Most people think the psychedelic experience is what heals.
They're wrong.
It's what happens in the days and weeks AFTER that determines everything.
In 2023, Gül Dölen's lab at Johns Hopkins made a discovery that should reshape how every practitioner thinks about their work:
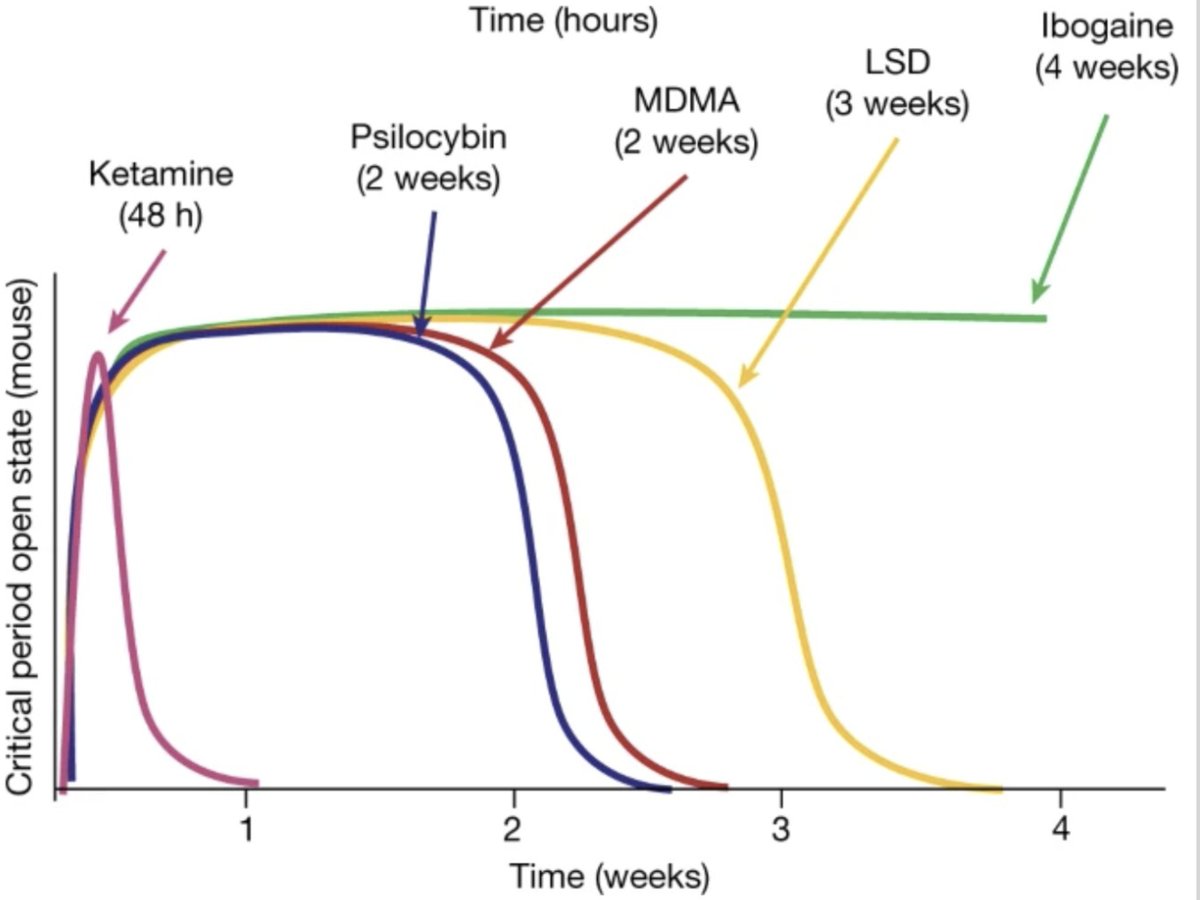
MDMA, psilocybin, LSD, ketamine, and ibogaine all reopen the social reward learning critical period, those rare developmental windows when we learn how to bond, trust, and adapt.
Our brains were once thought to close these windows by age 26. Turns out, psychedelics hand us the key to unlock them again.
Here's what makes this research so compelling:
Different compounds hit different receptors — 5-HT2A, NMDA, KOR — yet they converge on the same outcome: reopening critical learning windows.
It's not the trip that heals. It's the open state.
And each substance opens that window for a different duration:
→ Ketamine ≈ 48 hours
→ Psilocybin ≈ 2 weeks
→ LSD ≈ 3 weeks
→ Ibogaine/5-MeO-DMT ≈ 4 weeks
This isn't chaotic hyperplasticity. It's metaplasticity, a refined readiness to rewire. Dölen's team found oxytocin-mediated changes in the nucleus accumbens and softened extracellular matrix, which basically means the brain's scaffolding loosens so new wiring can stabilize.
Think of it as a biological permission slip for transformation.
But here's what most people miss: this window is time-sensitive.
During the open state, new behavioral habits and secure attachment patterns can take root. Miss the window, and old circuitry reasserts itself. Most people don't realize how critical the days and weeks AFTER a session really are.
This is exactly why we built our Practitioner Training at the Psychedelic Coaching Institute the way we did.
If the medicine opens a window, then the practitioner's job is to help clients make the most of it before it closes.
That means designing protocols around windows, not just sessions. It means mapping dose → duration → practice. Tracking behavior, HRV, mood, and relational change weekly.
The aim isn't to chase peak experiences. It's to facilitate durable rewiring through intentional repetition in the open state.
This is the next era of psychedelic work: utilizing microdosing, nervous system training, and intentional practice to expand the learning window.
The medicine opens it. Your discipline keeps it open. That's how insight becomes identity.
For practitioners ready to work at this level, our next PCI cohort (kicking off February 19!) is where this science meets real-world application.
What are your thoughts on how to design integration around the critical period window?
Two Visions for Psychiatry: The Future of Psychotherapy
A psychiatrist argues "Psychotherapy Training Shouldn’t Be Part of Psychiatry" training; emphasizing the importance of mastering biological skills. He sees psychotherapy as a niche, best left to other professionals.
I see psychotherapy as the core of human connection—a vital tool for understanding patients’ stories, building trust, and fostering healing. It’s not just about symptoms; it’s about meaning, narrative, and living authentically.
Should psychiatrists learn psychotherapy? I think so. IMO, the future of psychiatry depends on integrating science with humanity.
Each new DSM diagnosis (we are at around 370 right now) creates an entirely new market for psych-drug consumption. This is why the drug companies love DSM: it's an ever-reliable driver of profit.
Creemos que ayudando al resto vamos a ayudarnos a nosotros mismos cuando en realidad la mejor forma de ayudar al resto es empezar por ayudarnos a nosotros mismos
@narizdechanch0 Si es el mismo detergente de siempre… Con uña de gato Dice..Y donde están las plantaciones de aloe Vera? La concha de su madre. Si yo ando por todos lados