comorbidities
Maria, a 73-year-old widow living alone with heart failure and diabetes, hits all three.
The guidelines say she is not eligible. So no one offers her a drug.
THE STANDARD OF CARE
This is what is offered to the 47 percent who do get treated, in order:
Chemotherapy. Radiation. A checkpoint inhibitor.
A checkpoint inhibitor (Keytruda, Opdivo, or Tecentriq) is a drug that releases the brake the cancer puts on the immune system. Roughly half of metastatic NSCLC patients respond at first. Most eventually progress as the cancer finds a way around the unblocked immune cells.
When that happens the patient is on what oncologists call third-line treatment. Historical median overall survival in that setting with standard-of-care chemotherapy is approximately 7 to 9 months.
Yesterday @DrPatrick wrote: "Chemo. Radiation then checkpoints, then even more chemo!! When do we learn that this can change with immunotherapy? What could we do for the thousands of patients who failed all of above?"
He has data on that question.
THE TRIAL
QUILT-3.055 (NCT03228667) was a Phase 2b trial of N-803, the IL-15 superagonist now sold as ANKTIVA, given together with the same checkpoint inhibitor each patient had already failed. 86 patients with advanced NSCLC, all previously progressed on Keytruda, Opdivo, or Tecentriq either alone or with chemotherapy.
The results:
- Median overall survival: 14.1 months (95% CI 11.7 to 17.4)
- 12-month survival: 57 percent
- 18-month survival: 34 percent
- Long-term survivors out past 58 months
- Less than 10 percent grade 3 or higher ANKTIVA-related adverse events. No cytokine release syndrome.
In plain English:
Half the patients lived more than 14.1 months from the start of treatment. Half lived less. The midpoint is what oncologists call median overall survival. The 95 percent confidence interval was 11.7 to 17.4 months, which means the trial's data anchors that midpoint with statistical reliability. The comparable population on standard-of-care chemotherapy has a median around 7 to 9 months.
More than half of the 86 patients were still alive at 12 months. About a third were still alive at 18 months. Some are still alive more than 58 months - nearly five years - after treatment began.
Fewer than 10 percent of the patients had a serious side effect attributed to ANKTIVA. No patient experienced cytokine release syndrome, the dangerous immune storm that has limited other IL-15-class therapies.
The mechanism: IL-15 expands NK cells, the innate immune front line, and memory CD8+ T cells, the adaptive surveillance arm. It does so without expanding the regulatory T cells that suppress responses. The checkpoint inhibitor that had stopped working starts working again because the immune system it depended on has been rebuilt.
The 10-Q filed on May 7 formally defined ImmunityBio's strategy as "first-in-class immunotherapy strategy designed to restore immune competence by reversing lymphopenia." That is Cancer BioShield.
IMAGINE EARLIER
QUILT-3.055 enrolled patients at the bottom of the treatment ladder. They had been through chemotherapy. Many through radiation. All of them had been through a checkpoint inhibitor, and that checkpoint inhibitor had stopped working. They were on second- or third-line treatment. Some had run out of options.
In that population - the one with the least to gain - adding ANKTIVA to a checkpoint inhibitor that had already failed produced median overall survival of 14.1 months and long-term survivors out past five years.
That is the floor.
Now picture the same drug in a patient whose cancer was caught earlier. Before the chemotherapy. Before the radiation. Before the immune system had been beaten down by years of treatment and tumor burden. The mechanism would have more ground to work on. The cancer would have fewer escape routes already in place.
The NCI is testing exactly this premise. The same institution that listed two ANKTIVA cancer-prevention trials last week is asking whether immune restoration can stop cancer before it crosses the line into refractory disease.
The QUILT-3.055 results were obtained in the population least likely to respond. The ceiling is unknown.
THE APPROVAL THAT EXISTS
In mid-January 2026, the Saudi Food and Drug Authority granted ANKTIVA accelerated approval for non-small-cell lung cancer.
On April 21, 2026, the drug launched commercially in Saudi Arabia. Two indications available within 60 days through distribution partners Biopharma (Dubai) and Cigalah Healthcare (Jeddah): bladder cancer and lung cancer.
A Saudi patient who has failed chemotherapy, radiation, and a checkpoint inhibitor has access to the drug Cancer BioShield was built around. An American patient in the same disease, in the same position, does not.
THE GAP
The FDA has been busy on ANKTIVA in the past year.
May 2025: a refusal-to-file from CBER on a papillary bladder cancer supplement.
March 13, 2026: an FDA Office of Prescription Drug Promotion warning letter citing nine violations in ANKTIVA promotional materials.
Three class-action lawsuits filed against the company in the months that followed.
Vinay Prasad was appointed CBER director in May 2025 by FDA Commissioner Marty Makary, his podcast friend and co-host. Prasad had spent nine years publicly attacking Patrick Soon-Shiong in print, on STAT News, and on the same podcast he co-hosted with Makary. Makary appointed Prasad to CBER six months after his most recent attacks. Prasad departed April 30, 2026. Makary is, per the Wall Street Journal, being fired.
The JAMA Oncology authors wrote: "Despite advances in therapy in recent decades, almost half of patients never received systemic therapy, and the proportion treated only minimally improved over time."
The advances arrived. The patients have not.
THE STAKES
Half of American adults aged 65 and older diagnosed with metastatic NSCLC will receive no treatment of any kind.
40 percent will be dead within 90 days of diagnosis.
The drug developed for the patients who failed every existing treatment doubled median survival in QUILT-3.055. It has fewer grade 3 adverse events than the chemotherapy the population fears. The Saudi FDA approved it four months ago.
No public communication has explained why a US lung cancer indication has not followed.
THE HALF THAT GOT NOTHING
Maria. The widower in Tampa. The grandfather in Detroit. They will be diagnosed this week. Half will be offered nothing.
The trial finished. The data was published. The drug exists. The approval came in a different country.
The half that got nothing are still waiting.
$IBRX Somewhere in a genetic counselor's office today, a 25-year-old is being told the result of her test.
She has Lynch syndrome.
Her lifetime risk of colorectal cancer is closer to 80% than 5%. Her risk of endometrial cancer is 40 to 60%. There are six other organs the same mutation will try to kill her in.
The counselor will tell her to schedule a colonoscopy every year for the rest of her life starting now. He will tell her about risk-reducing hysterectomy and oophorectomy starting around age 40. He will mention aspirin.
He will not tell her about a preventive drug.
Because there isn't one.
THE NUMBERS
Lynch syndrome is caused by germline mutations in DNA mismatch repair genes. The mutation is inherited. Every cell of every body part carries it.
About one in 279 Americans is a carrier. Roughly 1.2 million people. Most do not know.
Lifetime cancer risks for the carriers:
- Colorectal cancer: 50 to 80%
- Endometrial cancer in women: 40 to 60%
- Stomach, ovarian, hepatobiliary, urinary, small bowel, brain
- Average age at colorectal cancer diagnosis: 44
General population colorectal risk: 4 to 5%.
Standard of care is not prevention. It is surveillance. For the highest-risk genes (MLH1, MSH2), annual colonoscopy starting between ages 20 and 25. Find the cancer earlier than it would otherwise be found. Cut it out before it spreads.
The only preventive intervention with randomized-trial evidence is daily aspirin (CAPP2, Burn et al, Lancet, 2011). 600 mg per day for a mean of 25 months. Per-protocol hazard ratio of 0.41 for colorectal cancer. Real but modest. A single anti-inflammatory tablet, repurposed.
That is the field. Until this week.
THE BURIED LINE
ImmunityBio filed its Q1 2026 quarterly report with the SEC on May 7. Dozens of pages of pipeline disclosures, financial statements, legal proceedings.
In the middle of one MD&A pipeline list, one sentence appears:
"ANKTIVA has been selected by the NCI for evaluation in a cancer prevention study in patients with Lynch syndrome."
That is one line in a federal SEC filing.
THE NEXT DAY
On May 8, one day after the 10-Q was filed, a new entry was posted to https://t.co/j6TST0ZdM2.
Trial NCT07574541. Phase 2. Sponsor: National Cancer Institute. Setting: NIH Clinical Center, Bethesda. Population: men with low- and intermediate-risk prostate cancer on active surveillance.
The intervention: an NCI-developed three-antigen vaccine (PSA, MUC-1, brachyury) plus N-803. N-803 is the generic name for ANKTIVA.
The NCI is putting its OWN vaccine alongside ANKTIVA in men whose tumors haven't progressed to radical therapy yet. Running it at its OWN clinical center in Bethesda. With ITS OWN budget. ImmunityBio supplies the drug. The taxpayers pay for the test.
Primary endpoint: CD8+ and CD4+ T-cell density inside the tumor before and after treatment.
Two NCI-sponsored ANKTIVA trials in two days. Both about catching cancer earlier or stopping it from progressing.
That makes three NCI-sponsored programs total: the two new ones plus the rBCG Expanded Access Program disclosed in the company's most recent annual 10-K.
THE FIRST ACT, 1969
The institution behind both new trials is the National Cancer Institute. The same NCI.
In 1969, a Hungarian-born physician named Joseph Sinkovics, working at MD Anderson Hospital, drew his own blood. He isolated the lymphocytes. He watched them kill cultured cancer cells in a petri dish. He photographed it.
He sent the photos and the data to the NCI. They cancelled his grant. They called the killing "an in vitro artifact." They were wrong. The cells he had photographed were what would later be named natural killer cells, formally classified by Kiessling, Klein, and Wigzell in 1975.
The NCI in 1969 said: this is not real.
THE SECOND ACT, 2007
In 2007, the same NCI hosted a workshop on cancer immunotherapy agents. Co-sponsored with NIH, FDA, AACR, ASH. They reviewed 124 immunotherapy agents. They ranked them by potential to impact cancer mortality.
The molecule ranked #1 was interleukin-15. IL-15. The cytokine that activates the very NK cells the agency had rejected as artifacts thirty-eight years earlier.
The NCI in 2007 said: this is the most important cancer molecule we know of.
The grants did not follow. Seventeen more years passed.
THE THIRD ACT, 2026
In 2024, the FDA approved the first IL-15 superagonist for human use. ANKTIVA. The molecule that activates NK cells. The molecule the NCI had ranked first seventeen years earlier.
This week, the same NCI selected the same molecule for two trials in two days. Lynch syndrome on Thursday. Prostate active surveillance on Friday.
Not treatment of advanced disease in either case. The category is what's new: catch cancer before it forms, or before it converts from manageable to lethal.
The NCI in 2026 says: we want to test whether this molecule can keep cancer from progressing in the first place. And we want to test it in two diseases at once.
Same agency. Three acts. Fifty-seven years.
THE BIOLOGY
Why Lynch syndrome and prostate active surveillance, simultaneously?
Both populations have cells that are not yet cancer but are accumulating the errors of cancer. Lynch carriers cannot repair DNA mismatches; their premalignant cells display abnormal proteins for decades. Active-surveillance prostate patients have organ-confined low-grade tumors that may or may not progress over years.
In neither case is the question how to kill cancer. The question is how to keep abnormal cells from becoming cancer that has gone too far to control.
That is what IL-15 does. It expands NK cells, the innate first responders. It expands memory CD8+ T cells, the adaptive surveillance arm. It does so without expanding the regulatory T cells that would suppress the response.
Both arms of the immune system at higher activity, in populations whose cells are already trying to become cancer.
The hypothesis is interception. Catch the cells before they cross into cancer.
THE SHIFT
Cancer treatment has been the focus of nearly all immunotherapy development since checkpoint inhibitors arrived in 2011. The Cancer Moonshot, launched in 2016 and revived in 2022, was framed as a mortality-reduction effort.
Most of the actual funding went to treatment trials.
ANKTIVA in Lynch syndrome would be the first IL-15 superagonist tested in true cancer prevention. ANKTIVA in active-surveillance prostate cancer is the first IL-15 superagonist tested in early intervention, keeping low-grade disease from converting to surgery or radiation.
If either works, the category changes. The question becomes whether immune-restoration drugs deserve a place alongside vaccines in cancer prevention and alongside watchful waiting in early intervention.
THE STAKES
About 1.2 million Americans carry a Lynch syndrome mutation. Most do not know they carry it. Of those who do, the standard offering is annual colonoscopy, risk-reducing hysterectomy and oophorectomy around age 40, daily aspirin.
The American Cancer Society projects 333,830 American men will be diagnosed with prostate cancer in 2026. Hundreds of thousands are on active surveillance at any given time. Roughly 35% of those men progress to radical therapy (surgery or radiation) within five years because their tumor grows.
The 25-year-old in the genetic counselor's office today has nothing to take. The 65-year-old on prostate active surveillance today is told to wait and watch.
This week, the NCI placed its name on the trials that ask whether something different is possible. Twice.
THE INSTITUTION RETURNED
NK cells were photographed in 1969. The NCI called the killing an artifact.
IL-15 was ranked #1 of 124 immunotherapy agents by the NCI in 2007. The grants did not follow.
ANKTIVA was approved by the FDA in 2024.
This week the NCI put its name on two cancer-prevention-and-early-intervention trials of the molecule. One on a Thursday. One on a Friday.
In the prostate trial, the NCI is putting its own vaccine alongside the drug. Both trials are NCI-sponsored. The federal government is paying to find out whether the immune system can be taught to stop cancer before it starts.
Same institution. Three different decades. Fifty-seven years between drawing the blood and sponsoring the prevention.
The work did not move.
The institution did.
$IBRX Yesterday morning in Athens, @DrPatrick posted a selfie.
Acropolis in the background. Light blue shirt, blue tie. One sentence:
"In the land of Hippocrates the Father of Modern Medicine..do no harm."
Eleven hours later, the Wall Street Journal reported that President Trump was planning to fire FDA Commissioner Marty Makary.
The harm had already been done.
THE FRIEND
On May 6, 2025 - just over one year ago - Marty Makary appointed his longtime podcast friend Vinay Prasad to direct CBER, the FDA division that regulates ANKTIVA.
The friendship was documented across at least eighteen pre-FDA podcast episodes spanning 2019 to 2024. They were on each other's shows. They wrote together. They built audience together.
On May 6, 2025, the friendship became regulation.
THE NINE YEARS
Vinay Prasad has spent nine years publicly attacking Patrick Soon-Shiong.
In 2017, in a STAT News investigation, Prasad called Soon-Shiong's NK cell trial findings "miniscule and vague."
In 2021, in JAMA Oncology, Prasad co-authored a paper attacking the FDA's accelerated approval pathway for BCG-unresponsive bladder cancer - the same pathway ANKTIVA used three years later.
In October 2024, on YouTube, Prasad called Abraxane "a me too drug" and said of Soon-Shiong: "that's how he got his money."
In late October 2024, on the VPZD Show podcast, Prasad and his co-host called Soon-Shiong "a snake oil salesman."
In November 2024, six months before being named to replace him at CBER, Prasad attacked the outgoing CBER director Peter Marks in profanity-laden language on the Sensible Medicine podcast.
In December 2024, four months before his own appointment, Prasad publicly slipped: "Hopefully it gets fixed because my friend Marty Macri is gonna be the new commissioner. So that's good news for me. No, it's good news for Marty. It's good news for all of us."
The friendship was on tape. The hostility was on tape. Both went on tape together.
Marty Makary heard them. And then he hired Vinay Prasad.
THE FIRE AND THE REHIRE
In July 2025, two months into Prasad's CBER tenure, HHS fired him.
Weeks later, Marty Makary insisted he come back.
Prasad came back.
The man who had publicly called the founder of ANKTIVA a snake oil salesman, attacked the regulatory pathway that approved ANKTIVA, and counted on a friendship with the new FDA Commissioner for personal advantage was placed back in charge of regulating ANKTIVA, after his employer had already fired him once.
That is the harm.
THE COST
During Prasad's tenure under Makary's protection:
The papillary expansion sBLA was refused-to-file in May 2025.
The OPDP issued a warning letter to ImmunityBio in March 2026 over a television advertisement that never aired and a podcast interview.
Three lawsuits were filed against ImmunityBio in March and April 2026 referencing that warning letter, naming the company and Patrick Soon-Shiong personally as defendants.
The patients waiting for ANKTIVA in indications it has not yet been approved for, in the country where the drug was discovered and approved, did not get it.
In 34 other countries, they did.
THE FRAME
Marty Makary trained as a doctor. The founding ethic of his profession is two thousand four hundred years old: first, do no harm.
He hired the man who had spent years attacking the founder of the only FDA-approved IL-15 superagonist.
His employer fired the man two months later.
Marty Makary brought him back.
The full investigation, with every receipt, is here: https://t.co/2dlmQc7JaI
DO NO HARM
Yesterday morning, Patrick Soon-Shiong posted from Athens.
Eleven hours later, Marty Makary was reportedly being fired.
Vinay Prasad is already gone.
Patrick Soon-Shiong is still posting.
Do no harm.
$IBRX Somewhere in a clinic today, a 60-year-old and a 70-year-old are getting routine bloodwork.
Both will get the same lab values back. One of them will be dead in ten years. The other will not.
The difference is not their age. It is their immune system.
That sentence is not opinion. It is a finding from a 31,178-patient study published in JAMA Network Open in 2019. Patrick Soon-Shiong cited the paper yesterday. He led with the conservative number. The buried lead is much darker.
THE 16x
The paper built a simple risk score from three commonly-measured blood markers - lymphocyte count, CRP (C-reactive protein), and RDW (red cell distribution width). Each is a single number from a routine blood draw.
Across the 31,178 participants, ten-year mortality ranged from 3.8% to 62.1%.
A 16-fold spread.
Same country. Same decade. Three numbers from a basic blood panel.
The lowest-risk profile carried 4.0% mortality. The highest-risk profile carried 62.0%. And the highest-risk profile is not rare. It applies to 19.3% of the US adult population. That is roughly twice as common as type 2 diabetes.
Diabetes gets attention. The thing that is twice as common, and several times more deadly, gets none.
THE PAPER
Zidar et al. JAMA Network Open, December 2019.
Soon-Shiong led with this number, age- and sex-adjusted: severe lymphopenia (lymphocytes below 1,000) tracks with 1.8x all-cause mortality.
The cause-specific univariate hazard ratios at severe lymphopenia, in the same paper, are these:
- 7.0x mortality from influenza and pneumonia
- 4.0x mortality from cardiovascular disease
- 3.0x mortality from cancer
One immune signal across three of the largest mortality categories in US adults.
This was on the public record in 2019. Six years before yesterday's tweet.
In 2026, Aditya Bardia at UCLA presented AACR Abstract 5418 - 28,742 breast cancer patients - showing the same association in a different decade by a different team in a different population. Post-COVID lymphopenia tracked with a 2.46-fold increase in distant recurrence (p=0.009).
Two papers. Two populations. Two decades. One finding.
THE THYMUS
The Zidar paper measures lymphocytes in the bloodstream. The lymphocytes do not appear there from nowhere. They are made in an organ most adults could not draw on a chest diagram.
The thymus.
Tucked behind the breastbone, above the heart. In a newborn it is the size of a small fist. In a healthy 70-year-old it has shrunk to a flake of fat.
The thymus is the school where T cells are trained. T cells are the cells the Zidar paper measures. They are the cells the four mortality multipliers - 7x infectious, 4x cardiovascular, 3x cancer - are produced by losing.
The growth factor that drives T cell production and survival is called interleukin-15. IL-15. The same cytokine that lives at the center of every Soon-Shiong post.
A 2023 study in the New England Journal of Medicine found that adults whose thymus was surgically removed had a markedly higher rate of all-cause mortality than those whose thymus was left intact (Kooshesh et al, NEJM 389:406-417). The "useless" organ taken out during cardiac surgery for sixty years is the organ that determines whether a 60-year-old outlives a 70-year-old.
The thymus shrinks. The T cells go with it. The mortality multipliers come due.
This is what @DrPatrick was doing yesterday with one image of a glowing thymus and a question at the bottom: "Are the dots connecting that ALC matters?" He drew the line from the disappearing organ to the disappearing cells to the disappearing decade of life.
The line was already there in JAMA in 2019.
THE TWO ARMIES
The immune system has two arms.
The first is innate. Natural killer cells - NK cells - patrol the bloodstream looking for cells that are sick, infected, or transforming into cancer. They kill on contact. No memory. No license. They are the immune system's first responders.
The first photographs of what would later be named natural killer cells were taken in 1969 by Joseph Sinkovics at MD Anderson. He drew his own blood, isolated the lymphocytes, and watched them kill cancer cells in a petri dish. The NCI canceled his grant. They called the killing "an in vitro artifact." Soon-Shiong has cited Sinkovics's 1969 photographs publicly as the origin of his work.
The second arm is adaptive. T cells learn. Once trained, they remember the threats they have seen. Memory T cells live for decades.
NK cells and memory T cells together cover both axes of immune defense. The fast unlearned kill, and the slow durable memory. Most cancer drugs work primarily on one arm. ANKTIVA expands both in the same patient at the same time.
The cytokine that drives both expansions is IL-15.
In 2007 the National Cancer Institute hosted a workshop reviewing 124 immunotherapy agents and ranking them by potential to impact cancer mortality. IL-15 was ranked #1. The ranking was published. The grants did not follow. Seventeen years passed.
In 2024 the FDA approved the first IL-15 superagonist for human use. ANKTIVA. Both arms of the immune system, restored.
This is the dot the regulators kept losing.
THE BIOLOGY
The Zidar paper does not name a drug. But it does name the mechanism.
It says four things destroy circulating T cells: TNF-alpha. IL-1-beta. Cortisol. Catecholamines.
The cellular mechanism it names is apoptosis - programmed cell death - and redistribution out of the bloodstream.
That is the disease. Stress cytokines kill T cells. Lymphopenia is what dying T cells leave behind. The mortality multipliers are what lymphopenia produces.
The reverse mechanism is also published. Alpdogan et al, in Blood, 2005, showed IL-15 administered to bone marrow transplant recipients did the precise opposite: less T cell apoptosis, more Bcl-2 (the anti-apoptotic protein), more proliferation. T cells came back. So did NK cells. So did NK T cells.
Wrangle et al, in Lancet Oncology, 2018, showed the same effect in human lung cancer patients receiving an IL-15 superagonist called ALT-803. Statistically significant expansion of NK cells. Statistically significant expansion of CD8+ T cells. Documented in patients since 2018.
ALT-803 is the molecule the FDA later approved as ANKTIVA, in April 2024, on the strength of a 71% complete response rate in BCG-unresponsive bladder cancer (Chamie et al, NEJM Evidence, 2023). Median duration of response: 26.6 months. 89.2% probability of avoiding cystectomy at 24 months. 100% disease-specific survival at 24 months.
The reason a complete response from ANKTIVA lasts 26.6 months is not just the T cell expansion. It is the kind of T cells. IL-15 specifically expands memory T cell populations - the long-lived cells that maintain immunity over time and patrol for cancer cells they have already encountered.
The cytokines that destroy T cells. The cytokine that brings them back. The cytokine that makes the new ones remember. All on the public record. All for years.
THE LONGEVITY CASE
Soon-Shiong's framing yesterday was not "cancer drug." It was three words: "cancer + longevity + sepsis."
The longevity word matters because the science is in the Zidar paper itself.
A 70-year-old with a low-risk immune profile had 74.1% ten-year survival in the cohort. A 60-year-old with a high-risk immune profile had 68.9%.
A decade of age was less determinative than the immune profile.
Saudi Arabia has spent the last several years building one of the largest longevity research programs in the world. The Hevolution Foundation, headquartered in Riyadh and launched in 2021, deploys substantial annual funding for healthspan research and hosts the Global Healthspan Summit, which ran in Riyadh in 2024 and 2025.
In May 2025, Patrick Soon-Shiong launched the Cancer BioShield platform inside that ecosystem. He met MBS. He signed MOUs with King Faisal Specialist Hospital and the King Abdullah International Medical Research Center. In January 2026 the Saudi FDA approved ANKTIVA for two indications - bladder cancer and metastatic non-small cell lung cancer with checkpoint inhibitors. Saudi Arabia is now the only jurisdiction on earth where ANKTIVA is approved for a second indication.
The country with one of the largest longevity research programs on the planet has approved the only FDA-approved IL-15 superagonist for two indications. They began commercial launch on April 21.
THE PATIENT
The mechanism is one thing. A real patient is another.
In 2026, Hammond et al published in Clinical Immunology Communications a single-patient case report on a critically ill ICU patient with refractory Coccidioides pneumonia and secondary Pseudomonas pneumonia. Standard antifungal and antimicrobial therapy had failed for thirty days.
The patient received emergency investigational immunotherapy with N-803 (ANKTIVA) plus invariant NK T cells - a third immune lineage that combines features of both NK cells and T cells. Within eight days, Pseudomonas counts in lung lavage dropped from 100,000 colony-forming units to 10. A 10,000-fold reduction. The bronchoalveolar lavage immune infiltrate went from sparse on Day 1 to roughly 1,500 cells per microliter on Day 7.
Pathogen control was real. The mechanism worked. Documented in a peer-reviewed journal.
That is the 7x infectious-disease number translated into measured response. Not a forecast. A documented case.
THE SCALE
Soon-Shiong's framing yesterday: 52 million Americans suffer from low T cells.
That number is an extrapolation. It comes from the 20.1% of the Zidar cohort with relative lymphopenia, applied to the US adult population. The math is defensible. The figure is not paper-stated.
What is paper-stated is heavier:
If 19.3% of US adults carry the highest-risk immune profile, that is roughly 50 million people. They are walking around. Their bloodwork is on file with their primary care physicians. The risk score takes thirty seconds to compute.
The math is not the bottleneck. The math has been on the public record since December 2019.
THE BUILD
The day Soon-Shiong endorsed Zidar, his company also pre-announced the AUA 2026 slate. Two indirect treatment comparisons of ANKTIVA versus the only two FDA-approved alternatives in the same indication. The randomized BCG-naive registrational trial gets a status update. Saturday May 16, Soon-Shiong presents personally on "The Role of IL-15 in the Urological Setting."
That evening, he posted a photograph of an industrial floor full of robotic arms and aseptic isolators - the world's first NK cell manufacturing robot, in production, delivery this month.
The medicine is being built at scale. The data is being filed at the FDA. The papillary sBLA filing-acceptance window is May 8 through May 12. The AUA presentations follow May 15 through 18.
This week, two binary catalysts.
THE STAKES
By April 2026, ANKTIVA was approved in 34 countries - the US in April 2024, then the UK, Saudi Arabia, the European Union, and Macau (the first Asian jurisdiction).
In the United States it is approved for one indication. ImmunityBio reported 3,745 ANKTIVA unit sales for full-year 2025 - the entire approved-indication US deployment.
The papillary expansion sBLA is at the FDA right now. Six days ago Vinay Prasad - the man who spent nine years fighting Soon-Shiong and was given the keys to CBER on May 6 last year by his friend Marty Makary - walked out the door.
THE QUESTION
NK cells were photographed killing cancer in 1969. The NCI called the killing an artifact.
IL-15 was discovered in 1994. The NCI ranked it #1 in 2007.
ANKTIVA was approved in 2024.
Fifty-five years between Sinkovics drawing his own blood and the FDA approving the first IL-15 superagonist for human use.
The mechanism is on the public record. The drug is on the public record. The patients are on the public record. The factory is on the public record.
The question is no longer whether the science is real.
The question is whether the door opens.
One year ago today, Vinay Prasad was given the keys to CBER, the FDA division that regulates this drug.
Named to the seat by his friend Marty Makary.
The man who called Patrick Soon-Shiong miniscule. Vague. Snake oil. A me-too drug seller.
For nine years.
While Soon-Shiong was building the medicine to save millions of lives.
Six days ago, Prasad was gone.
Today, the founder he spent nine years trying to bury posted three words.
Global expansion. Unstoppable.
Prasad got the keys. Soon-Shiong got the world.
https://t.co/2dlmQc7JaI
FDA Commissioner Marty Makary appointed his longtime podcast friend Vinay Prasad to regulate life-saving medicines. The man who had spent years publicly attacking the FDA, the people running it, and the scientists building cures was now in charge.
The friend had publicly called @DrPatrick a snake oil salesman, called Peter Marks a [BLEEP] regulator, mocked RFK Jr., and trashed three former FDA Commissioners.
He was given the keys anyway.
THE SCENE
On October 31, 2024, on the VPZD Show, Vinay Prasad and Zubin Damania were discussing news that Patrick Soon-Shiong was in private talks with Donald Trump for a health advisory role.
Vinay Prasad: "He's in private talks with Trump to like sit in some advisory role, because that dude is always a snake oil"
Zubin Damania, nearly simultaneously: "He's a snake oil salesman."
Source: https://t.co/5oL5WFFKdr
Six months and six days later, Vinay Prasad's friend Marty Makary appointed Vinay Prasad to head the FDA division that regulates Patrick Soon-Shiong's drugs.
Patrick Soon-Shiong has been silent on $IBRX since April 27, 2026. For a CEO who normally posts multiple times a day, eight days of silence is loud.
This is the file the silence sits on top of.
THE FRIENDSHIP, IN HIS OWN WORDS
On December 29, 2024, two months after the snake oil exchange, Vinay Prasad stood in front of a UCSF Hematology Oncology Interest Group and said this:
"My friend Marty Macri is gonna be the new commissioner. So that's good news for me."
He paused, then self-corrected: "No, it's good news for Marty. It's good news for all of us."
Four months later, his friend Marty Makary appointed him to head the FDA division that regulates Patrick Soon-Shiong's drugs.
Source: https://t.co/jwoyiWorM3 (audio at 35:00)
THE PARTNERSHIP
Marty Makary was not an occasional guest. He was a recurring voice on the Vinay Prasad and Zubin Damania podcast network for five years.
Between 2019 and late 2024, Makary appeared on at least 18 documented episodes across the network:
- 3 VPZD Show episodes co-hosted by Prasad and Damania - #4 "Omicron Panic" (late 2021/early 2022), #33 "Marty's Book" (Sept-Nov 2024), #34 "Blind Spots" (Sept-Nov 2024)
- 15 ZDoggMD episodes featuring Makary as guest, spanning 2019 through 2024 (one of which also featured Prasad)
- Sensible Medicine Substack cross-promotion as part of the same network
The podcasts drove paid subscribers to Vinay Prasad's drvinayprasad . com Substack and to Zubin Damania's Substack. Makary's books got dedicated promotional episodes on the network - notably VPZD Show #34 "Blind Spots" in late 2024, devoted to his then-new bestseller.
This is the network where Vinay Prasad called Patrick Soon-Shiong a snake oil salesman on October 31, 2024, where Vinay Prasad ratified Damania's same framing in the same breath, and where Vinay Prasad called Peter Marks a [BLEEP] drug regulator two weeks later.
None of it was illegal. None of it required formal disclosure under federal ethics rules at the time. All of it was on the public record at the time of Makary's nomination on November 22, 2024 and at the time Makary appointed Prasad to CBER on May 6, 2025.
On November 26, 2024, four days after Donald Trump nominated Makary as FDA Commissioner, Vinay Prasad posted a video to his YouTube channel titled "I endorse Marty Makary for FDA commish! Here is why!" Source: https://t.co/XkakfAUG5t
In that same video, at the 16:35 mark, Prasad said this about Peter Marks, the sitting CBER director Prasad would replace five and a half months later: "I hope Peter Marks gets the same treatment that he gave Marion Gruber and Phil Kraus. The same broom closet he can get reassigned to."
Source with timestamp: https://t.co/1Wwt0EXgt3
HOW DOES THIS HAPPEN
Vinay Prasad mocked RFK Jr. as a "rando guy who tells stories about bears." He called Peter Marks a [BLEEP] drug regulator. He attacked the last three FDA Commissioners by name - Califf, Gottlieb, Hahn. He called Patrick Soon-Shiong a snake oil salesman.
Six months later, Marty Makary handed Prasad the keys to the FDA division that regulates Patrick Soon-Shiong's drugs. Patrick Soon-Shiong has no recourse. Marty Makary and Vinay Prasad had been on the same podcast circuit for five years.
This is the record Marty Makary saw. He made the appointment anyway.
THE RECORD ON PATRICK SOON-SHIONG
Vinay Prasad has been attacking Patrick Soon-Shiong by name for nine years.
February 14, 2017. STAT News investigation by Adam Feuerstein and Damian Garde. Prasad on Soon-Shiong's NK-cell trial in Merkel cell carcinoma:
"The clinical breakthroughs touted by Patrick Soon-Shiong are less than modest - they are the most miniscule and vague findings."
Source: https://t.co/UMNMrgRTrl
This is not just an attack on a CEO. It is an attack on a molecule.
THE WAR ON IL-15
In 2007, the National Cancer Institute ranked 124 immune-modulating molecules by potential to cure cancer.
Number one was interleukin-15 - IL-15. The body's own signal to grow and activate NK cells and T cells. Discovered at the NIH.
Number two was Keytruda, Merck's blockbuster checkpoint inhibitor.
Nobody built IL-15 into a drug for almost two decades. Patrick Soon-Shiong did. The result was ANKTIVA, an engineered IL-15 superagonist that rebuilds the immune system rather than taking the brakes off the way Keytruda does. FDA approved it April 2024 for BCG-unresponsive bladder cancer. Saudi Arabia approved it for advanced lung cancer. Published research has extended IL-15 to sepsis, pancreatic, breast, head-and-neck, HIV, and radiation injury.
Vinay Prasad attacked the NK-cell trial in 2017 (STAT). He attacked the regulatory pathway in 2021 (JAMA Oncology - https://t.co/Qwfz5Xk5lo). He attacked the man in 2024 (his own YouTube channel).
He attacked the molecule the NIH ranked first. Then he was given the office that regulates it.
THE RECENT ATTACKS
October 28, 2024. On his YouTube channel, Prasad on Soon-Shiong's primary commercial drug Abraxane, at the 3:32 mark:
"His me too drug was marketed as Abraxane as a better alternative to the older drug, but it's actually not better. In multiple head-to-head randomized control trials, it fails to outperform Paclitaxel, most famously Rugo et al in 2015 in breast cancer when they dose on the same schedule. So I actually don't think Abraxane was ever worth that kind of money. It has a very narrow use, which is you can skip some steroid premedication. Okay, anyway, that's how he got his money."
Source: https://t.co/TfOnwm3Da8
October 31, 2024. On the VPZD show episode 36, the conversation turns to Patrick Soon-Shiong being in private talks with Donald Trump for a health advisory role. At the 1:23:52 mark, Vinay Prasad says: "He's in private talks with Trump to like sit in some advisory, because that dude is always a snake oil-" Zubin Damania, nearly simultaneously, completes: "He's a snake oil salesman." Vinay Prasad ratifies with: "That's the thing."
Both men called Patrick Soon-Shiong a snake oil salesman, on a recorded podcast, in the same breath.
Source: https://t.co/5oL5WFFKdr
THE RECORD ON PETER MARKS
PETER MARKS - the man whose CBER seat Prasad would assume on May 6, 2025.
November 14, 2024. On the Sensible Medicine podcast "MAHA and Medical Conservatism." Howard YouTube clip preserves the timestamp at 1:11:
"I expect less from RFK Jr than I do from Peter Marks. Peter Marks is a [BLEEP] drug regulator [BLEEP]ing up every single day."
(The original audio is unredacted. Verbatim source linked below.)
Source: https://t.co/brZS5yVSms
Peter Marks approved ANKTIVA in April 2024. Vinay Prasad publicly attacked him in profanity seven months later. Nearly six months after that, Prasad replaced him.
Recall what Prasad said about Makary's appointment: "good news for me." Peter Marks's fate was on the record five and a half months before his replacement was announced.
THE APPOINTMENT
May 6, 2025. Vinay Prasad named CBER director by Marty Makary.
He took office holding:
- A documented record of attacking IL-15, the molecule the National Cancer Institute ranked first out of 124 immune-modulating molecules in 2007
- Peer-reviewed academic opposition to the regulatory pathway that approved ANKTIVA
- Profanity-laden public hostility toward the predecessor whose seat he was filling
- Sustained personal attacks on Patrick Soon-Shiong dating back nine years
- Public mockery of the HHS Secretary who was now his boss
- Public attacks on the last three FDA Commissioners by name
- A publicly stated friendship with the man who appointed him
Every item above was on the public record when Marty Makary made the appointment.
ONE YEAR, TWO REGULATORY ACTIONS
Vinay Prasad's tenure at CBER ran 360 days, from May 6, 2025 to April 30, 2026. Two regulatory actions bracket that tenure on either end.
May 2, 2025: FDA Refuse to File on the ANKTIVA papillary sBLA. Issued by CBER staff in Peter Marks's last week. Vinay Prasad's name announced four days later.
The four-day gap is a paperwork detail. The friendship was on record since 2019. The hostility toward Patrick Soon-Shiong was on record since 2017. The opposition to the regulatory pathway was on record since 2021. Vinay Prasad arrived inside the office long before his name was on the door.
March 13, 2026: OPDP Warning Letter to ImmunityBio's CEO over claims made by Patrick Soon-Shiong in a Sean Spicer podcast appearance and a TV advertisement. The action came during Vinay Prasad's tenure and followed two prior untitled letters (September 9, 2025 and January 7, 2026) over the same disputed claims.
April 30, 2026: Vinay Prasad's last day at FDA.
WHAT THE RECORD SAYS
The man whose silence we are watching - Patrick Soon-Shiong - is the man who has been called miniscule, vague, snake oil, a me too seller, and the source of money he didn't deserve.
The man who said those things about him - Vinay Prasad - was given the keys to the FDA division that regulates his drugs by his friend Marty Makary.
Every line above is on file.
Vinay Prasad was given the keys. Patrick Soon-Shiong was given silence.
$IBRX It's time to get the answers.
@DrPatrick has been silent for five days. No original IBRX or ANKTIVA posts since April 27. For a CEO who normally posts multiple times a day, that is uncharacteristic.
But silence cuts both directions. And the record over the last twelve months has not moved an inch.
One year ago today, May 2, 2025, FDA refused to file the papillary sBLA. The stock hit $1.83 five days later. The company was hauled into class actions. Short interest sat near 40% of the float. The story was over, except it wasn't.
THE BASE RATE
JAMA Internal Medicine, 2021. 98 FDA Refuse to File letters studied. 72% of resubmissions were eventually approved.
That number is not a promise. It is a base rate. It says the agency, given a second look at the same drug from the same company with tighter data, says yes more than two times in three.
THE TWO COHORTS
The pivotal trial is QUILT-3.032. Open-label, single-arm, multicenter. It enrolled two main patient groups, both with BCG-unresponsive non-muscle-invasive bladder cancer.
Cohort A: patients with carcinoma in situ (CIS), the flat form. Some of these patients also had papillary tumors. This cohort produced the April 2024 approval.
Cohort B: patients with papillary tumors only, no CIS, the raised form. This is what the resubmission asks FDA to add.
Same drug. Same trial. Same delivery into the bladder. Same disease setting. The only difference is which form of the cancer the patient presented with.
In April 2024, FDA approved ANKTIVA out of Cohort A on single-arm data. That approval anchors the US commercial business: 240M+ covered lives, permanent J-code, over a year of real-world use. International approvals and launches stack on top of it, not in place of it.
The current resubmission asks FDA to extend that approval to Cohort B - on single-arm data from the same trial.
That is the actual heart of the May 2, 2025 RTF: FDA approved single-arm data for one cohort and refused to file single-arm data from the other cohort of the same trial twelve months later. Same drug. Same trial. Same trial design. Different patient subgroup of the same disease.
WHY NOT THE FIRST TIME?
A fair question. Three answers.
First: alignment. The original sBLA was filed under FDA leadership's explicit instruction, on the data the company had at the time. The reviewers refused without having articulated their own bar. The Type B end-of-phase meeting on January 20, 2026 finally surfaced FDA's specific concerns. ImmunityBio submitted additional data in February per FDA's requests and formally resubmitted in March. The agency finally defined the bar. The company met it. The 2025 application could not address questions the agency had not yet asked.
Second: the original RTF was a procedural reversal, not a science failure. January 2025, an in-person meeting with CBER, CDER, and OCE leadership unanimously instructed ImmunityBio to submit on the single-arm data they had at that moment. They did. Then the review-team refused to file on grounds leadership had already cleared. A former senior FDA official, Rachel Sherman, publicly called the RTF "regulatory inaccuracies."
Third: the world changed. Saudi did not exist on the original submission day. The EU Conditional Marketing Authorization did not exist. UK MHRA had not yet approved. Macau had not yet approved. NCCN had not yet listed. A full year of real-world U.S. commercial use had not yet accumulated.
The 2026 resubmission is not the 2025 application with more pages stapled to the back. It is a different submission, into a different agency, in a different world.
THE LEADERSHIP HAS TURNED OVER
When the RTF was issued on May 2, 2025, CBER was between directors. Peter Marks had resigned in March 2025 citing "assault on scientific truth." Four days after the RTF, Marty Makary named Vinay Prasad to run CBER. Prasad's published philosophy was skeptical of single-arm accelerated approvals.
Six months later, on November 12, 2025, Prasad and Makary co-authored a New England Journal of Medicine paper, "FDA's New Plausible Mechanism Pathway," that established the opposite principle: one trial plus mechanism of action can be sufficient when the biology is clear. They wrote it together.
Prasad's departure was announced March 6, 2026. His last day at FDA was the end of April. Today is May 2, 2026.
The CBER that decides whether to accept this filing is no longer the CBER that issued the RTF.
THE NEW DATA
Type B end-of-phase FDA meeting on January 20, 2026. ImmunityBio brought five years of follow-up to the table.
- 96% disease-specific survival at 36 months. Median survival not yet reached.
- 12-month disease-free survival: 58.2% (95% CI 46.6 - 68.2).
- 12-month progression-free survival: 94.9%.
- 36-month progression-free survival: 83.1%.
- 12-month cystectomy-free survival: 92.2%.
- 36-month cystectomy-free survival: 81.8%.
FDA requested updated efficacy data after the meeting. The company submitted it. FDA acknowledged the resubmission on March 9, 2026.
THE PARALLEL TRACKS
All five international approvals are for the CIS form, the same form FDA approved in April 2024. They validate the drug, the mechanism, and the regulatory category. The papillary resubmission asks FDA to add the second form.
Saudi SFDA approved ANKTIVA in January 2026 for both the CIS form of BCG-unresponsive bladder cancer and second-line non-small-cell lung cancer post-checkpoint. The Saudi NSCLC label cites absolute lymphocyte count as the biomarker tied to overall survival - the only regulator anywhere to write that into a drug label. Commercial launch in Saudi Arabia followed on April 21, 2026.
The European Commission granted Conditional Marketing Authorization on February 16, 2026. Thirty countries.
UK MHRA approved on July 7, 2025.
Macau ISAF approved on March 21, 2026 - the first ANKTIVA approval in Asia.
NCCN, by contrast, did move on the papillary form specifically. NCCN listed ANKTIVA + BCG for papillary disease as Category 2A on March 16, one week after FDA acknowledged the resubmission. NCCN is the guideline most U.S. insurers use for reimbursement decisions. The leading U.S. oncology expert panel endorsed the papillary indication while FDA's own filing review was still underway.
RMAT designation is active throughout.
And separately from this resubmission, the BCG-naive Phase 3 randomized trial - a different and much larger patient population, the upstream first-treatment market - is on track for a planned BLA submission on December 28, 2026. Its independent monitoring committee confirmed statistical power on March 27, 2026. That program is not affected by the May filing-acceptance window. It is the next thing.
STAY CALM
Nobody knows what FDA will decide. Nobody knows what PSS knows. The 60-day filing-acceptance window closes around May 8 to May 12, 2026, depending on the exact resubmission receipt date.
But here is what is true today, on the one-year anniversary of the day the market lost the plot.
The company resubmitting in March 2026 is not the company that got told no in May 2025. Twelve months of work doesn't disappear because the calendar got tense.
The silence isn't the answer. Twelve months of evidence is.














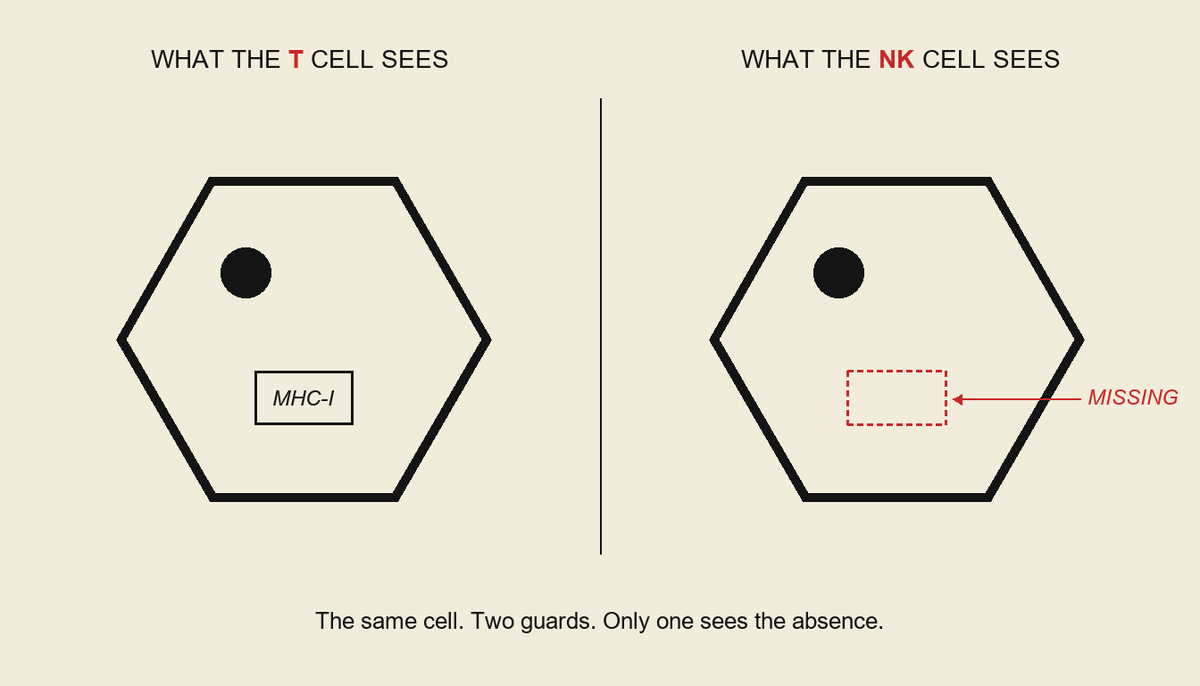



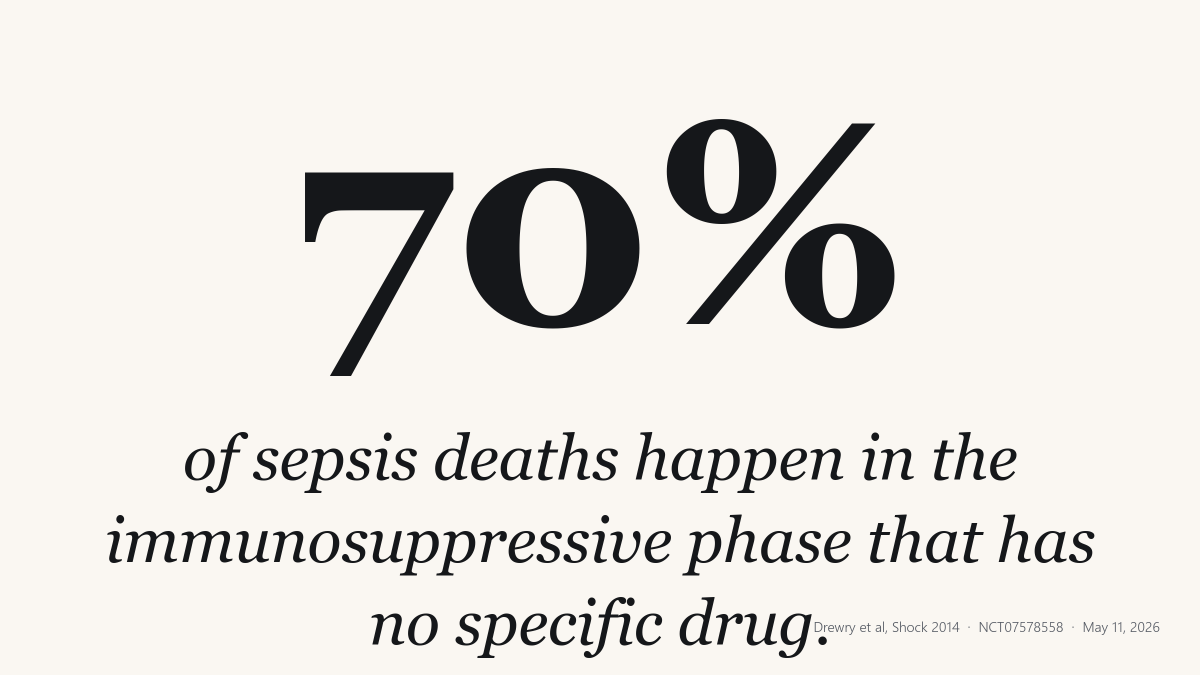



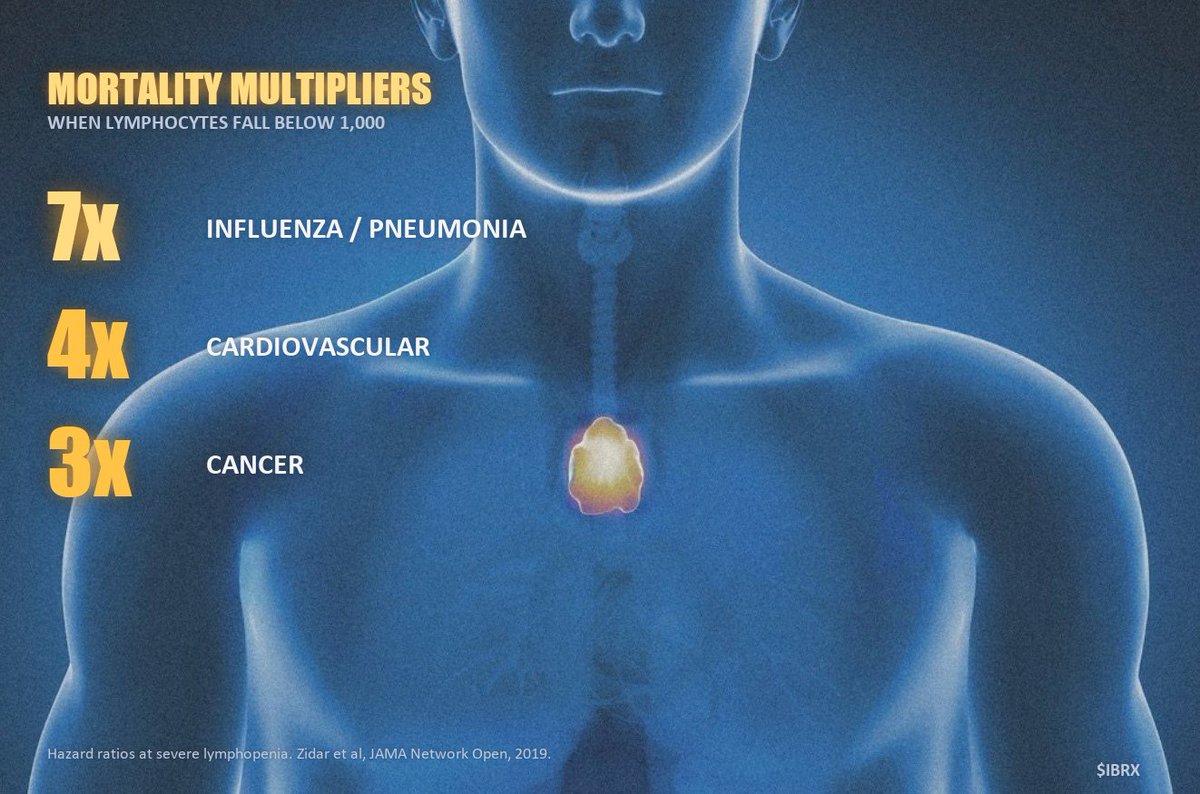
![ActionFixesFear's tweet photo. FDA Commissioner Marty Makary appointed his longtime podcast friend Vinay Prasad to regulate life-saving medicines. The man who had spent years publicly attacking the FDA, the people running it, and the scientists building cures was now in charge.
The friend had publicly called @DrPatrick a snake oil salesman, called Peter Marks a [BLEEP] regulator, mocked RFK Jr., and trashed three former FDA Commissioners.
He was given the keys anyway.
THE SCENE
On October 31, 2024, on the VPZD Show, Vinay Prasad and Zubin Damania were discussing news that Patrick Soon-Shiong was in private talks with Donald Trump for a health advisory role.
Vinay Prasad: "He's in private talks with Trump to like sit in some advisory role, because that dude is always a snake oil"
Zubin Damania, nearly simultaneously: "He's a snake oil salesman."
Source: https://t.co/5oL5WFFKdr
Six months and six days later, Vinay Prasad's friend Marty Makary appointed Vinay Prasad to head the FDA division that regulates Patrick Soon-Shiong's drugs.
Patrick Soon-Shiong has been silent on $IBRX since April 27, 2026. For a CEO who normally posts multiple times a day, eight days of silence is loud.
This is the file the silence sits on top of.
THE FRIENDSHIP, IN HIS OWN WORDS
On December 29, 2024, two months after the snake oil exchange, Vinay Prasad stood in front of a UCSF Hematology Oncology Interest Group and said this:
"My friend Marty Macri is gonna be the new commissioner. So that's good news for me."
He paused, then self-corrected: "No, it's good news for Marty. It's good news for all of us."
Four months later, his friend Marty Makary appointed him to head the FDA division that regulates Patrick Soon-Shiong's drugs.
Source: https://t.co/jwoyiWorM3 (audio at 35:00)
THE PARTNERSHIP
Marty Makary was not an occasional guest. He was a recurring voice on the Vinay Prasad and Zubin Damania podcast network for five years.
Between 2019 and late 2024, Makary appeared on at least 18 documented episodes across the network:
- 3 VPZD Show episodes co-hosted by Prasad and Damania - #4 "Omicron Panic" (late 2021/early 2022), #33 "Marty's Book" (Sept-Nov 2024), #34 "Blind Spots" (Sept-Nov 2024)
- 15 ZDoggMD episodes featuring Makary as guest, spanning 2019 through 2024 (one of which also featured Prasad)
- Sensible Medicine Substack cross-promotion as part of the same network
The podcasts drove paid subscribers to Vinay Prasad's drvinayprasad . com Substack and to Zubin Damania's Substack. Makary's books got dedicated promotional episodes on the network - notably VPZD Show #34 "Blind Spots" in late 2024, devoted to his then-new bestseller.
This is the network where Vinay Prasad called Patrick Soon-Shiong a snake oil salesman on October 31, 2024, where Vinay Prasad ratified Damania's same framing in the same breath, and where Vinay Prasad called Peter Marks a [BLEEP] drug regulator two weeks later.
None of it was illegal. None of it required formal disclosure under federal ethics rules at the time. All of it was on the public record at the time of Makary's nomination on November 22, 2024 and at the time Makary appointed Prasad to CBER on May 6, 2025.
On November 26, 2024, four days after Donald Trump nominated Makary as FDA Commissioner, Vinay Prasad posted a video to his YouTube channel titled "I endorse Marty Makary for FDA commish! Here is why!" Source: https://t.co/XkakfAUG5t
In that same video, at the 16:35 mark, Prasad said this about Peter Marks, the sitting CBER director Prasad would replace five and a half months later: "I hope Peter Marks gets the same treatment that he gave Marion Gruber and Phil Kraus. The same broom closet he can get reassigned to."
Source with timestamp: https://t.co/1Wwt0EXgt3
HOW DOES THIS HAPPEN
Vinay Prasad mocked RFK Jr. as a "rando guy who tells stories about bears." He called Peter Marks a [BLEEP] drug regulator. He attacked the last three FDA Commissioners by name - Califf, Gottlieb, Hahn. He called Patrick Soon-Shiong a snake oil salesman.
Six months later, Marty Makary handed Prasad the keys to the FDA division that regulates Patrick Soon-Shiong's drugs. Patrick Soon-Shiong has no recourse. Marty Makary and Vinay Prasad had been on the same podcast circuit for five years.
This is the record Marty Makary saw. He made the appointment anyway.
THE RECORD ON PATRICK SOON-SHIONG
Vinay Prasad has been attacking Patrick Soon-Shiong by name for nine years.
February 14, 2017. STAT News investigation by Adam Feuerstein and Damian Garde. Prasad on Soon-Shiong's NK-cell trial in Merkel cell carcinoma:
"The clinical breakthroughs touted by Patrick Soon-Shiong are less than modest - they are the most miniscule and vague findings."
Source: https://t.co/UMNMrgRTrl
This is not just an attack on a CEO. It is an attack on a molecule.
THE WAR ON IL-15
In 2007, the National Cancer Institute ranked 124 immune-modulating molecules by potential to cure cancer.
Number one was interleukin-15 - IL-15. The body's own signal to grow and activate NK cells and T cells. Discovered at the NIH.
Number two was Keytruda, Merck's blockbuster checkpoint inhibitor.
Nobody built IL-15 into a drug for almost two decades. Patrick Soon-Shiong did. The result was ANKTIVA, an engineered IL-15 superagonist that rebuilds the immune system rather than taking the brakes off the way Keytruda does. FDA approved it April 2024 for BCG-unresponsive bladder cancer. Saudi Arabia approved it for advanced lung cancer. Published research has extended IL-15 to sepsis, pancreatic, breast, head-and-neck, HIV, and radiation injury.
Vinay Prasad attacked the NK-cell trial in 2017 (STAT). He attacked the regulatory pathway in 2021 (JAMA Oncology - https://t.co/Qwfz5Xk5lo). He attacked the man in 2024 (his own YouTube channel).
He attacked the molecule the NIH ranked first. Then he was given the office that regulates it.
THE RECENT ATTACKS
October 28, 2024. On his YouTube channel, Prasad on Soon-Shiong's primary commercial drug Abraxane, at the 3:32 mark:
"His me too drug was marketed as Abraxane as a better alternative to the older drug, but it's actually not better. In multiple head-to-head randomized control trials, it fails to outperform Paclitaxel, most famously Rugo et al in 2015 in breast cancer when they dose on the same schedule. So I actually don't think Abraxane was ever worth that kind of money. It has a very narrow use, which is you can skip some steroid premedication. Okay, anyway, that's how he got his money."
Source: https://t.co/TfOnwm3Da8
October 31, 2024. On the VPZD show episode 36, the conversation turns to Patrick Soon-Shiong being in private talks with Donald Trump for a health advisory role. At the 1:23:52 mark, Vinay Prasad says: "He's in private talks with Trump to like sit in some advisory, because that dude is always a snake oil-" Zubin Damania, nearly simultaneously, completes: "He's a snake oil salesman." Vinay Prasad ratifies with: "That's the thing."
Both men called Patrick Soon-Shiong a snake oil salesman, on a recorded podcast, in the same breath.
Source: https://t.co/5oL5WFFKdr
THE RECORD ON PETER MARKS
PETER MARKS - the man whose CBER seat Prasad would assume on May 6, 2025.
November 14, 2024. On the Sensible Medicine podcast "MAHA and Medical Conservatism." Howard YouTube clip preserves the timestamp at 1:11:
"I expect less from RFK Jr than I do from Peter Marks. Peter Marks is a [BLEEP] drug regulator [BLEEP]ing up every single day."
(The original audio is unredacted. Verbatim source linked below.)
Source: https://t.co/brZS5yVSms
Peter Marks approved ANKTIVA in April 2024. Vinay Prasad publicly attacked him in profanity seven months later. Nearly six months after that, Prasad replaced him.
Recall what Prasad said about Makary's appointment: "good news for me." Peter Marks's fate was on the record five and a half months before his replacement was announced.
THE APPOINTMENT
May 6, 2025. Vinay Prasad named CBER director by Marty Makary.
He took office holding:
- A documented record of attacking IL-15, the molecule the National Cancer Institute ranked first out of 124 immune-modulating molecules in 2007
- Peer-reviewed academic opposition to the regulatory pathway that approved ANKTIVA
- Profanity-laden public hostility toward the predecessor whose seat he was filling
- Sustained personal attacks on Patrick Soon-Shiong dating back nine years
- Public mockery of the HHS Secretary who was now his boss
- Public attacks on the last three FDA Commissioners by name
- A publicly stated friendship with the man who appointed him
Every item above was on the public record when Marty Makary made the appointment.
ONE YEAR, TWO REGULATORY ACTIONS
Vinay Prasad's tenure at CBER ran 360 days, from May 6, 2025 to April 30, 2026. Two regulatory actions bracket that tenure on either end.
May 2, 2025: FDA Refuse to File on the ANKTIVA papillary sBLA. Issued by CBER staff in Peter Marks's last week. Vinay Prasad's name announced four days later.
The four-day gap is a paperwork detail. The friendship was on record since 2019. The hostility toward Patrick Soon-Shiong was on record since 2017. The opposition to the regulatory pathway was on record since 2021. Vinay Prasad arrived inside the office long before his name was on the door.
March 13, 2026: OPDP Warning Letter to ImmunityBio's CEO over claims made by Patrick Soon-Shiong in a Sean Spicer podcast appearance and a TV advertisement. The action came during Vinay Prasad's tenure and followed two prior untitled letters (September 9, 2025 and January 7, 2026) over the same disputed claims.
April 30, 2026: Vinay Prasad's last day at FDA.
WHAT THE RECORD SAYS
The man whose silence we are watching - Patrick Soon-Shiong - is the man who has been called miniscule, vague, snake oil, a me too seller, and the source of money he didn't deserve.
The man who said those things about him - Vinay Prasad - was given the keys to the FDA division that regulates his drugs by his friend Marty Makary.
Every line above is on file.
Vinay Prasad was given the keys. Patrick Soon-Shiong was given silence.](https://pbs.twimg.com/media/HHgAgCUawAEolM7.jpg)




















