Thank you to Dr. Dominik C. Benz for his live updates on ATTR-CM from the annual meeting of the Heart Failure Association of the European Society of Cardiology this past weekend! Check out this thread for highlights.
New research in @JAMA_current! As a supporter of the #HCM registry, we are excited for these findings on improving risk prediction of adverse events in HCM patients.
Read more: https://t.co/Tf6MNkkQDD
#CardioX
Special issue this week in @JNCjournal on cardiovascular imaging in amyloidosis!
Congratulations @mdicarli on putting together this essential guide for all things amyloidosis and to @premsoman123 for leading the paper we wrote on state of the art imaging with technetium-labeled tracers like PYP, DPD, HMDP.
https://t.co/AWtosMQwHd
https://t.co/3hcHOoBeKZ
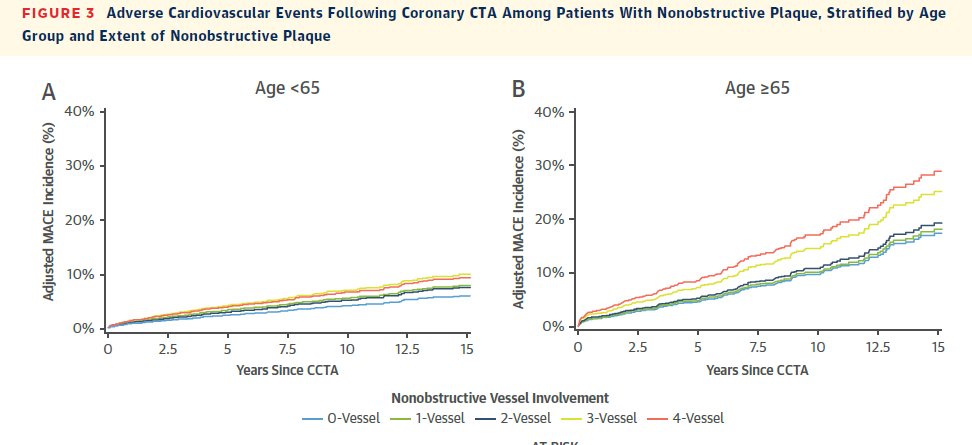
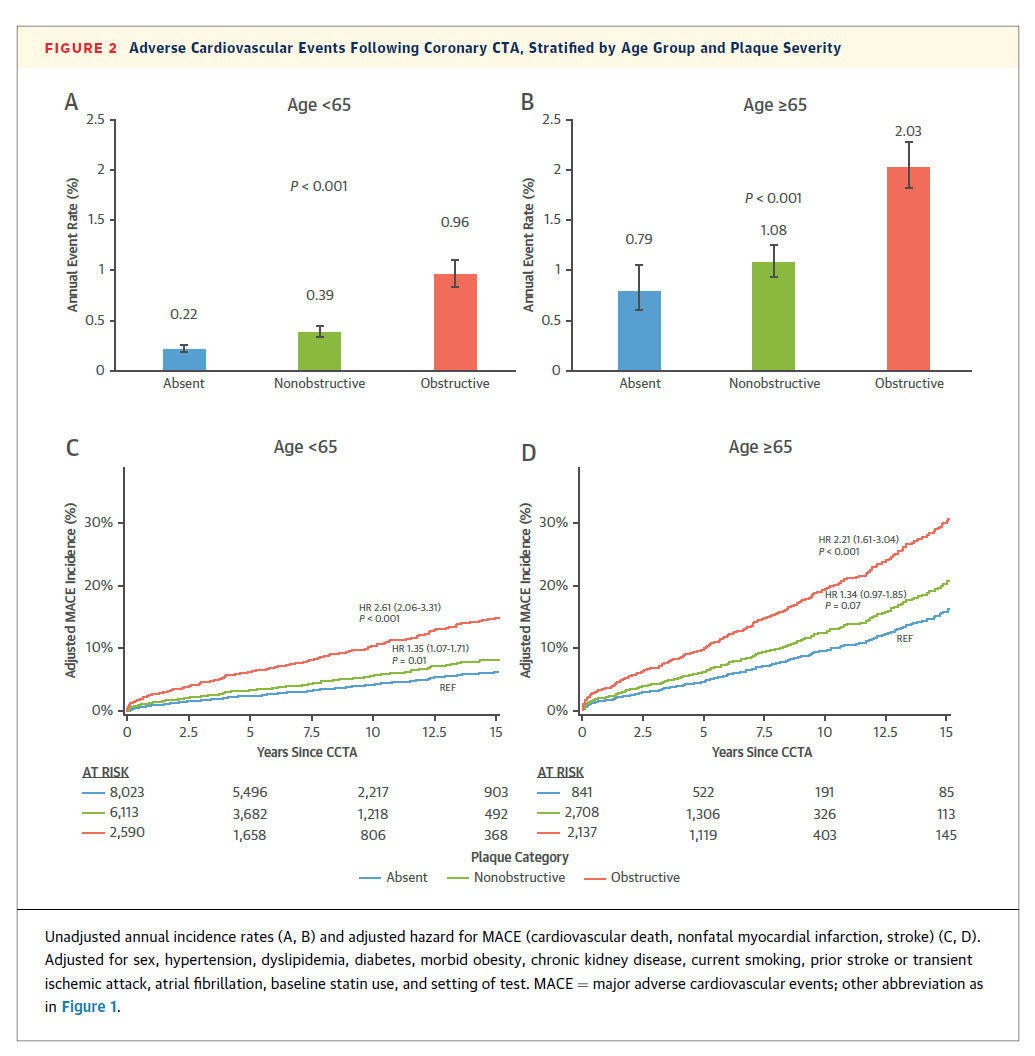
Congrats @DanielMHuck on leading largest & longest F/U @MassGenBrigham#CCTA registry #JACCIMG paper. Motivated by Chest Pain Guideline, we evaluated yield and prognostic implications of CCTA by age, showing value in both younger + older populations 👉https://t.co/CjJD2dwqYB
📄 Low-burden ATTR cardiac amyloidosis: can CMR detect early disease?
🔗 DOI: https://t.co/LPOis036Q0
🫀 Transthyretin cardiac amyloidosis (ATTR-CA) is often diagnosed late—but early detection is critical.
This study focuses on a challenging question:
👉 What does early (low-burden) ATTR look like on CMR—and how do we distinguish it from mimickers?
✨ Study at a glance:
🔹 83 patients with confirmed ATTR-CA
🔹 Stratified by ECV (extracellular volume)
👉 Low burden: ECV ≤43%
🔹 Compared with:
✔ hypertensive heart disease (HHD)
✔ mild hypertrophic cardiomyopathy (HCM)
✨ Key findings:
📊 Low-burden ATTR has a distinct phenotype:
🔹 Often subtle or even normal wall thickness
🔹 Mildly reduced EF (~52%)
🔹 Abnormal strain despite preserved function
👉 As shown in Figure 2 (page 5):
➡️ early disease predominantly affects basal segments
📈 Tissue characterization is the key:
🔹 LGE and ECV outperform strain
➡️ LGE AUC: 0.99
➡️ ECV AUC: 0.97
❗ Strain-based metrics perform significantly worse
⚠️ Why this matters:
👉 Early ATTR can mimic:
HCM
hypertensive LVH
👉 Conventional parameters (wall thickness, EF) are insufficient
➡️ Risk of misdiagnosis or delayed diagnosis
🧠 Unique imaging signature:
✔ Basal predominance of infiltration
✔ Progressive base-to-apex gradient
✔ Increased ECV even with mild phenotype
👉 As illustrated in segmental maps (page 6):
➡️ clear spatial pattern of disease progression
📉 Prognostic insight:
✔ Low-burden ATTR = better survival
❗ But still abnormal biomarkers and imaging
👉 Early stage = window for intervention
💡 Clinical take-home message:
👉 Suspect ATTR even in mild LVH or “atypical HCM”
✔ Use CMR tissue characterization (ECV + LGE)
✔ Do not rely on strain alone
🚨 Bottom line:
Early ATTR is subtle—but CMR tissue characterization can unmask it and differentiate it from hypertrophic mimickers.
#Cardiology #CMR #Amyloidosis #ATTR #CardiacImaging #ECV #LGE #HeartFailure #PrecisionMedicine #EarlyDiagnosis 🫀📊
𝐁𝐑𝐈𝐍𝐆-𝐔𝐏𝟑 𝐒𝐜𝐨𝐦𝐩𝐞𝐧𝐬𝐨: pubblicato su European Journal of Internal Medicine un nuovo articolo dal titolo 𝐷𝑖𝑠𝑐ℎ𝑎𝑟𝑔𝑒 𝑚𝑒𝑑𝑖𝑐𝑎𝑙 𝑡𝑟𝑒𝑎𝑡𝑚𝑒𝑛𝑡 𝑖𝑚𝑝𝑙𝑒𝑚𝑒𝑛𝑡𝑎𝑡𝑖𝑜𝑛 𝑎𝑛𝑑 𝑝𝑟𝑒𝑑𝑖𝑐𝑡𝑜𝑟𝑠 𝑜𝑓 𝑎 𝑠𝑢𝑐𝑐𝑒𝑠𝑠𝑓𝑢𝑙 𝑑𝑒𝑐𝑜𝑛𝑔𝑒𝑠𝑡𝑖𝑜𝑛 𝑖𝑛 𝑝𝑎𝑡𝑖𝑒𝑛𝑡𝑠 𝑤𝑖𝑡ℎ 𝑎𝑐𝑢𝑡𝑒 ℎ𝑒𝑎𝑟𝑡 𝑓𝑎𝑖𝑙𝑢𝑟𝑒: 𝑓𝑖𝑟𝑠𝑡 𝑑𝑎𝑡𝑎 𝑓𝑟𝑜𝑚 𝑡ℎ𝑒 𝐵𝑅𝐼𝑁𝐺-𝑈𝑃 3 𝐻𝑒𝑎𝑟𝑡 𝐹𝑎𝑖𝑙𝑢𝑟𝑒 𝑆𝑡𝑢𝑑𝑦.
Lo studio BRING-UP3 Scompenso promosso da HCF Fondazione ANMCO per il Tuo cuore ETS è stato
disegnato per facilitare l’implementazione delle linee guida nella pratica clinica.
📊𝐋𝐚 𝐩𝐫𝐚𝐭𝐢𝐜𝐚 𝐜𝐚𝐫𝐝𝐢𝐨𝐥𝐨𝐠𝐢𝐜𝐚 𝐢𝐭𝐚𝐥𝐢𝐚𝐧𝐚 𝐜𝐨𝐧𝐭𝐞𝐦𝐩𝐨𝐫𝐚𝐧𝐞𝐚 𝐦𝐨𝐬𝐭𝐫𝐚 𝐮𝐧'𝐞𝐥𝐞𝐯𝐚𝐭𝐚 𝐚𝐝𝐞𝐫𝐞𝐧𝐳𝐚 𝐚𝐥𝐥𝐚 𝐭𝐞𝐫𝐚𝐩𝐢𝐚 𝐟𝐚𝐫𝐦𝐚𝐜𝐨𝐥𝐨𝐠𝐢𝐜𝐚 𝐨𝐭𝐭𝐢𝐦𝐚𝐥𝐞 𝐚𝐥𝐥𝐚 𝐝𝐢𝐦𝐢𝐬𝐬𝐢𝐨𝐧𝐞 in tutto lo spettro della frazione di eiezione nei pazienti con insufficienza cardiaca acuta. Ciononostante, quasi un terzo dei pazienti lascia l'ospedale con congestione residua.
🤝 Le variabili individuate potrebbero aiutare i medici a identificare un profilo di paziente ad alto rischio che richiede strategie decongestionanti ospedaliere più intense e un'assistenza di transizione post-dimissione più aggressiva per ridurre il rischio di riospedalizzazione precoce.
📄 Trovi l’articolo al link : https://t.co/6zyK6Pxbi3
#ANMCO #FondazionePerilTuoCuore #BringUp3Scopmenso
#HFrEF #quattropilastri #fourpillars #ottimizzazione #implementationscience #Cardiologia
#RealWorldData #Ricercaclinica #Miglioramentodellaqualitàdellecure
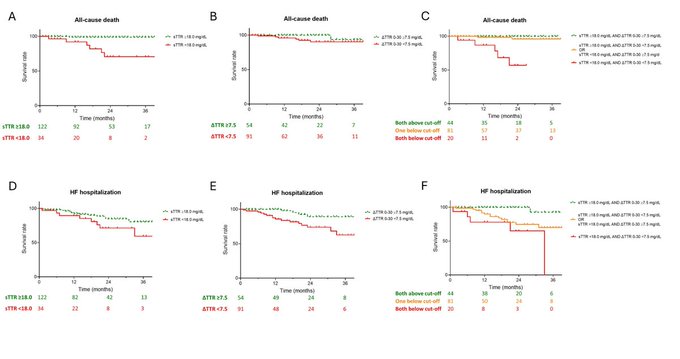
Interesting real-world ATTR-CM data: lower baseline serum TTR and smaller early TTR increases after tafamidis initiation were associated with worse outcomes. @AlbertoAimo90
Potentially relevant for future risk stratification and monitoring strategies.
#HeartFailure26 #MedIQESCHF26
Even if you never care for patients with amyloidosis, there are lessons that will make you a better doctor!
Check out my piece in the special amyloid focus issue of @JCardFail!
https://t.co/Ggxzjugdup
✨ Cascade genetic screening in ATTRv: early diagnosis = better survival ✨
📄 Read the paper here:
💡 A major multicentre study (15 Italian referral centres, >20 years of data) finally quantifies the real clinical impact of cascade genetic screening in hereditary transthyretin amyloidosis (ATTRv).
🔍 Why this matters
ATTRv is a progressive, multisystem disease — often diagnosed too late.
This study shows that screening families is not just diagnostic… it’s prognostic.
📊 Key findings
👨👩👧 Family screening works
– 398 index cases → 1243 relatives screened
– 569 carriers identified (~46%)
⏳ Disease is dynamic
– Among asymptomatic carriers (G+/P−):
→ 16.7% developed disease over ~5 years
⚠️ Earlier than expected
– Some patients developed disease >10 years before predicted onset
🧬 Genotype matters
– Conversion risk varies widely (e.g. Glu89Gln up to 42%)
❤️ The game changer: survival
✔️ Patients diagnosed via screening had ~57% lower mortality vs probands
✔️ Disease-modifying therapy → ~90% mortality reduction
👉 As shown in the survival curves (page 11), screened patients clearly outperform index cases, especially when treated early.
🚨 Take-home message
ATTRv is not a static diagnosis — it’s a continuum.
The earlier you look, the earlier you treat, the better patients do.
🧠 Clinical implications
• Systematic cascade genetic screening should be standard
• Follow-up must be genotype- and family-informed
• Multidisciplinary care (cardio + neuro + genetics) is essential
• Timing of therapy is critical — delay costs survival
🚀 This study moves the field from “should we screen?”
to
👉 “we must screen early and follow closely.”
#Amyloidosis #ATTRv #Genetics #Cardiology #RareDiseases #PrecisionMedicine #HeartFailure #MedTwitter
“More than 6,000 people joined us here at #HeartFailure26, fantastic science, fantastic discussions, & an incredible #HF community.”
Prof. @WilfriedMullens reflects on the remarkable energy & momentum of this year’s congress; and reminds us that the journey continues 🇬🇧
See you in London for #HeartFailure27! 👏
#HFA_ESC @escardio@MarcoMetra@jozinetm
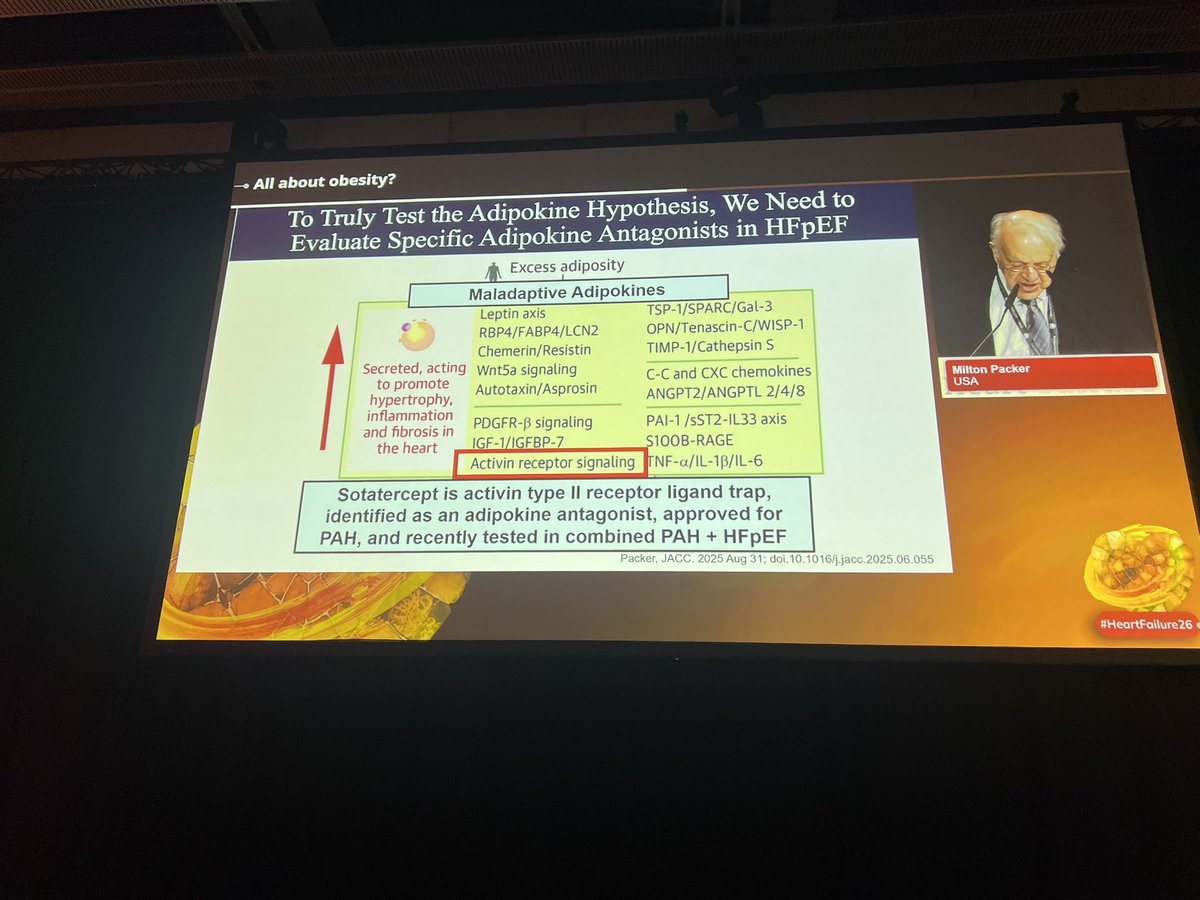
“Fascinating translational perspective from Milton Packer on obesity-related HFpEF:
If maladaptive adipokines drive myocardial hypertrophy, inflammation, and fibrosis, then directly targeting adipokine signaling may become a future therapeutic strategy.
The talk highlighted activin receptor signaling as one potential pathway — with sotatercept (already approved in PAH) emerging as a possible adipokine antagonist under investigation in combined PAH + HFpEF.
This is where HFpEF research is heading:
from hemodynamics alone → toward inflammation, metabolism, and adipose tissue biology. 🫀
The overlap between obesity, pulmonary vascular disease, and HFpEF continues to grow more biologically compelling.
#HFpEF #HeartFailure #Obesity #PulmonaryHypertension #Sotatercept #CardioMetabolic #Cardiology”
#HeartFailure26
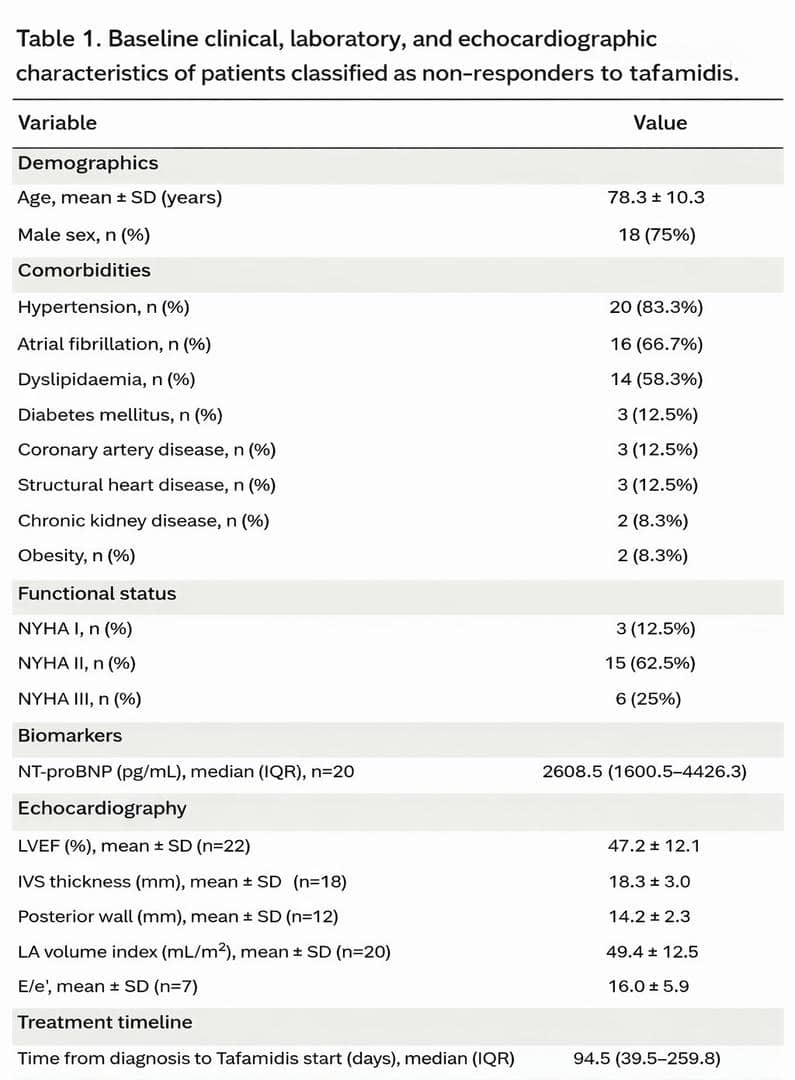
Real-world data suggest substantial heterogeneity in response to tafamidis in ATTR-CM, with nearly half of patients meeting predefined non-response criteria at 12 months.
Highlights the importance of longitudinal monitoring and improved risk stratification.
#HeartFailure26 #MedIQESCHF26
🔥 Ziltivekimab in HF: two trials targeting inflammation | IL-6 ligand inhibitor
Key entry criteria for both: elevated NT-proBNP + CRP ≥2 mg/L + NYHA II-III + echo abnormalities — enriching for inflammatory phenotype
🔵 ATHENA (n=673) — symptoms & function
• Ziltivekimab 15mg SC monthly x 12 months
• Primary endpoint: KCCQ-CSS
• Confirmatory secondary: 6-minute walk distance
🔴 HERMES (n=4900) — events & outcomes
• Event-driven (845 events), min 6-month exposure
• Primary: time to CV death, HFH or urgent HF visit
• Also powered for 4-point composite + CV death + all-cause death
The strategy: ATHENA tests if it makes patients feel better. HERMES tests if it keeps them alive and out of hospital.
Anti-inflammatory therapy in HF — the evidence base is building 🧪
#HeartFailure #Ziltivekimab #ATHENA #HERMES #Inflammation #HFTwitter
#HeartFailure26
A visionary physician, pioneering scientist, & mentor to generations.
Prof. Eugene Braunwald shaped the foundations of modern cardiovascular medicine, from myocardial physiology & haemodynamics to acute coronary care & heart failure.
A moving tribute by Prof. Frank Ruschitzka & Prof. Marc A. Pfeffer in the Heart Failure Association Congress 2026 Braunwald Lecture reminds us that his influence extends far beyond discoveries, through the countless clinicians, scientists, and patients impacted by his legacy.
“Cardiology lost not only a pioneer but its north star.”
➡️https://t.co/XG3zNntDQo
#HeartFailure26
@escardio@MarcoMetra@WilfriedMullens
In ATTRibute-CM, acoramidis attenuated decline in KCCQ-OS versus placebo across multiple pre-specified ATTR-CM subgroups over 30 months.
Interesting data from @dr_m_fontana on health status trajectories and patient-reported outcomes in ATTR-CM.
#HeartFailure26#MedIQESCHF26