🚨 Spectrum, prevalence, and clinical correlates of PPM1D mutations in patients with clonal hematopoiesis and clonal cytopenias.
I am very pleased with this collaborative effort. Grateful to @MrinalPatnaik for his mentorship.
Paper highlights 👇🏽
🧬 PPM1D mutations in clonal hematopoiesis – what really happens after chemo?
Multi center study of 337 CH/CCUS patients dissects how #PPM1D and #TP53 mutations shape therapy-related clonal hematopoiesis. 👇
1️⃣ PPM1D is the signature of therapy-related CH
•50% had PPM1D-mut/TP53-WT
•7% had PPM1D-mut/TP53-mut
•These genotypes were highly enriched in therapy-related CH/CCUS (up to 80% of cases).
2️⃣ All PPM1D mutations were truncating exon-6 variants
Median VAF only 6% — small clones, but biologically meaningful.
3️⃣ Latency after genotoxic therapy was strikingly short
Median time from last chemo/radiation to detection:
•PPM1D-mut groups: ~6 months
•TP53-mut only: ~11 months
•WT/WT: ~24 months
→ PPM1D clones emerge fast after DNA-damaging therapy.
4️⃣ Strong link with PARP inhibitors & radioligand therapy
In therapy-related CH/CCUS:
•PARPi exposure: 24–26% in PPM1D-mut vs 0–3% in WT groups
•Radioligand therapy: ~25–26% in PPM1D-mut vs near-zero otherwise.
5️⃣ Despite this… PPM1D clones rarely progressed
Rates of transformation to MDS/CMML:
•PPM1D-mut/TP53-WT: 2%
•PPM1D-mut/TP53-mut: 4%
•TP53-mut only: 18%
•WT/WT: 12%
AML transformation occurred only in WT/WT group.
6️⃣ When both PPM1D & TP53 are present, neither always “wins”
Among co-mutated patients:
•~⅓ #PPM1D-dominant
•~⅓ #TP53-dominant
•~⅓ co-dominant
Therapy-related CH showed more co-dominant competing clones, suggesting chemo creates a “Darwinian battlefield”.
7️⃣ The size of the PPM1D clone matters
Using ROC-derived cut-off:
•PPM1D VAF ≥13% → independently predicts worse PFS & OS
(HR ~2.3 for both).
Multiple PPM1D mutations ≠ worse outcome — it’s the clone size, not count.
8️⃣ Clinical message
#PPM1D mutations are:
•Common after chemo/PARPi/radioligand therapy
•Often small, fast-emerging clones
•Surprisingly low risk for malignant transformation, even with TP53 —
unless the VAF climbs ≥13%.
Take-home:
PPM1D-mut CH appears to be a therapy-selected, early-emerging, usually indolent precursor state — but rising clone size may signal real danger.
https://t.co/X2dJCu075w
Transplant in the modern-ish era for AdvSM. 1 yr PFS of 74% in the SM-AHN group but only 59% overall. Unclear yet if KIT inhibitors peri-transplant will help improve these outcomes.
British Journal of Haematology | Wiley Online Library https://t.co/W6PBCVAGVB
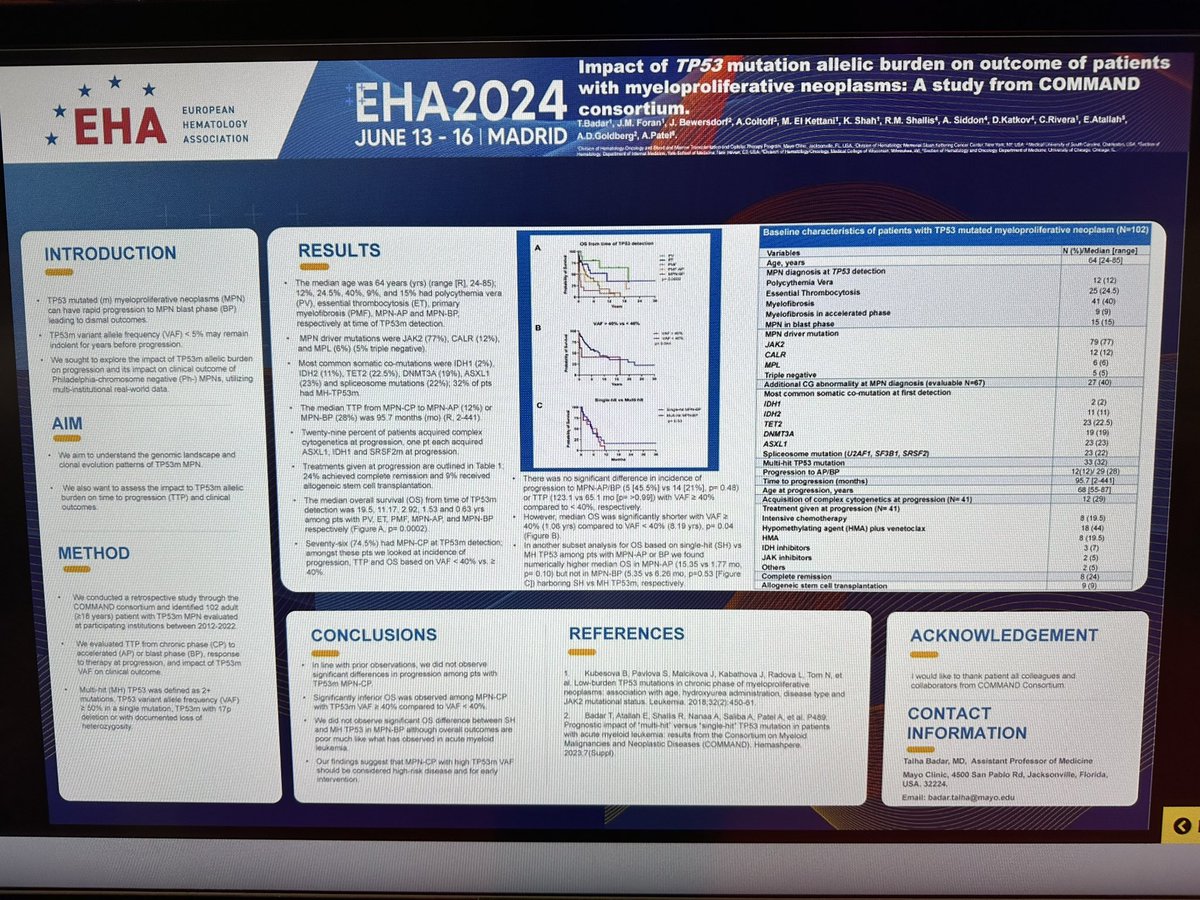
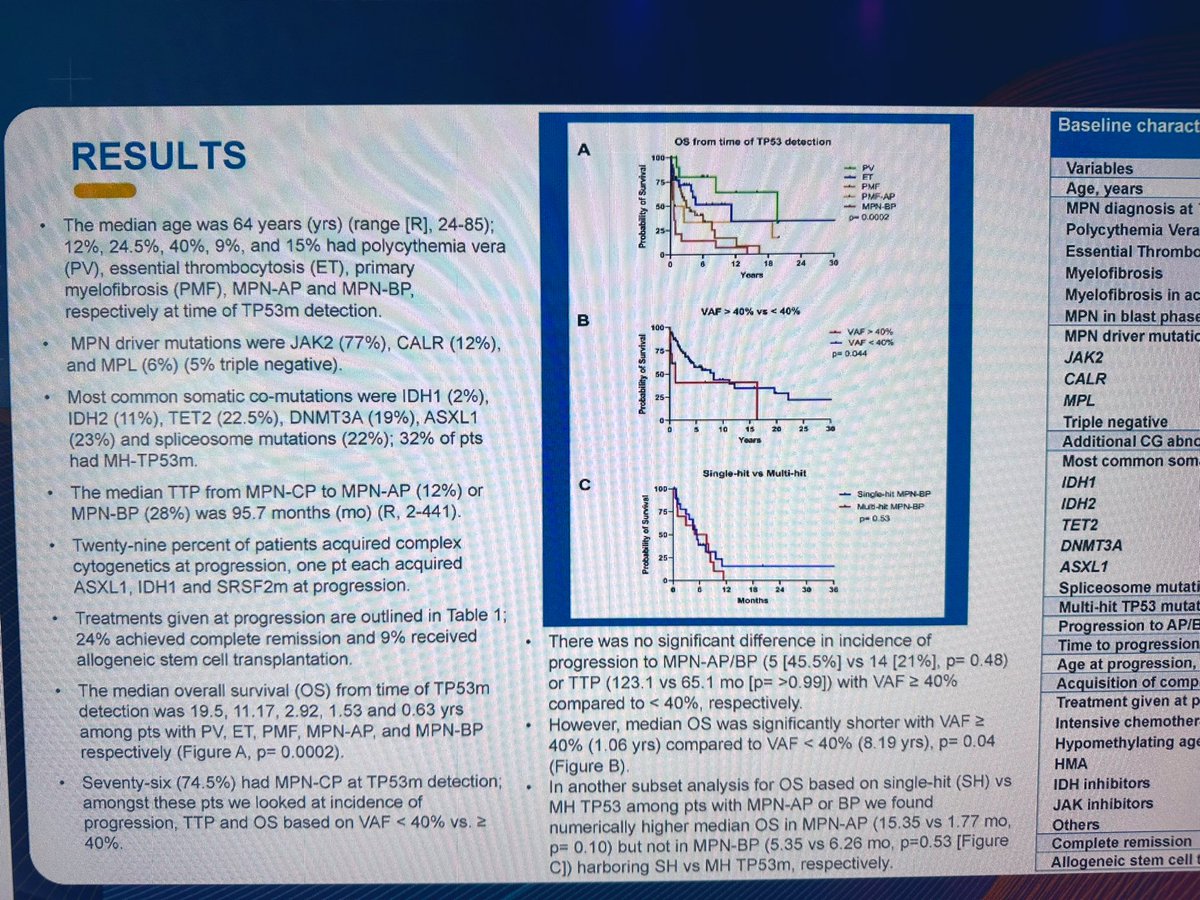
🚨 Latest paper from #COMMAND_consortium, reporting heterogeneity in clinical outcomes in #TP53m MPN, one of largest cohort of TP53m MPN:
1. Multihit TP53 had inferior outcome in chronic phase MPN, not so in MPN-AP or BP. Similar to our reports in HR-MDS/AML.
2. MH TP53 commonly seen in MF or MPN-AP/BP. Rare in PV/ET.
3. Allo-HCT improves outcome, less so with MH TP53/complex CG.
4. TP53 with low VAF commonly seen in PV/ET and does not impact disease progression significantly.
@Dr_RoryShallis@Irumkhan_hem@ChenyuLinMD@AlexColtoff@Anand_88_Patel@Wang_Yu_Hung et al. @MPN_Hub
British Journal of Haematology | Wiley Online Library https://t.co/lfZzBhHDSs
📢 @HOPArx members: one more day to submit your votes to select the next BIG idea‼️Official Votes here: https://t.co/yaW3k3tjLv
Use this poll to see the ✨unofficial✨ spoilers of our colleagues votes🧐
Review of fedratinib with John Mascarenhas. First Downey Jr, then McConaughey - is fedratinib going to have a career renaissance as well?
https://t.co/whurZTJ2LR
Grateful to have presented our experience with Pacritinib and Momelotinib after Ruxolitinib failure in patients with Myelofibrosis @SocietyofHemOnc#SOHO2024 We observed trends toward ⬆️ Hgb, ⬆️ PLT, and ⬇️ in transfusion dependency within 3 months of use #mpnsm#HemOnc
In the latest episode of “PV Pod: Stories from the Marrow,” Dr. Douglas Tremblay from Mount Sinai School of Medicine discusses #PolycythemiaVera (PV) progression and the challenges in predicting and preventing this #RareDisease.
Listen to PV Pod here: https://t.co/AXjS4plSfu
https://t.co/X9WsynX35p
More data regarding clinical and prognostic utility of D14 marrows. Most interesting to me was 63% of pts with RD at D14 had CR at count recovery. Personally, I almost never re-induce on D14 for good-risk and even hesitate for most intermediate-risk.
https://t.co/ZwltbhvRyC
- 84 AML pts stopped VEN (55%) or HMA+VEN (45%)
- Median f/u 23 mos, only pts off tx for 3+ mos included
- mOS 44 mos, mTFS 16 mos (whole cohort)
- mOS 19 mos, mTFS 10 mos (R/R)
- NPM1 MRD- (only 7 pts) 2-year OS 100%
- Very selected pop, but encouraging
https://t.co/QL99syOudN
ARES
- ET randomized 1:1 asa qd vs bid
- Decrease in TXB2 with bid - no difference in thrombosis (to be expected with 20 mo f/u)
- Some symptoms better w/bid, but open-label and all pts on asa at start (role for step-wise asa escalation for sx control?)
#EHA2024#EHA24#poster_session#TP53m#MPN#mpnsm
Genomic landscape, impact allelic burden, time to progression from CP-AP/BP in TP53m MPN—> AML
TP53m with VAF>40 had poorer outcome.
No significant impact of type of induction on outcome.
Special thanks to #COMMAND_consortium @MobasherK@Anand_88_Patel@Dr_RoryShallis #Jan_Bewersdorf #Ehab_Atallah #Aron_Goldberg #Kashish_Shah #Alex_Coltoff
Landmark Paper: the study published in 1998 by Bloomfield et al. established the standard for consolidation therapy in acute myeloid leukemia patients with core binding factor abnormalities.
https://t.co/w2cZOPNNNz